
Abstract
Spontaneous iliac vein rupture (SIVR) is extremely rare and can lead to serious complications, including death. Etiologies include inflammatory processes and hormonal and mechanical triggers, with concomitant May–Thurner syndrome (MTS) being a rare cause. Management can be challenging due to the difficult balance between reducing thrombotic burden and life-threatening hemorrhage that can result from aggressive anticoagulation. Furthermore, surgical interventions are associated with high mortality, making conservative management more desirable. We report a case of SIVR with retroperitoneal hematoma and concurrent MTS that was successfully managed using conservative measures. We further provide a narrative review of the current literature addressing the diagnosis, management, and outcome of SIVR focusing on cases with concurrent MTS.
Case vignette
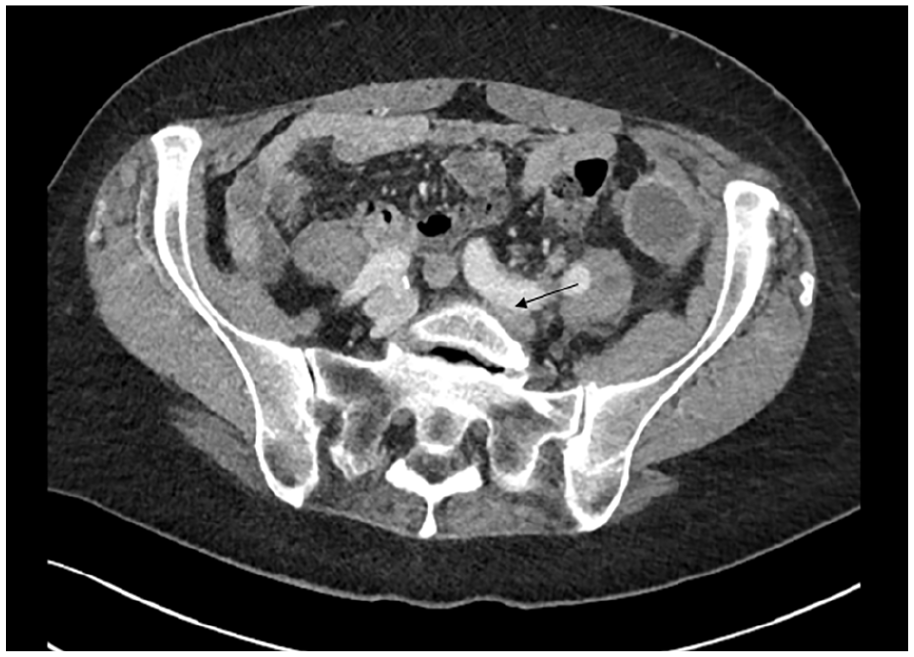
A 71-year-old woman with a history of hypertension presented with sudden onset left-sided abdominal pain and lightheadedness. She was found to be hypotensive (60 mmHg systolic), pale, mildly confused, and unable to move her left leg. Relevant work-up revealed a hemoglobin (Hgb) of 6 g/dL, and a computed tomography angiogram (CTA) showed a large retroperitoneal hemorrhage within the left lower abdomen and pelvis involving the left psoas muscle with compression of the left common iliac vein between the left common iliac artery and the vertebral body (Figure 1). Venous Doppler ultrasound revealed extensive left lower-extremity deep vein thrombosis (DVT) extending from the left external iliac to the popliteal vein (Figure 2). A catheter-based venogram confirmed the presence of thrombus throughout the popliteal, femoral, common femoral, and external iliac veins with active extravasation arising from near the confluence of the left common and external iliac veins (Figure 3A). In addition, there was evidence of May–Thurner syndrome (MTS) based on left common iliac vein stricture and cross-pelvic collaterals (Figure 3B). Careful review of the patient’s history and clinical presentation as well as analysis of laboratory and imaging findings led us to believe that our patient had spontaneous iliac vein rupture (SIVR) with concurrent MTS. Owing to the presence of venous collaterals, we speculated that venous thrombosis occurred prior to SIVR, and that MTS was the underlying etiology.
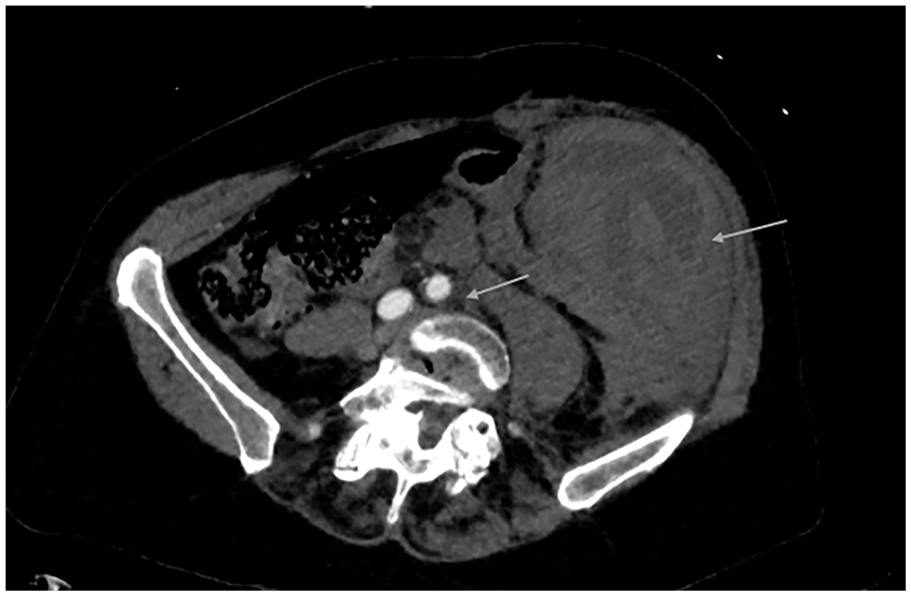
Transverse image of a CTA of the abdomen and pelvis showing a large, left-side retroperitoneal hematoma and left common iliac vein compression between the left common iliac artery and the vertebral body (arrows).
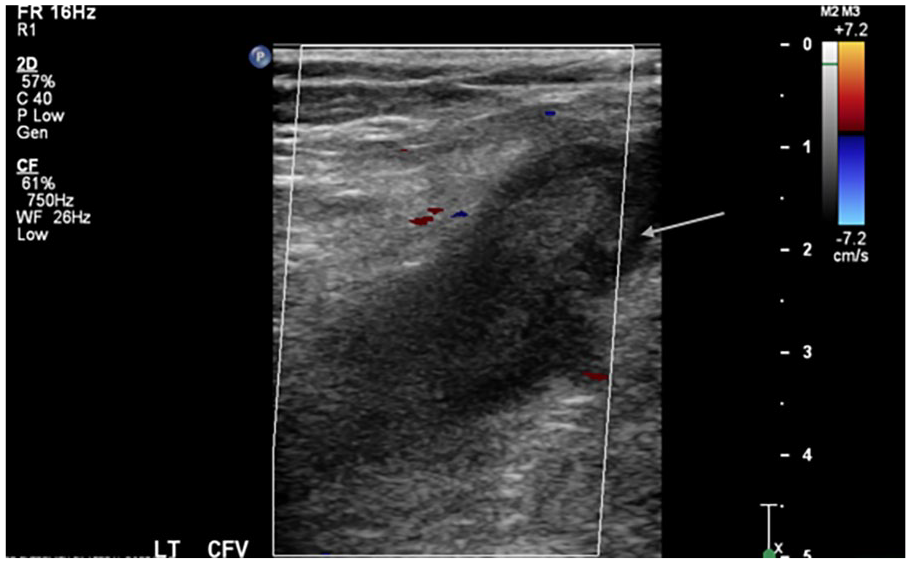
Left lower-extremity venous duplex ultrasound revealing an acute, large, hypoechoeic thrombus (arrow) within the noncompressible left common femoral vein.
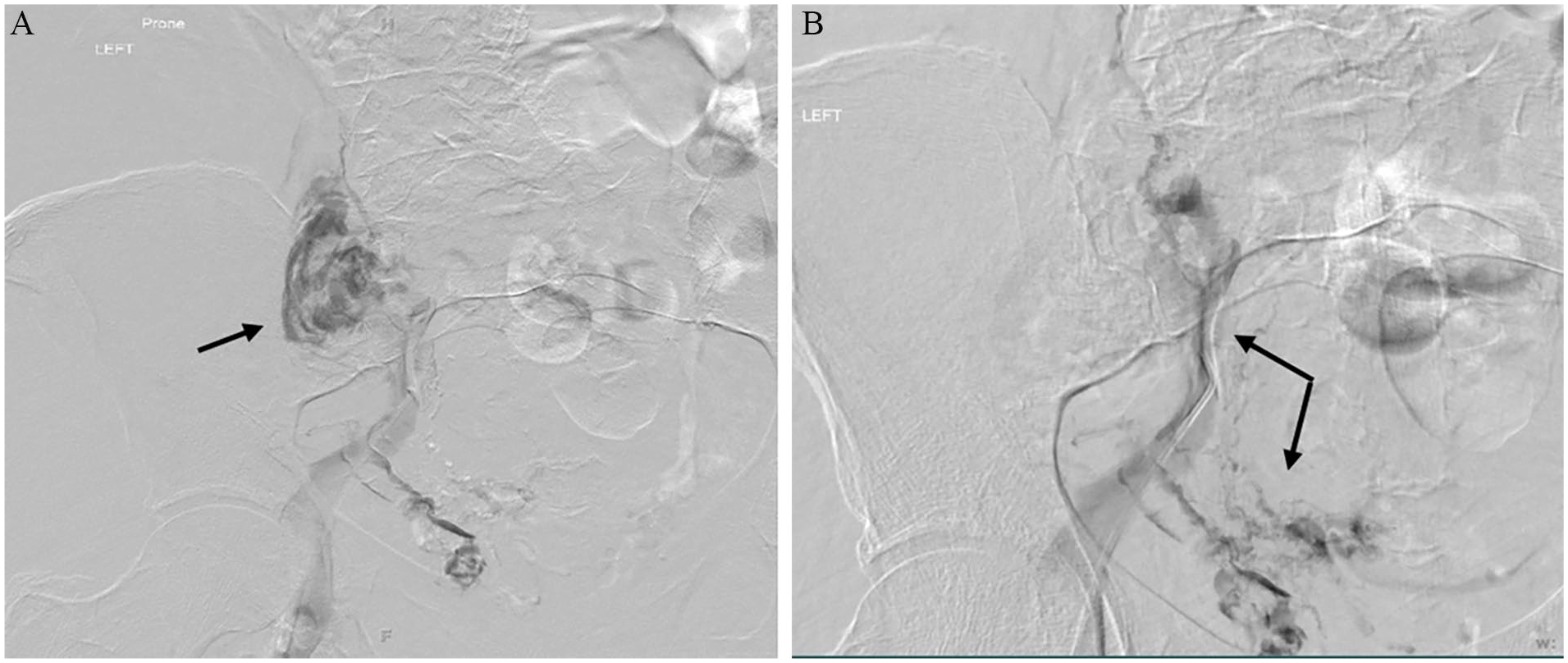
Catheter-based venogram showing active extravasation arising from near the confluence of the left common and external iliac veins (
Based on this presentation, what is the optimal treatment strategy?
Literature review
We conducted a literature search for manuscripts and poster presentations on PubMed and Google from all available dates (1977–November 2022) using the search term “spontaneous iliac vein rupture” with a filter of “full text available” (Figure 4; online Supplemental Table 1). It should be noted that four out of the nine cases from the Jiang et al. publication 1 were not included as the diagnosis of SIVR was not confirmed. Although we included the other five patients in the total number of SIVR cases, we were not able to stratify treatment modality and outcome per patient for this sample. In summary, we found a total of 51 unique English language publications with 60 total cases, out of which 55 could be further stratified.
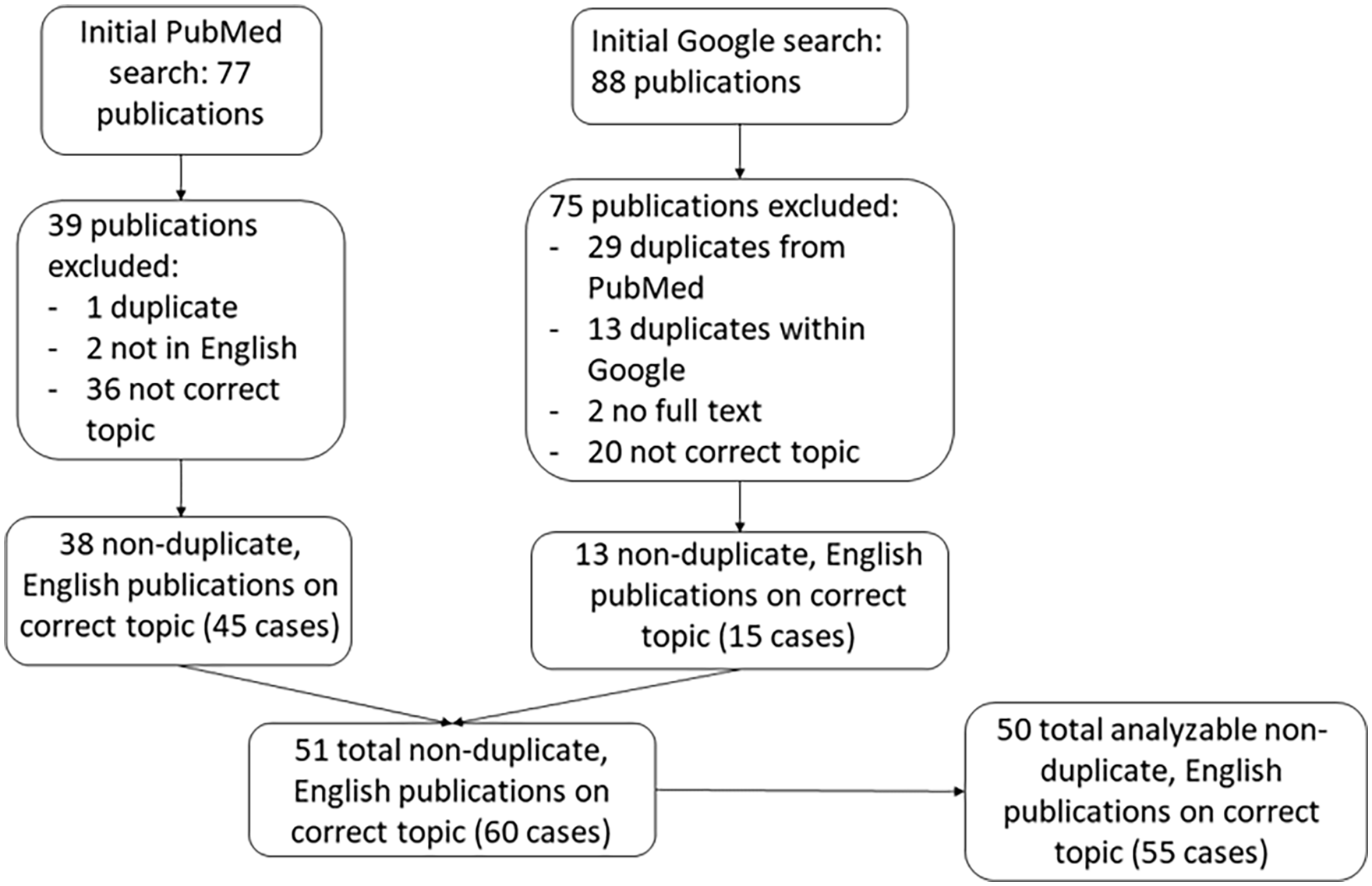
Flowchart including articles found in PubMed and Google search using the search term: “spontaneous iliac vein rupture” and a filter of “full text available.” This resulted in a total of 51 manuscripts and 60 cases. Note: one manuscript with five cases was excluded because relevant data were not available for analysis.
Limitations
Because our goal was to stratify treatment options including conservative and interventional strategies, and outcome, we had limited our search to papers with the full-text available. Thus, we may have not reported all SIVR cases in the literature. Nevertheless, this rigorous case search provides useful information on the characterization and trends in practice of this rare condition.
Clinical presentation of spontaneous iliac vein rupture (SIVR)
Iliac vein rupture (IVR) is a dreaded complication associated with trauma or surgical interventions. However, SIVR is a rare entity of still uncertain etiology. Proposed causes of SIVR include mechanical (MTS and DVT), hormonal, and inflammatory processes.2–5 DVT-induced obstruction and inflammation may lead to vessel wall weakness and rupture.2,5,6 It has also been speculated that the obstruction of flow and increased pressure due to MTS can cause further weakening of the vein wall and increase the likelihood of rupture. 5 Other rare etiologies include pregnancy or loss of the vessel-protective effects of estrogen after menopause (hormonal fluctuation), intra-abdominal masses, vibratory irritation, and sudden increase in intra-abdominal venous pressure (valsalva maneuver, bending, or coughing).3,5–8
Clinical presentation of this condition includes the sudden onset of painful abdominal mass, paleness, and general signs of hypovolemic shock including hypotension. Other symptoms include leg swelling, pain, and weakness, often secondary to an acute DVT 8 (Table 1). A review of 35 patients with SIVR between 1961 and 2010 reported that 79% of these cases were related to vein thrombosis. 1 Therefore, management of SIVR presents a clinical dilemma for the managing physician who must balance the benefit of reducing clot burden with the risk of life-threatening hemorrhage.
Summary of spontaneous iliac vein rupture.
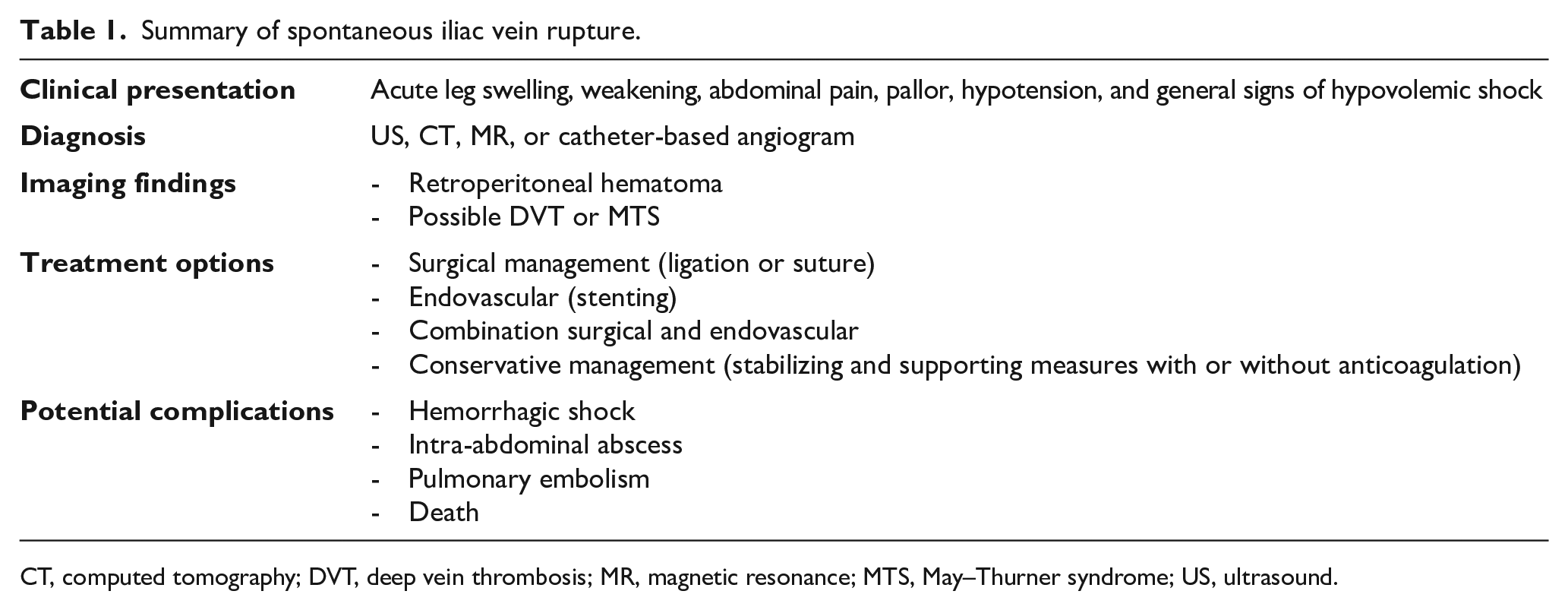
CT, computed tomography; DVT, deep vein thrombosis; MR, magnetic resonance; MTS, May–Thurner syndrome; US, ultrasound.
Laboratory findings may include low Hgb with high D-dimer. Imaging with venous duplex ultrasound, CT, and/or catheter-based venogram usually confirms the presence of SIVR and helps to clarify the presence of concurrent vein thrombosis or compression.1–3
Based on our literature search, SIVR occurred primarily in women (41/55, 74.5%) and predominately affected the left limb (53/55, 96.4%). Of these cases, 51/55 (92.7%) underwent treatment including conservative, surgical, endovascular, or combined intervention. The other four patients died before receiving any treatment, out of whom three were postpartum. We report an overall mortality rate of 18.2% (10/55) and an overall complication rate of 49.1% (27/55). Reported complications included lower-extremity edema, DVT, pulmonary embolus, decrease in respiratory function, intra-abdominal abscess, atrial fibrillation, and mortality (Table 2; see online Supplemental Table 1 for complete descriptions of complications).
Treatment outcomes in the 55 analyzed SIVR cases.
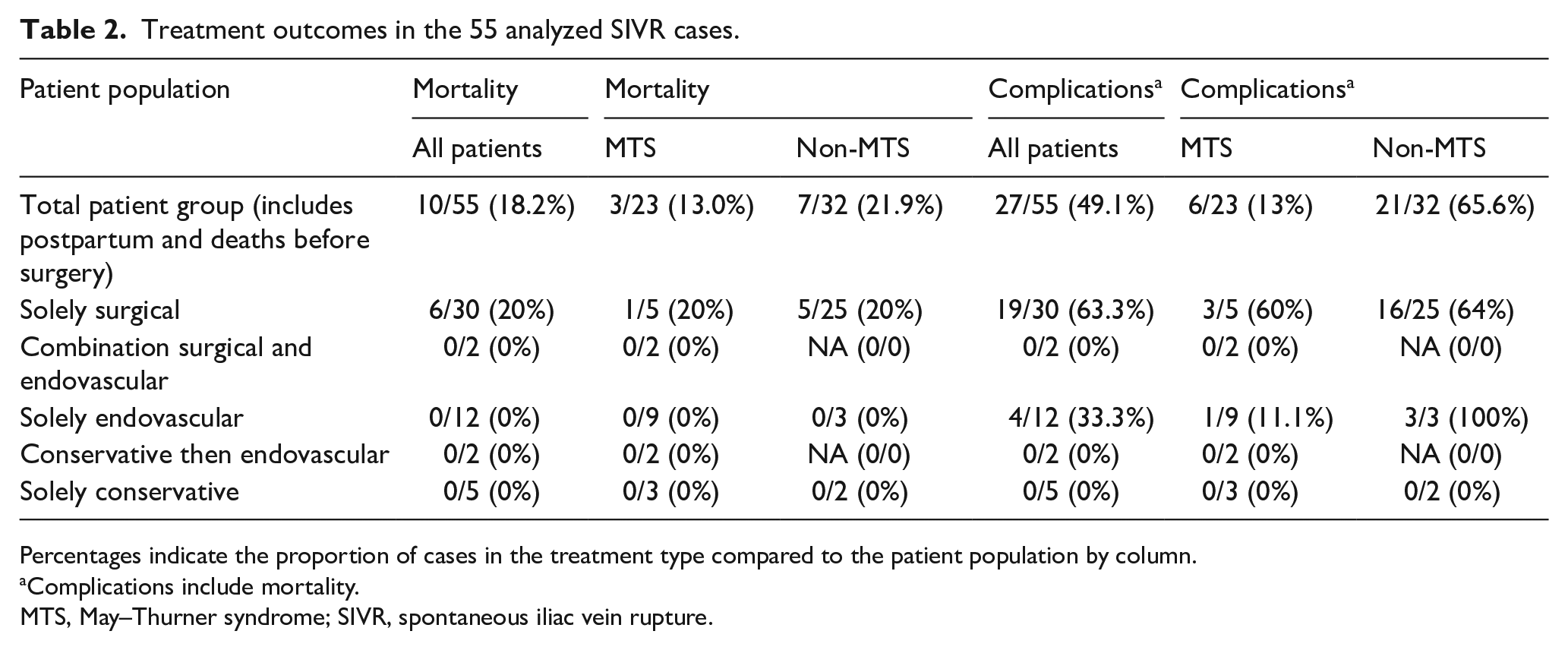
Percentages indicate the proportion of cases in the treatment type compared to the patient population by column.
Complications include mortality.
MTS, May–Thurner syndrome; SIVR, spontaneous iliac vein rupture.
SIVR in the context of May–Thurner syndrome
Of the cases we reviewed, 23/55 (41.8%) had reported underlying MTS (Table 3). Our case report adds to the growing evidence supporting that MTS is an important risk factor for SIVR. First described in 1957 by May and Thurner, May–Thurner anatomy (MTA) was encountered in 22% of the 430 cadavers autopsied. 5 More recent studies have corroborated this estimate to be around 24%, with the majority of patients with > 50% compression remaining asymptomatic. 9 In fact, only a fraction of patients with MTS are symptomatic with DVT, which occur in 2–5% of patients with this condition.10,11 For this reason, and given the presence of more common risk factors for DVT such as oral contraceptives, recent pregnancy, or thrombophilia, MTS has been frequently overlooked, leading to recurrent DVT, postthrombotic syndrome, and rarely to left IVR.10,12–15 Thus, increased vigilance should be taken in the clinical setting when determining causes of DVT to prevent more serious complications, such as SIVR.
Treatment modalities of the 55 analyzed cases with SIVR based on the presence or absence of May–Thurner syndrome.
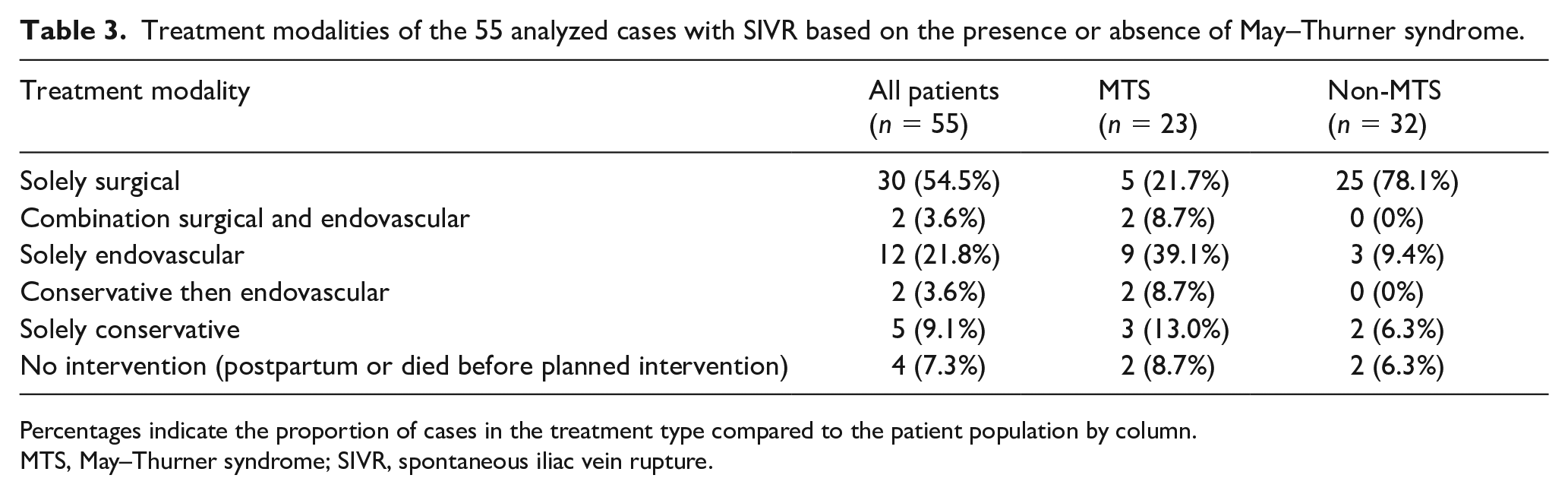
Percentages indicate the proportion of cases in the treatment type compared to the patient population by column.
MTS, May–Thurner syndrome; SIVR, spontaneous iliac vein rupture.
Management options for SIVR
There are several options for the treatment of SIVR. More than half of the patients we reviewed (30/55, 54.5%) had open-surgical operations, which included ligation, primary surgical repair, Palma–Dale bypass, and/or evacuation of retroperitoneal hematoma. Additionally, endovascular treatment with stenting (12/55, 21.8%) has been shown to be an effective modality. 16 Conservative treatment is not often considered for this condition (5/55, 9.1% of all cases), though the outcome of our case supports the viability of this approach. Endovascular treatment has also been rarely reported in combination with both open-surgical (2/55, 3.6%) or conservative approaches (2/55, 3.6%). Table 3 summarizes the complete breakdown of treatment options reported in our literature search.
Though open-surgical treatment has been the most reported treatment option for SIVR, this treatment modality has been associated with higher complication and mortality rates than other treatment options. We report a mortality rate of 20% (6/30) for surgery-only treatment and a complication rate of 63.3% (19/30) (Table 2; see online Supplemental Table 1 for a complete list of complications). This mortality rate is corroborated by past literature reviews, which found between 23.8% and 29%.4,7,8 In contrast, we report a 0% mortality and complication rate for all other treatment options, except for solely endovascular treatment, which had a complication rate of 33.3% (Table 2). However, we agree with Tannous et al. that the complication and mortality rates may be underestimated due to bias in reporting favorable outcomes. 7 Nevertheless, we have noticed a change in practice pattern, or at least in reporting, among the papers we have reviewed that nonsurgical treatment options have been more frequently considered (increased from 17.9% before 2012 to 74.1% after), likely due to the higher complications encountered in the surgical group including mortality. 16
Management options for SIVR with concurrent May–Thurner syndrome
Patients with underlying MTS were reported to receive more endovascular (39.1% vs 9.4%) and fewer solely surgical treatments (21.7% vs 78.1%) than patients without MTS (Table 3). Additionally, patients with MTS who were treated with a solely endovascular approach had a lower complication rate than patients without MTS (1/9, 11.1% vs 3/3, 100%). However, the complication rate for surgical intervention only was similar between the two groups (MTS: 3/5, 60% vs non-MTS: 16/25, 64%) (Table 2). We have noticed a trend of increased reporting of endovascular treatment for SIVR, and an increased reporting of underlying MTS, which can be explained by increased awareness of MTS as an important etiology for SIVR.
To the best of our knowledge, there have been only three reported cases of SIVR with underlying MTS in the English literature that were successfully and solely managed concervatively.3,17,18 All three were treated with anticoagulation. One patient was initially treated with therapeutic low-molecular weight heparin (LMWH) and subsequently bridged to warfarin. 3 The second patient was treated with intravenous (IV) unfractionated heparin (UFH) and discharged on LMWH. 17 The third patient was initially treated with LMWH and was discharged on acenocoumarol with a target INR of 2.0–2.5. 18 Although one of these patients developed a pulmonary embolism (PE), 3 all three recovered well and experienced improved leg edema, hematoma, and overall symptoms related to DVT and PE.3,17,18
Of the surviving patients with SIVR, 32/45 (71.1%) were reported to have received anticoagulation postintervention or as part of the conversative management. Cases in which anticoagulation was started as a treatment for a complication, such as DVT, were not counted in this percentage. The complication rate for patients who received anticoagulation was 11/32 (34.4%) versus 6/13 (46.2%) for those who did not. Three out of the five cases (60%) who had conservative management received anticoagulation therapy.3,17,18 Their thrombosis and leg swelling resolved over time.
The data are too scarce to support any recommendations for timing of anticoagulation initiation, appropriate agent, or dosing. Decisions regarding initiating anticoagulation should be based on thrombus and bleeding sites, extension, and related complications. We suggest initiating low-intensity prophylactic IV UFH (goal activated partial thromboplastin time [aPTT] of 60–80 seconds) once bleeding is contained and Hgb has been stable. We favor apixaban given its safety profile. Similarly, there are insufficient data to determine the role of inferior vena cava (IVC) filter placement in patients with SIVR. However, based on current evidence, a retrievable IVC filter can be considered in patients with extensive concurrent DVT who are not candidates for anticoagulation. It is important to note that this approach may increase the risk of lower-extremity DVT burden and related symptoms. 19
Based on our review, conservative treatment with anticoagulation alone has not been considered frequently given the tight balance between thrombotic burden and life-threatening bleed. 20 Nevertheless, compared to intervention, the conservative approach in patients with or without underlying MTS was associated with a better outcome, fewer complications, and no reported mortality (Table 2).3,4,17,18,21
Back to our patient
The patient was managed urgently with a transfusion of six units of packed red blood cells, one unit of platelets, and three units of fresh frozen plasma, which resulted in improved Hgb (12.3 g/dL) and recovery of her left leg motor function. Conservative management was considered based on the size of the bleed, DVT-related symptoms, and possible complications related to any surgical intervention. IVC filter was not considered given the low risk of thrombus migration with concurrent MTS and given the increased risk of worsening thrombus burden below the filter which could lead to phlegmasia and an urgent need for intervention. After weighing the risks and benefits, anticoagulation with IV UFH (goal aPTT of 60–80 seconds) was started on hospital day 6, when Hgb had been stabilized with no signs of expanding hematoma. As she continued to improve with stable Hgb levels, vital signs, and a contained hematoma shown on a repeat CTA, she was transitioned to oral apixaban 5 mg twice daily on hospital day 9. The patient was discharged home on hospital day 10 with close Hgb and vital sign checks. She continued to improve over the following 3 months with CT venogram imaging at 1 and 3 months showing resolution of the left pelvic/retroperitoneal hematoma with persistent left common iliac vein compression and chronic thrombosis (Figure 5). She has remained asymptomatic on apixaban with stable Hgb and vital signs.
Transverse image of a CT venogram of the abdomen and pelvis showing resolution of the left-side retroperitoneal hematoma and persistent left common iliac vein compression between the left common iliac artery and the vertebral body with chronic thrombosis (arrow).
Therefore, our case sheds light on an unique condition and adds to the scarce evidence supporting conservative management versus surgical intervention in the setting of SIVR with concurrent MTS.
Conclusion
Though SIVR is extremely rare, it can lead to serious complications – including death. MTS should be considered among the differential diagnoses in patients presenting with SIVR. Given the relatively high risk of complications associated with open-surgical intervention and the low morbidity of stand-alone medical management, conservative management should strongly be considered in hemodynamically stable patients. Endovascular therapy may be considered over open surgery in patients with hemodynamic instability.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X231175697 – Supplemental material for Spontaneous iliac vein rupture and thrombosis in patients with May–Thurner syndrome: A narrative review
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X231175697 for Spontaneous iliac vein rupture and thrombosis in patients with May–Thurner syndrome: A narrative review by Nedaa Skeik, Andrew Adamek and Jesse Manunga in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.