
Abstract

Several approaches have assessed arterial compliance in population studies, but few compliance measures have been rigorously evaluated for reproducibility. PTC1 and PTC2 are indices of arterial compliance, derived from a Windkessel model of the pressure waveform (a continuous pressure measurement throughout the cardiac cycle), and have been shown to be associated with cardiovascular disease.1–7 The indices are named PTC1 and PTC2 because they are analogous to other measures of compliance called C1 and C2 and share similarities with time constants derived from pressure profiles. PTC1 and PTC2 can be computed from waveforms using standard open-source software, but so far have only been obtained from participants of the Multi-Ethnic Study of Atherosclerosis (MESA) 8 at the baseline exam.1,2 In this study, we report on the feasibility and reproducibility of PTC1 and PTC2 among MESA participants using waveforms collected at the fifth exam (during 2010 to 2012) with a different device. A subset of the participants was selected to have repeat measurements performed on the same day for quality control purposes. The study was approved by the institutional review boards of all participating clinics and all participants provided informed consent.
At the fifth MESA exam, pressure waveforms were collected by technicians (certified after they had successfully obtained waveforms from three individuals) using a tonometer (Millar Instruments, Houston, TX, USA) that sampled pressures at 250 Hz and a stabilizer to hold the tonometer in place over the participant’s right (whenever possible, otherwise left) radial artery. The technician was instructed to perform the procedure for a total of 60 seconds (two 30-second recordings), immediately removing and repositioning the device between 30-second recordings. The median total length of recordings was 60 seconds and the IQR was 60–90 seconds. Here, we use ‘60-second’ recording to refer to the total recording. Participants who were randomly selected to have repeat measurements for quality control purposes had waveforms collected for an additional 60-second recording later that same day. A different technician was expected to perform the repeat procedure whenever possible.
From the recordings, we obtained beat-specific waveforms and PTC1 and PTC2 using methods as in Brumback et al., 1 with a minor adjustment due to the 250 Hz sampling rate at the fifth exam (online Supplemental Figure). The open-source code to obtain PTC1 and PTC2 is available at github.com/LBrumback/PTC1andPTC2.
We created one PTC1 and one PTC2 for each participant using the median PTC1 and median PTC2 from all beat-specific waveforms from the 60-second recording. For the subset of participants with same-day repeat measurements, we created a second PTC1 and PTC2 for their additional 60-second recording to assess inter- and intra-technician reproducibility. We also computed the median from only the latter 30 seconds of each of the two 60-second recordings to investigate reproducibility over 30 seconds versus 60 seconds.
Of 4716 original MESA participants who participated in the fifth exam, 4005 (including 134 with repeat same-day measurements) provided waveform data. The primary reason for missing waveform data was clinic staff were not yet certified to perform the procedure at the time of the participant’s exam. There was a total of 303,028 beat-specific waveforms. The median (IQR) number of beat-specific waveforms across participants was 67 (58, 83), which is appropriate given a 60-second recording and typical heart rate. Among the 4005 participants, the mean ± SD age was 70 ± 9 years; 47% were male; and 41% were White, 12% were Chinese, 27% were Black, and 21% were Hispanic/Latino. The participants with repeat measurements were similar except fewer were White (23%) and more were Hispanic/Latino (38%).
PTC1 and PTC2 were successfully computed for all 4005 (100%) participants. Mean ± SD was 279 ± 131 milliseconds for PTC1 and 85 ± 32 milliseconds for PTC2 from 60-second recordings. Among all 134 participants with same-day repeat waveform measurements (78 with different technicians, 56 with same technicians), the correlation was 0.78 for PTC1 and 0.87 for PTC2 with 60-second recordings, and the mean ± SD of differences were 4.6 ± 82 and 0.8 ± 15 milliseconds, respectively. Reproducibility was better (i.e., correlations were higher and the SD of differences were smaller) with the same technician compared to different technicians (Figure 1). Reproducibility was also better from 60-second recordings compared to 30-second recordings (online Supplemental Table); for example, with 30-second recordings, the correlation among all participants was 0.65 for PTC1 and 0.79 for PTC2, and the mean ± SD of differences were 8.0 ± 111 and 2.8 ± 21 milliseconds, respectively.
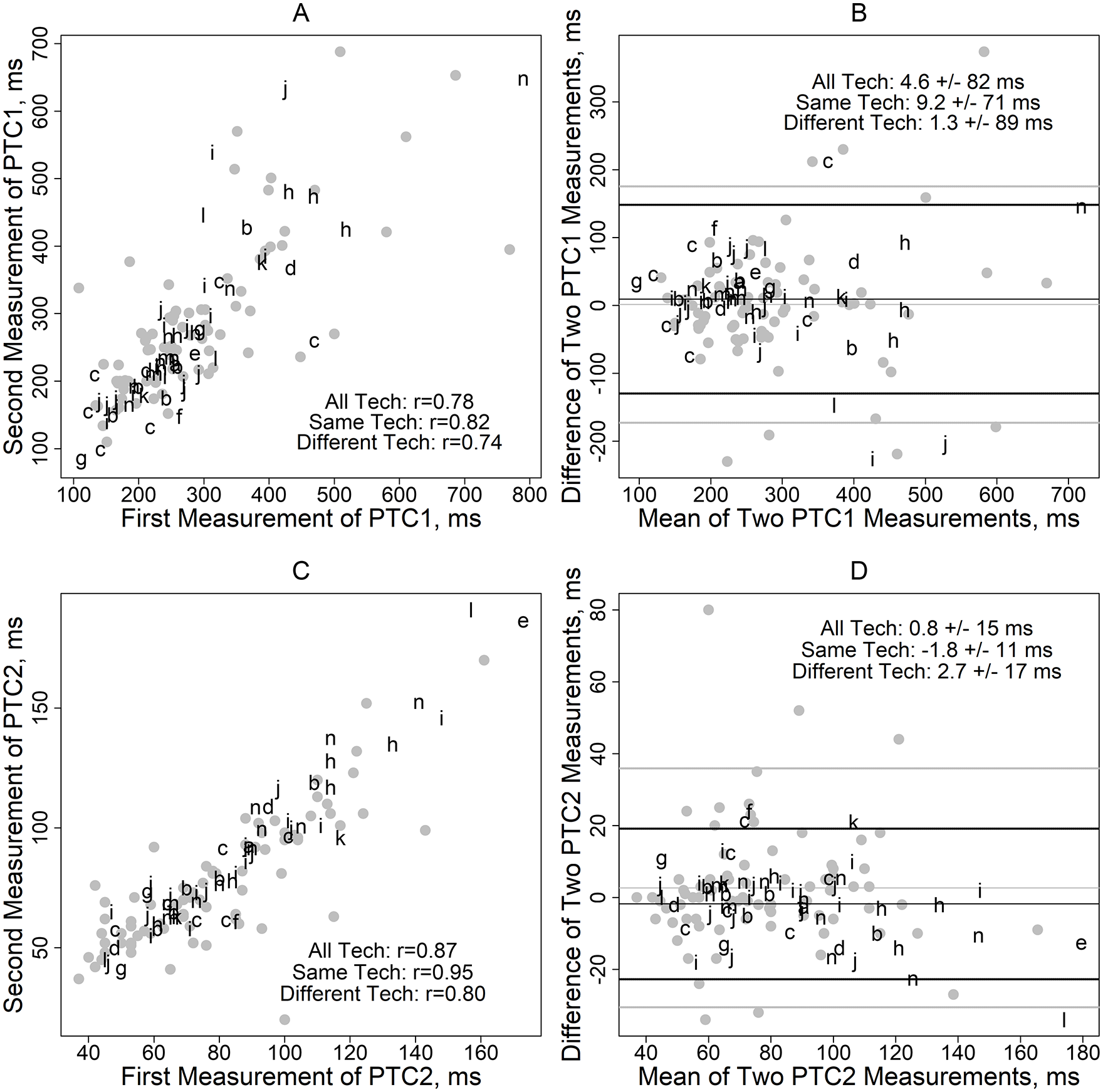
Scatterplots
In summary, PTC1 and PTC2 were successfully computed from all participants with waveform data, which is notable as other measures of arterial compliance have not always been computed for individuals with irregular waveforms. This is the first study to describe inter-technician (in addition to intra-technician) reproducibility of PTC1 and PTC2 and reproducibility based on longer (60-second) versus shorter (30-second) recordings. The intra-technician reproducibility from 30-second recordings is similar in this study (MESA Exam 5) and the prior study involving another tonometer/device (MESA Exam 1). 1 Intra-technician reproducibility was higher than inter-technician reproducibility, which suggests that precision, but not necessarily accuracy, is better when one technician performs repeat measurements. Although PTC1 and PTC2 (unlike C1 and C2 from Hypertension Diagnostics Inc.) are not affected by linear calibration of the waveform to systolic and diastolic blood pressure which can vary due to circadian rhythm, it is possible that time of day affected the intra- and inter-technician reproducibility. At both MESA Exam 1 and Exam 5, PTC2 appeared more reproducible than PTC1. There is some literature to suggest that PTC1 is related to compliance of the large arteries and PTC2 is related to compliance of the small arteries (and to a similar measure, which has been termed ‘oscillatory’ or ‘reflexive’),9,10 but it is not obvious why compliance of the small arteries might be more reproducible. Both PTC1 and PTC2 are functions of Windkessel model parameters and it is relatively straightforward to compute them, but if only one measure can be reported, we recommend PTC2. We also recommend collecting waveforms for a total of 60 instead of 30 seconds since that appears to improve reproducibility without adding much time to a relatively simple, noninvasive procedure. Further evaluation of PTC1 and PTC2 in other studies would be useful.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X221151089 – Supplemental material for Reproducibility of PTC1 and PTC2, indices of arterial compliance, from the radial artery waveform: The Multi-Ethnic Study of Atherosclerosis
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X221151089 for Reproducibility of PTC1 and PTC2, indices of arterial compliance, from the radial artery waveform: The Multi-Ethnic Study of Atherosclerosis by Lyndia C Brumback, Leah IB Andrews, David R Jacobs, Daniel Duprez, Elizabeth K Hom Thepaksorn, Joel D Kaufman, Julie Denenberg and Matthew Allison in Vascular Medicine
Footnotes
Acknowledgements
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by the National Institutes of Health (HHSN268201500003I, N01-HC-95159, N01-HC-95160, N01-HC-95161, N01-HC-95162, N01-HC-95163, N01-HC-95164, N01-HC-95165, N01-HC-95166, R01 HL098382, and R01 HL142283) and the National Center for Advancing Tran-slational Sciences (UL1-TR-000040, UL1-TR-001079, and UL1-TR-001420).
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.