
Abstract

Keywords
Chronic limb-threatening ischemia (CLTI) has a high level of morbidity and mortality if there are delays in diagnosis and revascularization. This problem is compounded in rural areas with limited access to vascular specialists, as evidenced by higher rates of amputation in this geographic cohort. 1 The use of telemedicine may improve disparities by connecting vascular experts with patients at risk for CLTI and thereby expediting their evaluation, management, and revascularization. We sought to determine whether a telemedicine clinic is feasible for the evaluation of veterans in rural areas with suspected CLTI.
We connected a rural VA wound care clinic in Hudson Valley, New York with a tertiary care VA hospital in West Haven, Connecticut. Traditionally, patients seen in the wound clinic with suspected CLTI were referred for a face-to-face evaluation at this tertiary hospital, which could be several months in the future, and would arrange their own transportation to the appointment. In this model, a vascular curriculum was developed for first-line wound care providers (primarily podiatrists and internists) for identification of wounds and symptoms that would benefit from a vascular evaluation. Telepresenters underwent formal training taught by a vascular expert to learn how to perform a thorough wound evaluation and vascular physical exam utilizing Doppler pulse evaluation, as well as a sensory examination for neuropathy. Patients underwent synchronous telemedicine evaluation with the vascular specialist during a 30-minute scheduled appointment. When lower-extremity angiography was deemed necessary, transportation was arranged between the two VA systems for expedited care. This study was exempt from review by the VA Institutional Review Board as an approved quality improvement study.
Forty-eight veterans were referred to the vascular telemedicine clinic between June 2019 and July 2021 and were prospectively followed. The average time from consult request to virtual appointment was 23.2 ± 17.9 days. There were 40 referrals for nonhealing lower extremity wounds and eight who had claudication symptoms rather than evidence of CLTI. Baseline characteristics of the study cohort are shown in the online Supplemental Table.
The outcomes for the total cohort are summarized in Table 1 over the median follow-up period of 660.5 days. The average travel distance saved via utilization of telemedicine rather than face-to-face consultation was 280.0 ± 182.6 miles. Of the 40 patients with lower extremity wounds, 70% were deemed to be secondary to peripheral artery disease (PAD) based on noninvasive studies, abnormal Doppler physical exam, and clinical judgment. The rest were thought to be secondary to venous insufficiency and/or peripheral neuropathy. Nearly one-third of the patients with perceived arterial etiology were referred for peripheral angiography, of which nine (22.3%) underwent peripheral vascular intervention (PVI) and four (10.0%) were referred for surgical revascularization following angiography. The remainder (n = 15) were successfully managed medically to complete wound healing. A large majority of patients (65%) had complete resolution in wounds at follow-up, though five (12.5%) did not attend follow-up appointments or sought opinions at outside facilities. Only three (7.5%) of the 40 patients with wounds underwent amputation. Two were minor amputations after PVI and the one major amputation occurred after the patient sought an outside opinion rather than following through with surgical referral within the VA system.
Vascular telemedicine clinic patient outcomes based on presenting symptom (wounds or claudication).
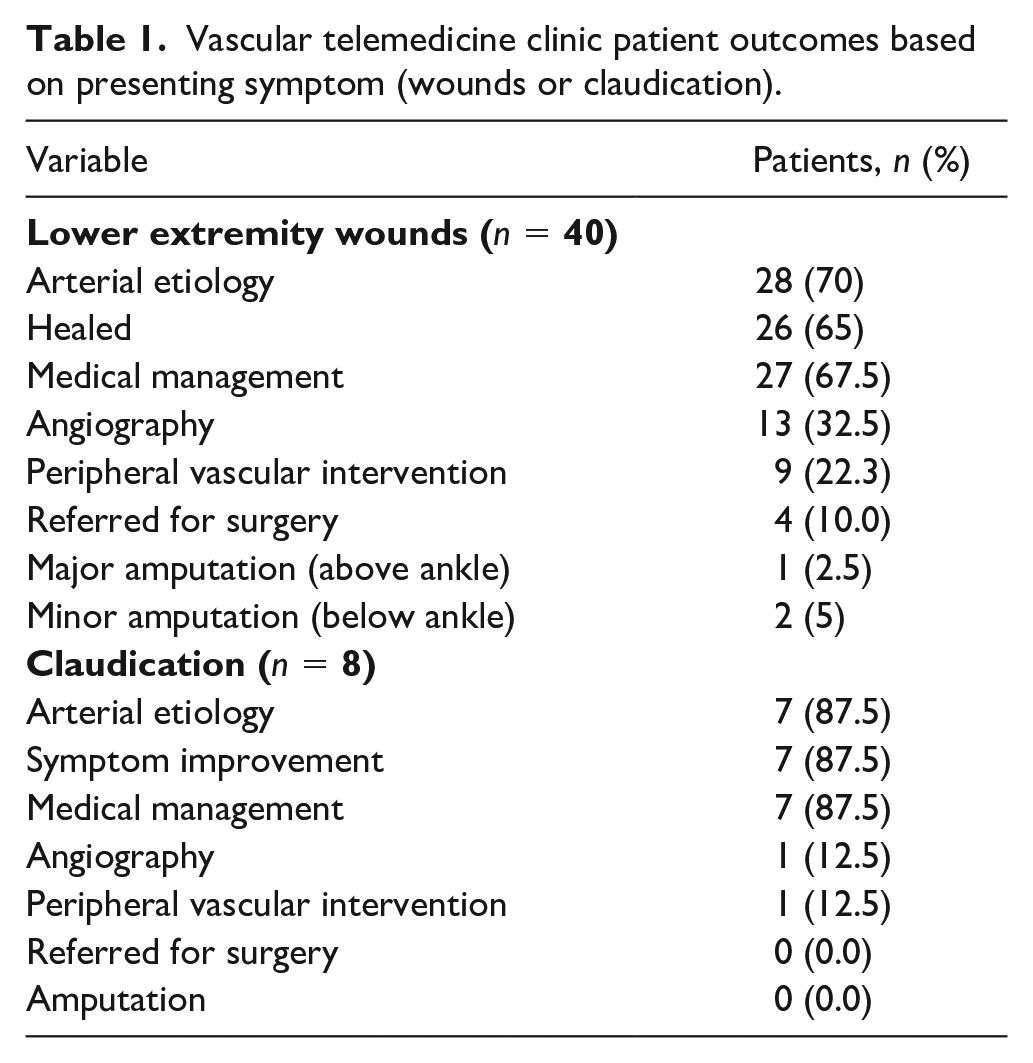
Of the eight patients with claudication symptoms, seven were thought to be secondary to PAD. One patient was treated with PVI for limiting claudication; the remaining patients were treated conservatively with medication optimization and supervised exercise therapy. No amputations were observed during follow-up over a median of 734.0 days.
The current study demonstrates that telemedicine enables rapid time from consult request to vascular evaluation, averaging approximately 3 weeks, which is considerably faster than the average 8.6 weeks for conventional face-to-face evaluation. 3 Furthermore, the remote performance of a high-quality vascular physical exam by a trained telepresenter was feasible and the determination of underlying PAD was possible. Finally, patients who needed evaluation with angiography were successfully transported to the tertiary campus, saving approximately 280 miles of travel per patient.
CLTI is common among United States veterans owing to increased rates of diabetes, hypertension, dyslipidemia, and tobacco use.4,5 Disappointingly, the limb amputation rates for patients in the VA healthcare system are twice those in public hospitals and four times higher than in private facilities, with veterans waiting four times longer for treatment. 2 The poor outcomes largely stem from regional disparities, with VA facilities lacking access to vascular specialists and the ability to perform revascularization. 4 This was highlighted in a recent retrospective study of over 20,000 VA patients, which demonstrated that nearly 50% of veterans receive amputation prior to angiography with large differences at the facility level. 4
For telemedicine to be effective and improve outcomes, an accurate vascular examination must be feasible remotely. Prior multicenter studies have shown that Doppler examinations performed by nonvascular clinicians are poorly reliable; 6 however, our telepresenters underwent comprehensive training. Additionally, the synchronous performance of the remote Doppler exam ensured that pulses were obtained with real-time discrimination of phasicity as monophasic, biphasic, and triphasic, as confirmed by the vascular expert. This study demonstrates that the remote vascular examination is feasible when performed by a trained technician.
Although this was designed as a feasibility study, patient outcomes were excellent in this small cohort. This may result from a combination of educating primary providers to assess for early signs of CLTI and training telepresenters to facilitate a remote examination, allowing for an expedited and thorough evaluation from a vascular expert. Having telepresenters on site also decreased disparities related to language barriers, fluidity with technology, internet access, and physical limitations – inequalities which can be paradoxically increased through telemedicine.
This pilot study has several limitations. This was a small population consisting of mostly White males. Owing to cost limitations, ankle–brachial indices were not obtained for all patients and angiography was reserved for patients who did not improve despite optimal medical therapy. Because the VA sites were in different states, we relied on the primary medical physicians to enact recommended medication changes. Finally, the descriptions of wound characteristics were limited.
In conclusion, the use of a telemedicine clinic is feasible for the evaluation of patients with suspected PAD and CLTI. Future studies are needed to compare the outcomes of these patients to patients who are seen in traditional face-to-face consultations. Telemedicine holds promise for mitigating disparities in vascular care.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X221148797 – Supplemental material for Use of telemedicine facilitated by trained telepresenters to manage advanced peripheral artery disease in rural areas
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X221148797 for Use of telemedicine facilitated by trained telepresenters to manage advanced peripheral artery disease in rural areas by Thomas J Breen, James B Peake, Heidi Keefe, Justine Moran, Felix Kunjukutty, Steven Pfau and S Elissa Altin in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.