Abstract

Poster Number: 51
Abstract Number: 1272715
Aortobronchial fistula in a 75-year-old male presenting with hemoptysis- a case report
St. Luke’s Medical Center Global City
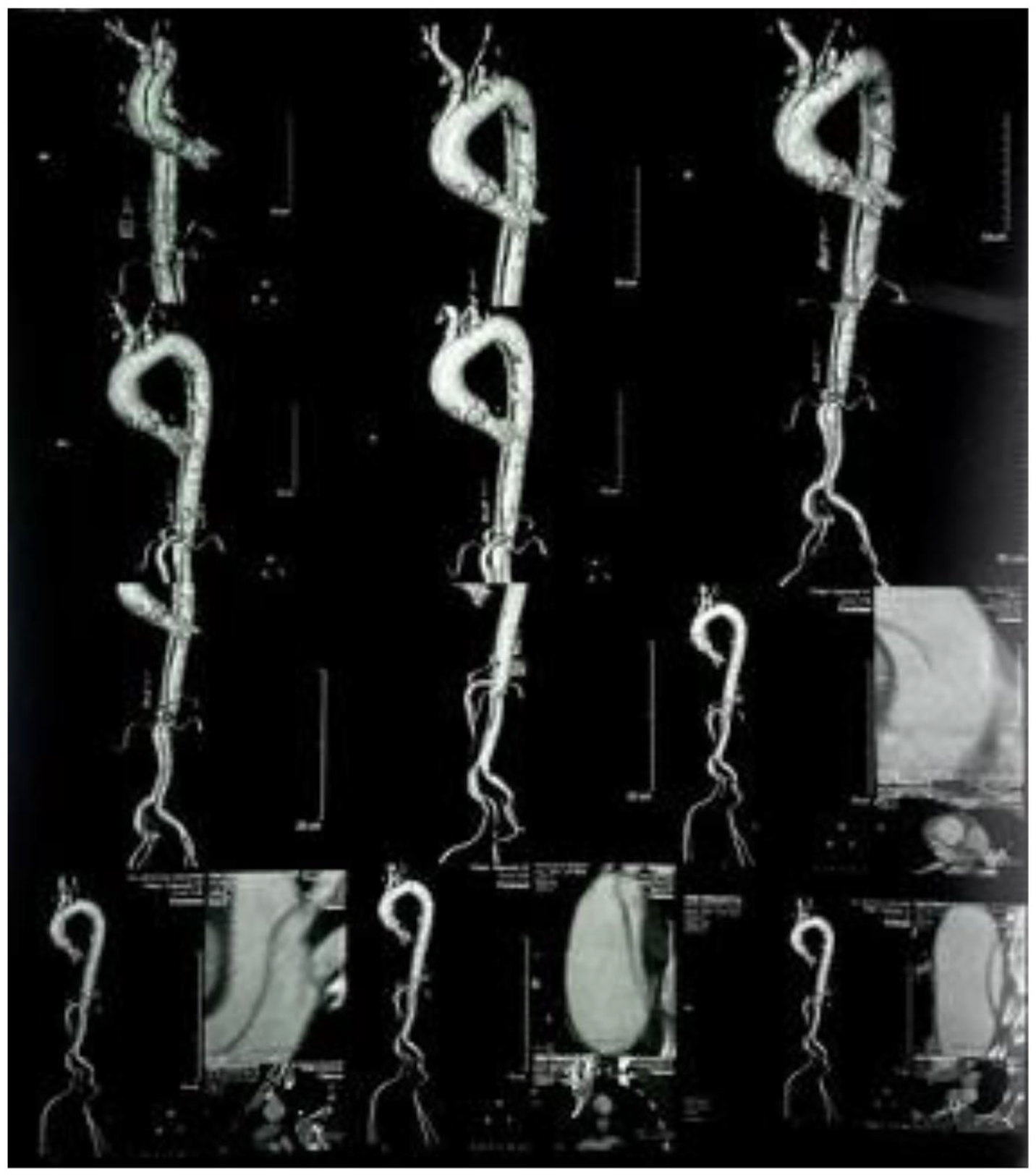
Background: Aortobronchial fistula is an anomalous communication between the aorta and a segment of the tracheobronchial tree. This is a rare condition with a relatively low incidence, ranging from 0.56% to 1.7%. Patients with aortobronchial fistula usually present with hemoptysis especially in those with a history of thoracic aortic aneurysm. This case highlights clinical awareness on this uncommon cause of hemoptysis and with timely diagnosis and immediate surgical intervention, it can prevent fatal outcome and improve survival rate.
Case presentation: Aortobronchial fistula is an anomalous communication between the aorta and a segment of the tracheobronchial tree. It has a relatively low incidence, ranging from 0.56%. Patients with aortobronchial fistula usually present with hemoptysis but a high index of suspicion is needed to arrive at the correct diagnosis. A Computed Tomography (CT) aortogram of the thoracoabdominal aorta showed thoracic aortic aneurysm and infrarenal aneurysm. Additional findings include extravasation of blood out of the aneurysmal sac, manifesting as hematoma formation with gas locules adjacent to the hematoma and web-like endobronchial densities in the left upper lobe, all suggestive of aortobronchial fistula. He underwent hybrid procedure using Type 1 aortic debranching of the aortic arch with thoracic endovascular aortic repair of the mid ascending to proximal aorta and aortic endovascular repair of the infrarenal aneurysm. This case highlights clinical awareness on this uncommon cause of hemoptysis and with timely diagnosis and immediate surgical intervention, it can prevent fatal outcome and improve survival rate.
Conclusions: In conclusion, aortobronchial fistula is a rare etiology of hemoptysis. This rare condition should be highly suspected in patients with known thoracic aortic aneurysm who present with hemoptysis. Although treatment is still challenging especially when dealing with an elderly who has multiple co-morbidities with complex aortic pathology, hybrid procedures can offer a promising alternative surgical treatment as a less invasive procedure for high-risk patients. With a timely diagnosis and expert surgical intervention, the survival rate is high.
Poster Number: 52
Abstract Number: 1269536
A rare case of COVID-19 associated aortitis
Prisma Health - University of South Carolina School of Medicine
Background: There has been a myriad of vascular manifestations associated with the coronavirus disease 2019 (COVID-19) pandemic, including reports of associated small- and medium-vessel vasculitis. However, there are limited reports of large vessel vasculitis, specifically aortitis, related to the COVID-19 infection.
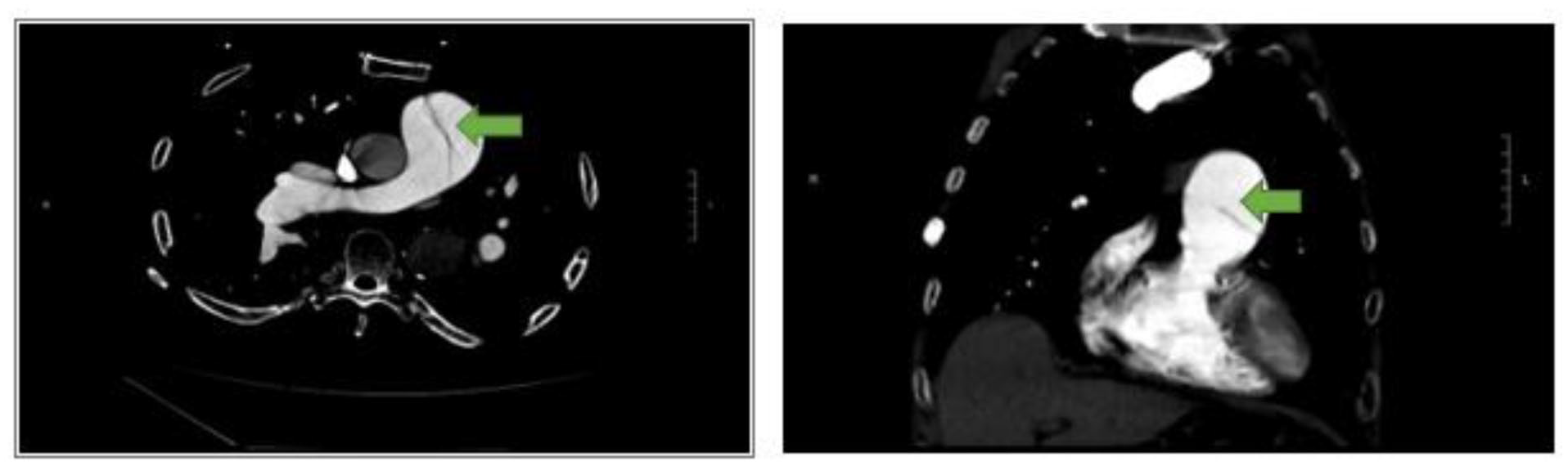
Case presentation: A 62-year-old female with history notable for peripheral artery disease, chronic obstructive pulmonary disease, hypertension, and hyperlipidemia presented for evaluation of abdominal pain. She was hospitalized two weeks prior with a COVID-19 infection causing respiratory failure. At presentation, she endorsed one week of progressive lower abdominal pain with anorexia. Vitals were notable for a blood pressure of 185/93 mmHg and heart rate of 94. Labs were notable for white blood cell count 8.1, CRP 85.4, and ESR of 96. A CT abdomen/pelvis with IV contrast demonstrated circumferential wall thickening of the infrarenal aorta with surrounding inflammatory stranding, suggestive of aortitis (Panel A). Additional evaluation included negative blood cultures, non-reactive RPR, normal IgG subclass 4, negative ANA screen, negative myeloperoxidase and proteinase-3 antibodies, and negative cryoglobulin. Given her recent COVID-19 infection, it was felt that her aortitis was COVID-19 related. For this, the patient was initiated on prednisone 60mg daily after her negative infectious work up with subsequent resolution of her abdominal pain. Repeat imaging and labs at 2 weeks demonstrated resolution of aortic findings (Panel B) and normalization of inflammatory markers. Her prednisone was tapered over a 6-week course without recurrence of symptoms.
Conclusions: Aortitis should be recognized as a potential complication related to COVID-19 infections. While aortitis is associated with significant morbidity and mortality, early initiation of corticosteroids can lead to favorable outcomes.
Poster 52 Panel A and B.

Poster Number: 53
Abstract Number: 1261312
Complications of vascular Ehlers-Danlos syndrome
Eri Fukaya, MD, PhD,
Stanford University
Background: This case highlights the diagnosis and treatment of a rare vascular complication associated with vascular Ehlers-Danlos syndrome (vEDS).
Case presentation: 23M with a history of spontaneous splenic aneurysm rupture and headaches since childhood presented for evaluation. On examination, he has myopia correction since 3rd grade, a triangular face, slight enophthalmos, a small jaw with dental crowding and flexible fingers and joints but otherwise unremarkable. CTA showed multiple small segment dissections in the bilateral internal carotid artery (ICA). Aneurysmal dilation and pseudoaneurysm were also seen in the ICA and vertebral arteries. Subsequent genetic testing revealed COL3A1 gene mutation consistent with vEDS. 18 months later, he developed severe headaches with pulsatile tinnitus and nausea. CT at local ER was negative for stroke. Over the next week, symptoms worsened and he developed gait instability, light sensitivity, blurry vision looking to the left and pain extending from the occipital head to the left eye. Repeat CTA showed new aneurysms in the cavernous portion of the left ICA and right MCA but he was instructed to follow up outpatient. The patient presented to clinic 3 days later. He was ill appearing and had ongoing headache with nausea. He had light intolerance, ipsilateral ptosis, mild conjunctival injection and -3 abduction consistent with left CN VI palsy. The constellation of symptoms was concerning for direct carotid cavernous fistula (CCF). Subsequent cerebral angiogram revealed a direct Barrow Type A left CCF arising from a ruptured cavernous segment aneurysm and steal from the left anterior circulation. The patient underwent transvenous coiling of the left CCF. Balloon occlusion test of the left ICA was performed under neurologic monitoring while coiling of the left cavernous sinus was performed. Completion angiogram showed absent AV shunting and restoration of antegrade flow to the left anterior circulation. Post procedure, he received Decadron 4mg q6hrs with a 10-day taper. His photophobia resolved and vision is improving. He continues to have headaches, but his gait normalized.
Conclusions: It is important to recognize the development of a CCF in a patient with vEDS to provide appropriate treatment.
Poster 53 Panel A-C.

Poster Number: 54
Abstract Number: 1277445
Good things don’t always come in small packages: Idiopathic small-vessel vasculitis
Vanderbilt University Medical Center
Background: 56-year-old female with stage IV breast cancer on palliative chemotherapy, who presented with digit ischemia.
Case presentation: She was smoking 4-6 cigarettes daily which she quit soon after her finger symptoms started. She underwent an extensive thrombo-embolic search with no underlying etiology. A calcium channel blocker and therapeutic anticoagulation was initiated without improvement. Her right fourth digit demonstrated distal necrosis without purulence (Panel A). On exam, distal pulses were difficult to palpate, there was acrocyanosis of all toes which were cool and tender to touch. Labs showed a positive speckled pattern ANA (titer ⩾1:2560), mildly positive rheumatoid factor, and negative APLS and ANCA. Selective extremity angiography demonstrated severe calcific ischemic changes of both hands and the left lower extremity with very mild evidence of corkscrewing out of proportion to her presentation (Panels B and C). Given her significantly elevated ANA, smoking cessation, and lack of more significant pathognomonic angiographic findings for thromboangiitis obliterans her small vessel vasculitis remains idiopathic. She remains on doxazosin and therapeutic anticoagulation with limited improvement in her symptoms. After discussion with her Oncologist, she was started on prednisone and methotrexate. She has had limited improvement of her toe ischemia and progression of left-hand ischemia since initiation of prednisone and methotrexate.
Conclusions: Progressive small vessel vasculitis and digital ischemia in the setting of stage IV breast cancer in a former smoker. The timing of her breast cancer progression and digital ischemia raises suspicion for a paraneoplastic etiology of her small vessel vasculitis.
Poster 54 Panels A-C.

Poster Number: 55
Abstract Number: 1273773
Kissing carotids: A case of incidental found bilateral retropharyngeal carotid arteries
Cleveland Clinic Foundation
Background: Retropharyngeal carotid artery is an unusual rare anatomic variation that can be sometimes missed in imaging reports. Most cases reported are incidental findings in asymptomatic patients, however some can present with nonspecific symptoms. We hereby present a case of asymptomatic patient retropharyngeal carotids found incidentally on imaging.
Case presentation: A 65-year-old female past medical history significant for PAD and non-small lung cancer undergoing radiotherapy. She followed up with vascular medicine for PAD. Serial CT imaging is performed to monitor malignancy. A CT neck revealed retropharyngeal carotid arteries bilaterally with moderate calcifications near the carotid bifurcation (Panel A). Carotid US has been done that revealed plaque in the common carotid, subclavian and internal carotid arteries bilaterally. In addition, bilateral 20-39% ICA stenosis and right subclavian stenosis 50-99% has been reported based on the Cleveland Clinic Vascular Lab criteria.
Conclusions: Cases of unilateral carotid retropharyngeal artery have been reported, in rare cases bilateral carotid arteries are identified, this finding is usually referred to as “kissing carotids”. Identifying and reporting such finding is important because it helps in avoiding complications during endotracheal intubation or surgical procedure. In this case we discuss a patient who has reported past successful endotracheal intubations with no complications. She has been found to have an incidental finding of bilateral retropharyngeal carotid arteries, this finding was important to be reported specially in setting of lung malignancy and possible anticipated future surgeries.
Poster 55 Panel A.

Poster Number: 56
Abstract Number: 1273802
Downhill esophageal varices: Rare cause of esophageal varices
Cleveland Clinic Foundation
Background: Downhill esophageal varices are common consequence of SVC obstruction, they are usually formed in upper two-thirds of the esophagus. We hereby present a case of esophageal varices in setting of SVC obstruction
Case presentation: A 65-year-old gentleman, with past medical history significant for ESRD on intermittent dialysis complicated by multiple malfunctioning arteriovenous fistulas including prior brachiocephalic vein and caudal superior vena cava (SVC) stenosis with repair presented to the emergency department with abdominal pain. The abdominal CT scan on presentation showed diverticulitis and numerous venous collaterals in the abdominal wall at the gastroesophageal junction. Colorectal surgery was consulted and recommended further evaluation for causes of portal hypertension given that the collateral vasculature was in the potential surgical field. Subsequent liver vascular ultrasound showed patent hepatic vasculature without evidence of cirrhosis. Subsequently, CTA chest showed occlusion in the distal SVC with multiple collaterals in the chest, abdominal wall, and mediastinum. A bilateral upper extremity venogram showed extensive thrombus involving the bilateral axillary, subclavian, innominate veins, and superior vena cava. Subclavian, innominate veins, and superior vena cava. In addition, right subclavian retrograde flow has been noted.
Conclusions: We are reporting a case of esophageal varices in setting of SVC obstruction. Usually esophageal varices present with upper GI bleed in setting of liver disease. In our case, CT abdomen showing multiple venous collaterals on CT abdomen, necessitated further investigates. Suspicion of SVC obstruction in setting of esophageal varices should be high especially in setting of AV fistulas and or with a history of a central catheter, in patients with no stigmata of chronic liver disease.
Poster 56 Panels A-F.

Poster Number: 57
Abstract Number: 1269089
Acute upper limb ischemia and a large cardioembolic infarct in an elderly female presenting with multiple intracardiac thrombi
Angela Apostol-Alday, MD, FPCP, FPCC, FPSVM,
Central Luzon Doctors Hospital
Background: Acute upper limb ischemia accounts for less than 5% of total cases of limb ischemia. Embolic phenomenon is still the most common etiology. There are no guidelines for evaluation and management that is specific for the upper extremity. We report a case of a patient who presented with a large acute ischemic stroke then subsequently had acute upper limb ischemia caused by emboli from intracardiac source.
Case presentation: A 67-year-old female with no previously diagnosed comorbidities, presented at the emergency room of our institution with difficulty of breathing associated with hemodynamically unstable supraventricular tachycardia. After successful resuscitation, supraventricular tachycardia deteriorated to atrial fibrillation with rapid ventricular response. Patient also had right hemiplegia and aphasia and was confirmed to have a massive infarct involving the left middle cerebral artery territory. Echocardiogram showed multiple intracardiac thrombi with global hypokinesia and an estimated ejection fraction of 36%. Follow-up examination on day 1 of hospitalization showed cyanosis of the left hand. The left upper extremity was cold to touch up to the level of the antecubital fossa. There were absent arterial signals on the left radial, ulnar and distal brachial on handheld Doppler. Because of the contraindication to anticoagulation and refusal to undergo revascularization, she was started with a glycosaminoglycan (GAG) in the form of sulodexide. Gradual improvement in the left upper extremity was noted 48 hours after starting sulodexide. No bleeding episodes were observed. Patient was eventually discharged after 2 weeks with a beta-blocker, statin, antiplatelet and an anticoagulant and was advised for close follow up.
Conclusions: Acute limb ischemia becomes a management dilemma when complicated by conditions precluding anticoagulation or posing high-risk for perioperative morbidity and mortality. In this particular case, GAG was shown to improve the ischemic signs and symptoms without the added risk of bleeding.
Poster Number: 58
Abstract Number: 1272311
Acute upper limb ischemia as initial presentation of COVID-19 infection in a 49-year-old male: A case report
Angela Apostol-Alday, MD, FPCP, FPCC, FPSVM,
Central Luzon Doctors Hospital
Background: Coronavirus disease-19 (COVID-19) is an emerging threat because of its significant damage to the lungs and its risk of thrombosis in microvascular, venous, and arterial beds. Moreover, thrombosis in patients with the COVID-19 infection may also be more extensive, leading to limb loss and death. One of the thrombotic complications reported in COVID-19 is acute limb ischemia (ALI), which is characterized with an abrupt decrease in the arterial perfusion of a limb, threatening its viability and integrity. In this report, we describe an unusual case of an unvaccinated patient who presented with acute unilateral upper extremity ischemia as the initial manifestation of COVID-19.
Case presentation: A 49-year-old man, unvaccinated for COVID-19, presented to the emergency room due to worsening left hand and forearm pain of one week duration. The brachial, radial, and ulnar pulses were absent. Emergency arterial duplex scan of the left arm showed acute thrombi totally occluding the lumen of axillary artery and extending to the proximal to distal brachial, proximal to distal radial and ulnar arteries. Anticoagulant infusion in the form of heparin was immediately started was titrated accordingly depending on aPTT. Surgical embolectomy was offered but could not be immediately done within 6 hours of presentation due to positive result for SARS-CoV2. Patient denied history of respiratory symptoms and was also noted to have normal lung findings. During surgical embolectomy, a significant amount of large, elongated acute thrombi were retrieved. Anticoagulation was resumed post-operatively and no signs and symptoms of compartment syndrome were noted. Patient slowly recovered his sensory and motor functions within a month from onset of ALI.
Conclusions: Thrombotic events such as acute limb ischemia may be the initial manifestation of COVID-19 infection. In this patient, what we found particularly peculiar was that he had no respiratory symptoms despite being unvaccinated during the time that the Delta variant was the prevailing strain of coronavirus. This case underscores the fact that clinicians should have high index of suspicion of COVID-19 infection as a cause of thrombotic events, especially in patients with no or very few risk factors.
Poster 58 Panel A and B.

Poster Number: 59
Abstract Number: 1272137
A missed ruptured abdominal aortic aneurysm in a paraplegic patient
1University of California Riverside School of Medicine, 2Loma Linda University Medical Center
Background: Abdominal aortic aneurysms (AAA) classically present as a triad of hypotension, abdominal/flank pain, and a pulsatile abdominal mass in males over 65 and with a history of smoking. Here, we present a unique case of a missed ruptured AAA (rAAA) in a paraplegic patient atypical of the classical at-risk patients, where complications led to limb ischemia and resulting cryoamputation.
Case presentation: This case describes a 54-year-old male patient with T2 paraplegia, who presented to the ED for generalized fatigue. The patient initially presented with hypotension and tachycardia, but with strong distal pulses to the bilateral lower extremities. Hospital workup revealed severe electrolyte imbalance, absent urinary output, and a complete collapse of the inferior vena cava on inspiration. After returning from CT to evaluate for acute renal failure, however, the patient again became hypotensive and was noted to have absent dorsalis pedis pulses with cold extremities. An incidental finding of a 7.47 cm rAAA (Panel A) on CT scan was found 12 hours after ED presentation and medical ICU admission and immediate abdominal endovascular aneurysm repair (EVAR) was performed. However, acute limb ischemia rendered the right lower extremity unsalvageable and cryoamputation was performed. The patient was ultimately discharged to a long-term care facility after a two-month hospital stay.
Conclusions: This case both outlines the relative lower efficacy of the physical exam when evaluating for AAA– especially in paraplegic patients lacking sensation in the abdomen and below– and potentially demonstrates the benefits of performing the Rapid Ultrasound for Shock and Hypotension (RUSH) exam in patients with unknown sources of shock, which likely would have identified the presence of an AAA prior to rupture.
Poster 59 Panel A.

Poster Number: 60
Abstract Number: 1265519
Rare adverse event following cyanoacrylate closure of greater saphenous vein
1Presbyterian Hospital, 2Stanford University
Background: Cyanoacrylate glue closure of symptomatic venous reflux has similar rates of long-term closure as thermal ablation with the benefits of avoidance of tumescent anesthesia and thermal injury. Here, we report a rare adverse event associated with cyanoacrylate glue use.
Case presentation: 82M with non-healing mixed arterial and venous ulcer underwent treatment of venous reflux in the right great saphenous vein (GSV) with cyanoacrylate glue using Venaseal closure system (Medtronic, Minneapolis, Minn). His wounds healed completely, however, 2 months later he developed a lump in the medial knee with increased leg swelling. He also developed fistulas along the medial aspect of his leg with extrusion of thick viscous material. Ultrasound showed irregular cystic tissue suspicious for foreign body granuloma along the medial aspect of the knee and lower leg. He was treated with intra-lesional and systemic steroids. This resulted in significant improvement however, the wounds worsened after completion of the prolonged steroid taper. He did not develop fever, chills or leukocytosis during this time period. Empiric antibiotics did not have any significant clinical effect on the granuloma formation. Eventually, excision of the below knee GSV and complete excision of the right groin mass was performed. Histopathology showed granulomatous lesions. Groin granuloma included pellets that likely represented extruded glue casts with no growth in cultures. All wounds healed however, a few weeks later, he developed a new lesion in the distal thigh where there was residual cyanoacrylate. He subsequently underwent excision of remainder of GSV with complete resolution of his symptoms.
Conclusions: This is a case of an exaggerated immune response to cyanoacrylate glue leading to destruction of vein wall, development of foreign body granulomas around extruded glue and fistulas with extrusion of glue to the exterior. Treatment ultimately required complete resection of the foreign object. We discuss the clinical presentations and some possible mechanisms for this rare adverse event.
Poster 60 Panels 1-4.

Poster Number: 61
Abstract Number: 1273302
Vascular Ehlers-Danlos Syndrome: a case of leaking intracranial and intraabdominal aneurysms
University of Virginia
Background: Vascular Ehlers-Danlos Syndrome (vEDS) is a rare inherited disorder that arises due to a genetic defect in type III collagen synthesis and predisposes to rupture of arteries and hollow organs. Unfortunately, the diagnosis of vEDS is often delayed until patients present with severe sequelae of their disease.
Case presentation: A 43-year-old male presents with an acute subarachnoid hemorrhage secondary to a leaking intracranial aneurysm for which he underwent embolization. He had spontaneous pneumothorax in childhood. His family history was remarkable for a spontaneous pneumothorax and the premature death (attributed to alcohol abuse) of his father around age 45. CT revealed mediastinal and subpleural hematomas, severe emphysema, multifocal dissections (left vertebral artery, left common iliac artery), and multifocal aneurysmal disease (celiac artery, splenic artery, superior mesenteric artery, and bilateral renal arteries). Later the patient acutely decompensated with tachycardia, hypotension, and altered mental status prompting emergent intubation. Repeat imaging showed new dissections (bilateral vertebral arteries, right common iliac artery), development of moderate volume hematoperitoneum for which he underwent embolization of a leaking splenic artery aneurysm, and cerebral vasospasm with delayed cerebral ischemia. Differential diagnosis included segmental arterial mediolysis, connective tissue disorders, and other inflammatory conditions. A serologic evaluation was negative for rheumatologic and vasculitic processes. Genetic testing reported COL3A1 mutation consistent with vEDS.
Conclusions: The diagnosis of vEDS requires a high degree of suspicion based on clinical presentation and family history and can be confirmed with genetic testing.
Poster Number: 62
Abstract Number: 1270095
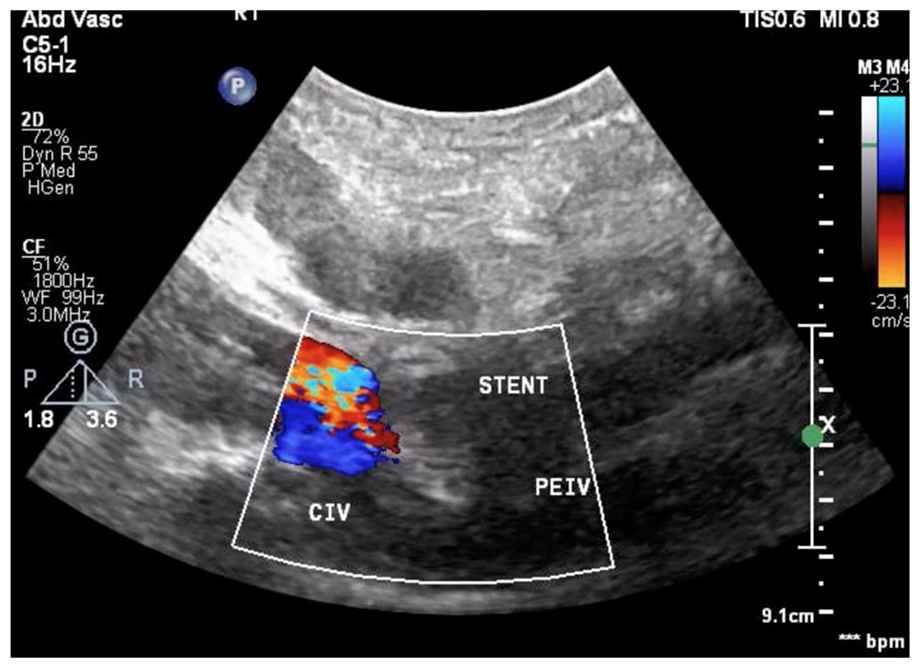
Recanalization of an occluded vena cava filter and iliac veins to treat post-thrombotic syndrome with venous stasis ulcers
University of Louisville School of Medicine
Background: Anticoagulation (AC) is first-line therapy for inferior vena cava (IVC) filter thrombosis. However, in cases of extensive iliofemoral deep vein thrombosis (DVT) in the presence of obstructed IVC filter with venous stasis ulcers (VSU), AC is often unsuccessful.
Case presentation: A 30-year-old female with IVC filter placed for failure of AC and frequent DVT presented with recurrent VSU of bilateral lower extremities. On venogram, she was found to have thrombosis of bilateral common iliac veins (ILV) and the distal IVC, with an IVC filter at infrarenal location. The patient was started on thrombolysis which had to be discontinued due to rapid drop in fibrinogen. Mechanical thrombectomy was performed bilaterally followed by balloon angioplasty of ILV and IVC. There was no flow visualized in ILV post-angioplasty. We deployed two self-expanding stents (SES) on the right side and two SES on the left side. The stents extended from origin of the external ILV into the IVC to the level of the renal veins, across the previously placed IVC filter. All stents were post-dilated. Venography after stent deployment showed excellent flow bilaterally, with both ILV and IVC widely patent. The patient tolerated the procedure well and had complete resolution of her symptoms.
Conclusions: We present a unique case of invasive treatment of recurrent VSU in a patient with frequent DVT and IVC filter thrombosis who had failure of AC and could not tolerate thrombolysis. Stenting of obstructed IVC filter in patients with VSU is safe and can help in resolution of symptoms.
Poster 62 Panels.

Poster Number: 63
Abstract Number: 1273789
Atraumatic radial and ulnar artery thrombotic occlusion resulting in critical limb ischemia triggered by black mold infestation
University of Colorado Anschutz School of Medicine
Background: Atraumatic upper extremity arterial thrombosis is uncommon. We present a case of radial and ulnar artery thrombosis with critical limb ischemia, with symptoms resolving after remediation of a black mold home infestation. This case highlights the importance of identifying potential environmental exposures in uncommon clinical presentations.
Case presentation: Chart review of all visits in two hospital systems. Informed consent was obtained from the patient. Results: A 51-year-old male noted pain and paresthesia of the left hand. Critical ischemia was found with mid-forearm occlusion of the radial and ulnar arteries; surgical care included no distal target for bypass and digital ray amputation. Workup did not reveal autoimmunity, thrombophilia, or source of embolism. Symptoms were recurrent with ongoing ischemia and tissue loss. Further evaluation identified a home water leak. Professional remediation of black mold coincided with resolution of pain, discoloration, and ulceration without return of symptoms at follow up of 22 months.
Conclusions: Immune-mediated mechanisms can lead to clinical thrombotic events. Vascular occlusion related to COVID-19 has stimulated interest in thrombotic pathways not routinely emphasized. We postulate neutrophil extracellular traps (NETs), triggered by chronic exposure to mold, contributed to persistent digital ischemia. NETs are fibrous extensions of extracellular strings of DNA, antimicrobial peptides, and chromatin that bind pathogenic microbes and provide scaffolding for thrombi, triggering vascular occlusion. This is a novel case of upper extremity arterial occlusion leading to amputation associated with exposure to black mold. Thrombosis may be related to NETs formation and symptoms did not resolve until the environmental mediator was eradicated. Environmental exposure should be considered in otherwise healthy patients who present with atraumatic critical digital ischemia without thrombophilia, autoimmunity, illicit drug use, or vasculitis.
Poster Number: 64
Abstract Number: 1259433
A novel thrombolytic protocol for mechanical aortic valve thrombosis
1Northwell, 2Brown University
Background: Subtherapeutic anticoagulation (AC) of mechanical aortic valves (MAV) can lead to thrombosis causing obstruction. Hyperdynamic left ventricular (LV) systolic function, elevated LV outflow tract velocity, and aortic insufficiency (AI) can be seen on echocardiogram (TTE) due to changes in transvalvular gradient. Thrombolytics (tPA) are used in high-risk candidates while surgery is done in low/moderate risk candidates and those with large clots. Our case shows a high-risk candidate treated with a novel tPA protocol that resulted in the resolution of aortic valve obstruction.
Case presentation: 54-year-old female with MAV underwent abdominal surgery where AC was held now presenting with cardiogenic shock. TTE showed new severe aortic stenosis (AS) due to leaflet restriction from a large thrombus along with new AI, which precluded mechanical circulatory support. She was a poor surgical candidate and was given 50mg of alteplase at a rate of 8.3 mg/dl along with low intensity IV heparin. After 2 hours, TTE showed resolution of AI and significant improvement of AS. Unfortunately she experienced cardiac arrest due to other reasons and failed to respond to multiple rounds of resuscitation. Hemoglobin checked during the code blue was stable, ruling out hemorrhage as the cause of death.
Conclusions: tPA infusion for AV thrombosis is generally recommended at an ultraslow rate of 25mg over 25 hours followed by IV heparin 6 hours post infusion. Given the instability of our patient, we administered 50mg of tPA over 6 hours, simultaneously with heparin, which led to the resolution of AI and improved transvalvular gradients. Observational studies indicate lower complication rates with the ultraslow protocol, but it can fail in those with severe symptoms or larger thrombus burden. Our case demonstrates a new protocol that can be considered in patients with hemodynamically unstable AV thrombosis.
Poster Number: 65
Abstract Number: 1273401
A rare case of pulmonary artery dissection: Prevent so you don’t have to treat!
1University of Wisconsin Health, 2 University of Illinois College of Medicine
Background: Pulmonary artery dissection (PAD) is a rare fatal complication of chronic pulmonary hypertension. Less than 200 cases were reported since 1842. It can lead to sudden cardiac death by causing cardiac tamponade secondary to hemopericardium. Here, we report a rare case of PAD with a discussion about the possible presentations, diagnosis, and management.
Case presentation: A 66-year-old man with a medical history of pulmonary hypertension WHO group 2,3,4, COPD GOLD III on chronic oxygen therapy 4 L and HFprEF. He presented to the emergency department with increased shortness of breath and oxygen requirement up to 6 L for one week. He reported leg edema too. He had no chest pain. Clinical examination revealed an elevated JVP, and an accentuated pulmonic component S2. He was afebrile, respiratory rate was 20, oxygen saturation 92% on 44 % FiO2. Heart rate was 102 and BP 114/83. Blood work was significant for elevated measured bicarb at 37, reduced E-GFR 66, elevated ALP 107, and elevated BNP 224. Chest X-ray showed pulmonary edema. EKG showed NSR, right atrial, right ventricular enlargement and right bundle branch block. CT angiogram of the chest showed an intimal flap consistent with dissection of the proximal main pulmonary artery extending into the proximal right main pulmonary artery as shown Panels 1 and 2. TTE showed EF 54%, grade 1 diastolic dysfunction, RVSP 79 mm Hg, mild right ventricular dilation and moderate right atrial dilation. He was managed with diuresis, beta-blockers. Riociguate was continued for pulmonary hypertension. The patient was transferred to a tertiary care facility for surgical management .
Conclusions: Pulmonary artery dissection is a life-threatening condition that should be considered when a chronic pulmonary hypertension patient presents with chest pain or SOB. The diagnosis is best made by CT angiogram. The best-suggested management is medical management with diuretics, vasodilators, and beta-blockers followed by surgical management. That said, proper management and prevention of pulmonary hypertension in patients with lung and heart disease is the most effective tool in preventing that kind of fatal complication.
Poster 65 Panels 1 and 2.
Poster Number: 66
Abstract Number: 1272705
The revenant. A perilous acute aortic syndrome
Dr HB Calleja Heart and Vacsular Institute
Background: Acute aortic syndrome is a rare, life-threatening condition that may present as one of the following: acute aortic dissection, intramural hematoma or penetrating atherosclerotic ulcer.
Case presentation: Herein, we report a rare case of a three-in-one lesion in a single aorta of a hypertensive, 30 pack-year smoker 63-year-old Filipino male who presented with loss of consciousness. A CT Aortogram was requested from a widened mediastinum clue on chest xray which showed long segment abdominal aortic dissection with entry point at the proximal abdominal aorta and re-entry at the left external iliac artery, short segment thoracic aortic dissections, distal aortic arch and proximal descending aorta, penetrating aortic ulcers, proximal abdominal aorta. Intramural hematomas, ascending aorta, brachiocephalic artery, left subclavian artery, main pulmonary trunk, and both main pulmonary arteries. He underwent ascending branch and total arch replacement Type III arch debranching with modified frozen elephant trunk (antegrade deployment of valiant thoracic stent graft size (32-39) with TEE. Other lesions in the aorta were long segment abdominal aortic dissection with entry point at the proximal abdominal aorta and re-entry at the left external iliac artery. Intraoperatively he was diagnosed to have had acute aortic syndrome, aortic dissection, Stanford B Debakey III, non-A, non-B thoracic aortic dissection with retrograde dissection, Intramural hematoma - ascending aorta and arch branches, penetrating ulcers at the proximal abdominal aorta. He was discharged improved on 19th hospital day from a regular unmonitored bed. He was on beta blockers, statin, ARNIs, antiplatelet, and colchicine. Instructions were given on target blood pressure, heart rate and avoidance of straining. Repeat CT aortogram was scheduled 3 months after post discharge.
Conclusions: Our report highlights a rare case of a successfully timed surgical intervention for a life threatening acute aortic syndrome presenting with aortic dissection, intramural hematoma and penetrating atherosclerotic ulcer. A first in the institution and third in the country.
Poster Number: 67
Abstract Number: 1275541
Successful percutaneous retrieval of embolized MitralClip - an extremely rare complication
Mount Sinai Hospital
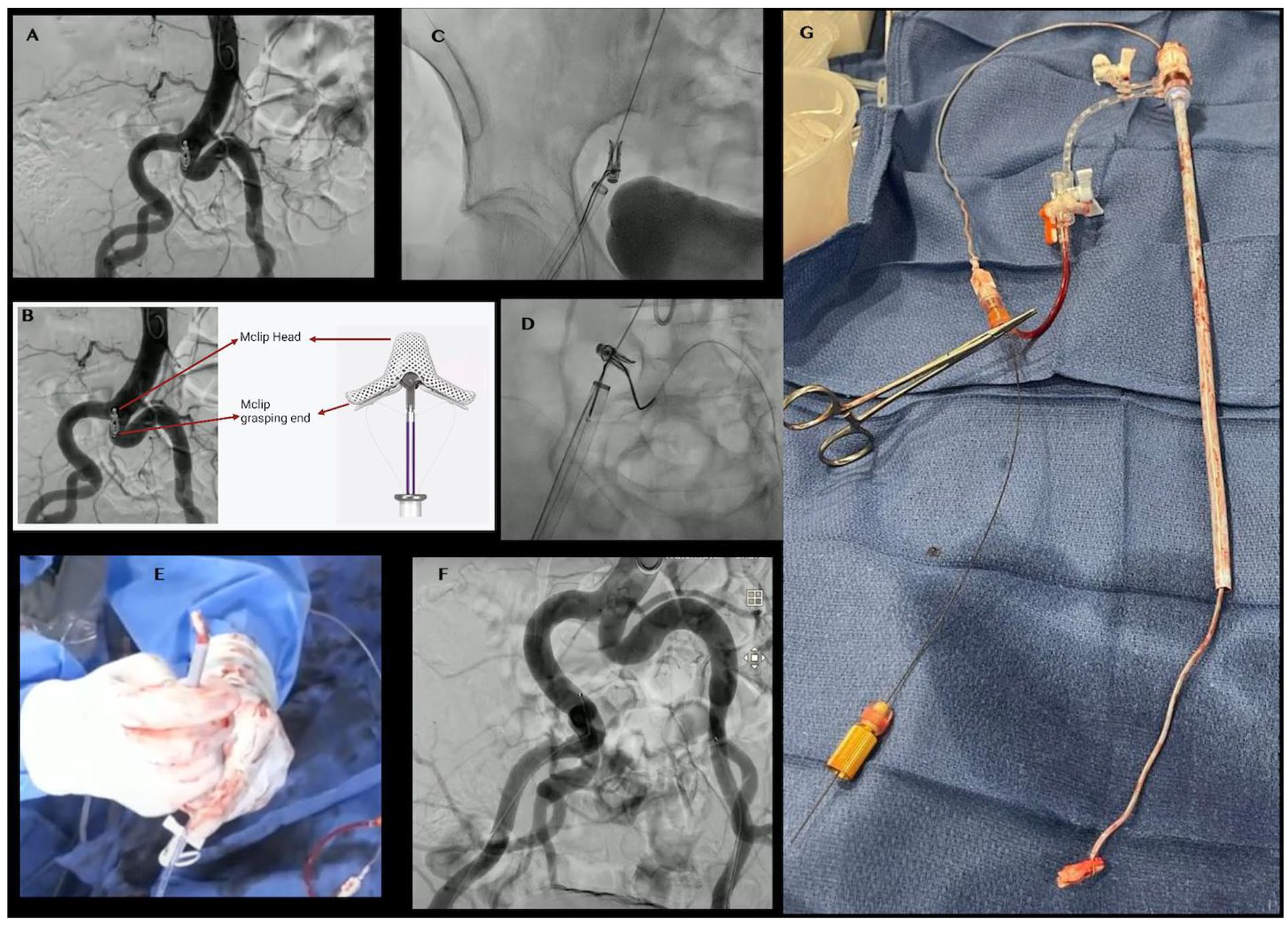
Background: The number of endovascular and intracardiac procedures performed is increasing exponentially as technology improves and device migrations can be encountered in contemporary practice.
Case presentation: An 81-year-old female with s/p MitralClip (Mclip) for severe mitral regurgitation presented with a recurrent CHF exacerbation. A new finding after the Mclip procedure revealed recurrent severe mitral regurgitation on echocardiogram. With the failure of the Mclip procedure, mitral valve replacement was planned. Fluoroscopic examination of iliac arteries revealed a migrated Mclip in the proximal part of the left common iliac artery (CIA). (Panel A) Multiciliary team discussion, including the cardiothoracic surgeon, interventional cardiologist, and the endovascular surgeon, was performed and collectively decided to proceed with mitral valve replacement first, followed by the removal of the migrated mitral clip. Analysis of migrated mitral clip revealed the head of Mclip was closed to the right CIA. (Panel B) Hence, the right femoral artery (RFA) was used as the primary access site with a plan to capture the clip from the head of Mclip. Triple vascular accesses via right and left femoral and right radial arteries were obtained. As the width of the mitral clip ranges from 4-6mm, 18F sheath size from RFA with a backup plan to upsize the sheath to 22F. Another consideration was to use two supracore wires from RFA with a plan to remove Mclilp and sheath together in case of inability to remove the Mclip through the sheath. First, Amplatz Gooseneck snare (Medtronic) and EN Snare (Merit Medical Systems) were used to grasp the Mclip via RFA without success. Then, a gooseneck snare was used to capture the clip from LFA with a plan to push up the clip. Subsequently, another gooseneck snare via RFA was used to grasp and remove the Mclip but many challenges were encountered probably due to severe tortuosity in the iliac artery. Finally, both the sheath and Mclip with gooseneck snare were required to remove with the placement of a new sheath. A final angiogram revealed no dissection or perforation seen.
Conclusion: It is paramount to be aware of such complications and the feasibility of the percutaneous removal technique.
Poster 67 Panels A-G
Poster Number: 68
Abstract Number: 1272222
The approach to a patient with superficial femoral artery aneurysm with concomitant mycosis due to an infected baker’s cyst
St. Luke’s Medical Center Quezon City
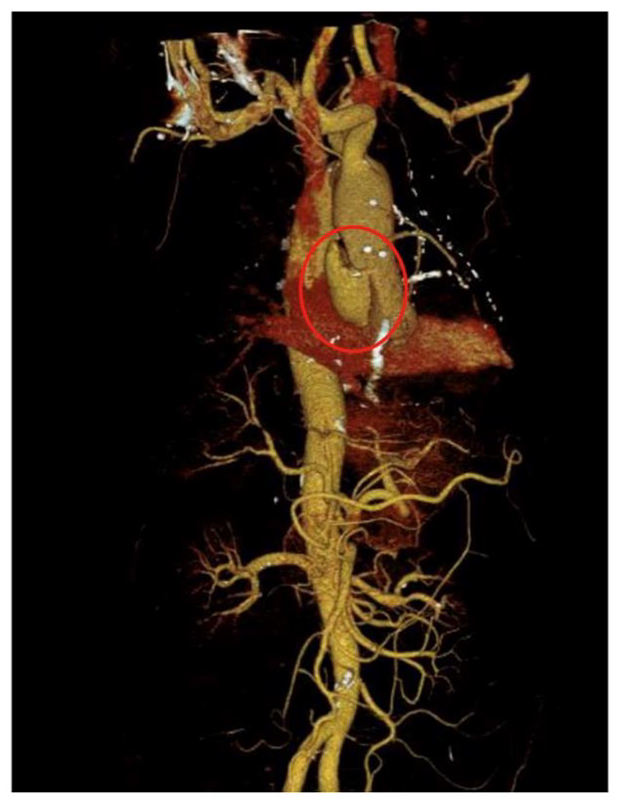
Background: Superficial femoral artery aneurysm is a rare disease usually discovered in elderly male patients. Presence of bacteremia from multiple infections could establish a vascular infectious focus.
Case presentation: This is a case of an 89-year-old male with a known case of left lower extremity superficial femoral artery aneurysm who presented with a two-week history of high-grade fever. Focused physical examination showed an inflamed and pulsatile mass from the popliteal region to the distal thigh. Imaging studies revealed a large and infected Baker’s cyst distal and below the stable-sized superficial femoral artery aneurysm. This was managed as superficial femoral artery mycotic aneurysm which is associated with significant morbidity and mortality. Treatment-changing factors include type and timing of interventions, patient co-morbidities and infection recurrence. A multidisciplinary approach is recommended to help weigh the risks and benefits of each possible treatment strategy.
Conclusions: This is a case of superficial femoral artery aneurysm with concomitant bacteremia leading to a diagnosis of mycotic aneurysm. Treatment should be patient-specific as there are no management-guiding studies currently available.
Poster 68 Panel.

Poster Number: 69
Abstract Number: 1280331
Surgical repair of a large type A symptomatic penetrating atherosclerotic ulcer complicated with pseudoaneurysm and severe aortic regurgitation in a 66-year-old male
St. Luke’s Medical Center
Background: Penetrating atherosclerotic ulcers (PAU) are typically seen in hypertensive elderly male patients with a history of coronary artery disease. It accounts for approximately 7.5% of all cases of acute aortic syndrome and is usually located in the descending aorta.
Case presentation: This is a case of a 66-year-old male who came in due to 2 hours history of sudden 10/10 substernal chest pain associated with headache and dizziness. Point-of care ultrasound revealed an intimal flap in the posterior wall of the aortic root with severe aortic regurgitation. CT aortogram showed a large penetrating aortic ulcer with pseudoaneurysm formation measuring 3.2 x 3.3 x 6.2 cm along the right posterolateral aspect of the ascending aorta. A bentall procedure with bioprosthetic valve and vascular prosthetic graft and coronary artery bypass graft was done. Unfortunately, the patient died because of cardiogenic shock due to stunned myocardium.
Conclusions: PAU in the ascending aorta is uncommon and is fatal when it ruptures. Even though mortality rate is high (15-20%), an open surgical intervention is recommended for these cases as certain ulcers are not anatomically favorable to an endovascular approach due to the location, aortic dimensions or the inability to gain access given the frequently extensive atherosclerotic burden of these patients.
Poster 69 Panel.
Poster Number: 70
Abstract Number: 1279087
Diagnosis and management of vascular complications of fibrosing mediastinitis
1Creighton University, 2Children’s Hospital and Medical Center
Background: Calcified granulomas are a common imaging finding in the American Midwest. While tuberculosis is a feared cause, Histoplasma capsulatum, a fungal pathogen is far more prevalent in the community. A rare and feared complication of the disease is fibrosing mediastinitis, where mediastinal masses can compress adjacent structures including mediastinal vasculature.
Case presentation: Here we will present three patients, who both initially presented with shortness of breath with pulmonary vascular compression due to fibrosing mediastinitis found on CT scan. With lack of improvement from medical therapy, two of the patients received endovascular intervention with durable results. One patient was found to have occlusion of the main pulmonary artery with chronically reduced respiratory function.
Conclusions: Endovascular treatment of fibrosing mediastinitis is important consideration. Even if radiographs and clinical exams are equivocal or negative, a CT scan is important to rule out vascular compression that maybe amenable to endovascular intervention. Given the natural history of the disease, it is important to obtain follow-up clinical and imaging follow-up.
Poster Number: 71
Abstract Number: 1279215
Fatty vascular masses-diagnosis and management of lymphovenous malformations
1Creighton University, 2Children’s Hospital and Medical Center
Background: Cutaneous lymphovenous malformations are rare, low flow lesions that are more common in the pediatric population. They can increase in size with patients age. Treatment is important to prevent complications such as pain, infections, and disfiguration. This case study will review typical presentation, imaging findings, and treatment for these low flow lesions.
Case presentation: The case discusses a pediatric patient who was found to have enlarging lower extremity mass during clinical follow-up. MR imaging of the affected region was performed demonstrating signal and morphological characteristics compatible with slow flow lymphovenous malformation. Endovascular intervention was chosen as the mode of treatment with successful sclerosis of lesions, and durable results on further clinical followup.
Conclusions: MRI imaging is useful for the diagnosis of lymphovenous malformations, which can present as growing slow flow lesions. Endovascular treatment can offer a durable result, while remaining minimally invasive.
Poster Number: 72
Abstract Number: 1278655
Unicorns can also have stripes: reactivated varicella zoster virus mediated vasculitis and fibromuscular dysplasia
Vanderbilt University Medical Center
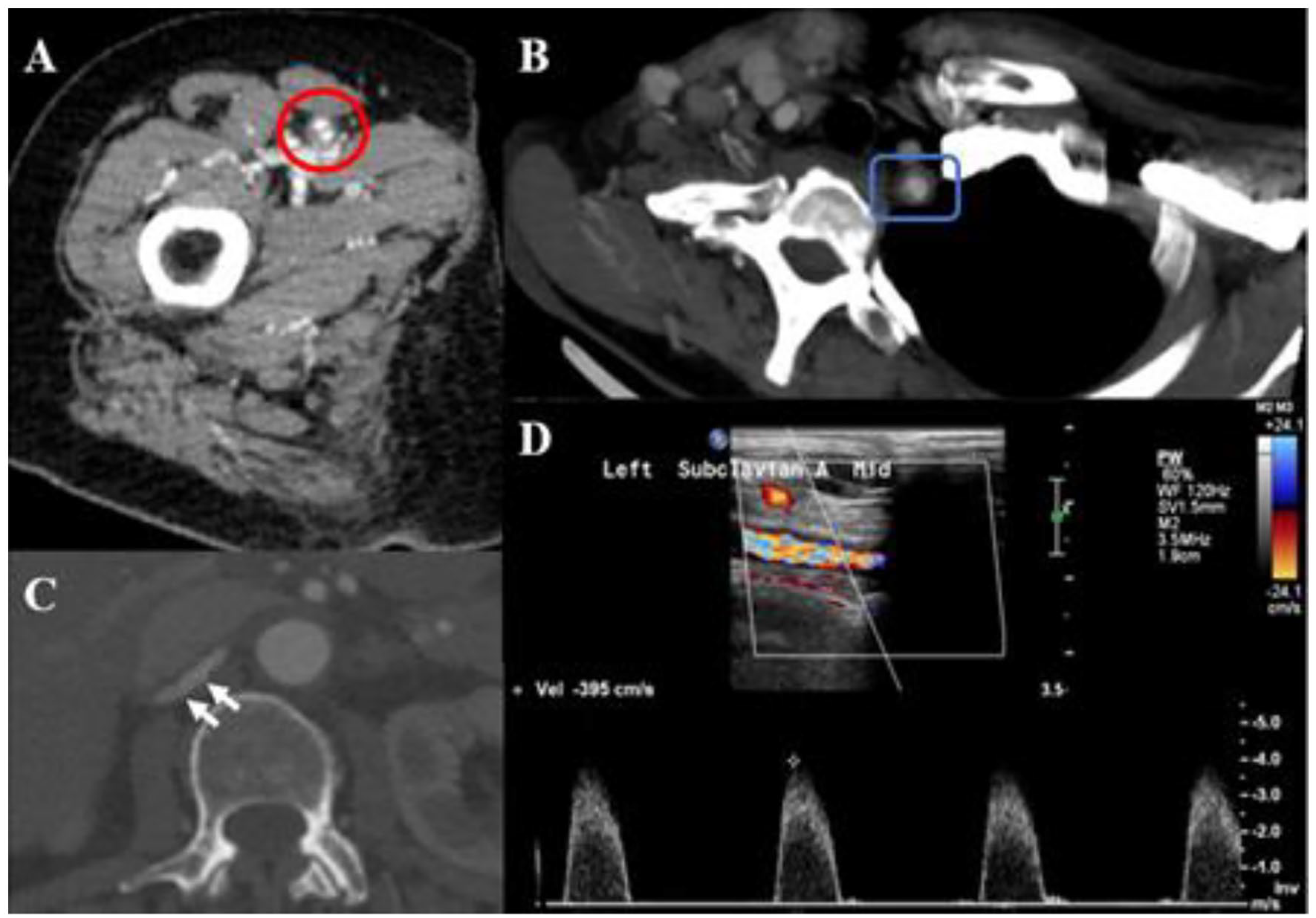
Background: 70-year-old female with history of prediabetes, former smoker (quit age 55) who developed reactivated Varicella Zoster Virus (VZV) and subsequent acute bilateral lower extremity pain with walking.
Case presentation: On exam, she was found to have reduced blood pressure in the left arm, left supraclavicular bruit, non-palpable right popliteal artery, palpable left popliteal artery, palpable PT bilaterally, non-palpable DP bilaterally. Labs demonstrated ESR 118 mm/hr (nL 2-37 mm/hr), CRP 18.1 mg/L (nL < 5mg/L), normal LDL. Right lower extremity ABI was abnormal with exercise. Given elevated inflammatory markers and new onset claudication, additional CT imaging was performed. She had concentric thickening of the right common femoral, superficial and popliteal arteries, with evidence of superficial femoral artery (SFA) dissection. There was diffuse concentric thickening of the left subclavian artery with evidence of significant stenosis on ultrasound. These findings were consistent with a large and medium vessel vasculitis in the setting of shingles. As her course of VZV resolved her inflammatory markers normalized and the SFA dissection completely resolved with normal exercise ABIs. On imaging her right renal artery also demonstrated a beaded appearance concerning for fibromuscular dysplasia (FMD), which remains the likely etiology for her SFA dissection.
Conclusions: This case represents a reactivated VZV large and medium caliber vessel vasculitis and FMD associated SFA dissection causing claudication. At the resolution of her VZV her claudication resolved, and inflammatory markers normalized without initiation of additional immunosuppressive therapy.
Poster 72 Panels A-D.
Poster Number: 73
Abstract Number: 1277538
Intracardiac echocardiography and simultaneous proximal embolic protection during inferior vena cava mechanical thrombectomy using the FlowTriever system
University of Connecticut
Background: Management of clot in transit in patients with pulmonary embolism, who are candidates for percutaneous intervention, can be challenging due to uncertainty of thrombus location during aspiration. This is a case report of simultaneous inferior vena cava and right atrial mechanical thrombectomy under real time intracardiac echocardiography guidance with proximal embolic protection using the FlowTriever system (Inari Medical Inc., Irvine, CA, USA).
Case presentation: A 52-year-old male with renal disease who had a craniotomy for glioblastoma resection surgery a month before presented for management of massive pulmonary embolism and clot in-transit in his inferior vena cava and right atrium. Intracardiac echocardiography during aspiration and pulling sheath down continuously visualized the partially protruded thrombus at the tip of the FlowTriever sheath and confirmed no-embolization under the proximal embolic protection disc clearly without need of using uncertain contrast injection.
Conclusions: Interventional cardiologists have the unique ability to apply cardiac imaging knowledge and use of innovative technologies to comprehensively address the percutaneous management of the thromboembolic disease processes. Real time intracardiac echocardiography can be safely and effectively used to visualize the retrieving clot from the inferior vena cava and cardiac chambers, in addition to standard fluoroscopy and angiography guidance while using the FlowTriever system. Intracardiac echocardiography can minimize use of contrast and avoid potential endotracheal intubation and mechanical ventilation, while providing good quality imaging to delineate proximal clot extent, thereby facilitating deployment of proximal embolic protection device.
Poster 73 Panels A-D.

Poster Number: 74
Abstract Number: 1273177
Multiple episodes of acute coronary syndrome: An uncommon presentation of medium-vessel arteritis
University of Massachusetts Medical School
Background: A 38-year-old male with a history of hypertension presented with atypical chest pain and stage II hypertension, as well as troponin elevation of 0.59 ng/mL, however left against medical advice due to an upcoming trip to his native country. The patient experienced recurrent symptoms while traveling and was reportedly admitted abroad to an ICU for 5 days. He subsequently returned to seek further care, re-presenting eight days after his initial encounter with recurrent hypertension and chest pain, found to have a troponin elevation of 0.34 ng/mL.
Case presentation: Investigations included echocardiography (within normal limits), unremarkable evaluation for secondary causes of hypertension, and cardiac catheterization. He was found to have a first diagonal with a mid-to-distal filling defect and likely intramural hematoma, suggestive of type 1 spontaneous coronary artery dissection (SCAD). CT angiogram of the abdomen and pelvis performed as part of fibromuscular dysplasia screening revealed findings suggestive of multifocal medium vessel arteritis involving the superior and inferior mesenteric arteries, the right colic artery, and the distal segments of the renal arteries. ESR was elevated at 29 and CRP at 55.8. The patient was initiated on prednisone, but developed corticosteroid toxicity, requiring IV cyclophosphamide infusions. The following year, the patient presented with an inferior ST segment-elevation myocardial infarction, due to SCAD of the right coronary artery. Prior site of dissection (D1) showed normal flow and appearance. A subsequent CTA showed improved pattern of vasculitis. His inflammatory markers had normalized.
Conclusions: This case describes a patient with polyarteritis nodosa and recurrent SCAD, which is likely under-recognized in this population.
Poster Number: 75
Abstract Number: 1278722
Porto-mesenteric venous thrombosis in patients with complicated intra-abdominal infections: a report of 2 cases
St. Luke’s Medical Center Quezon City
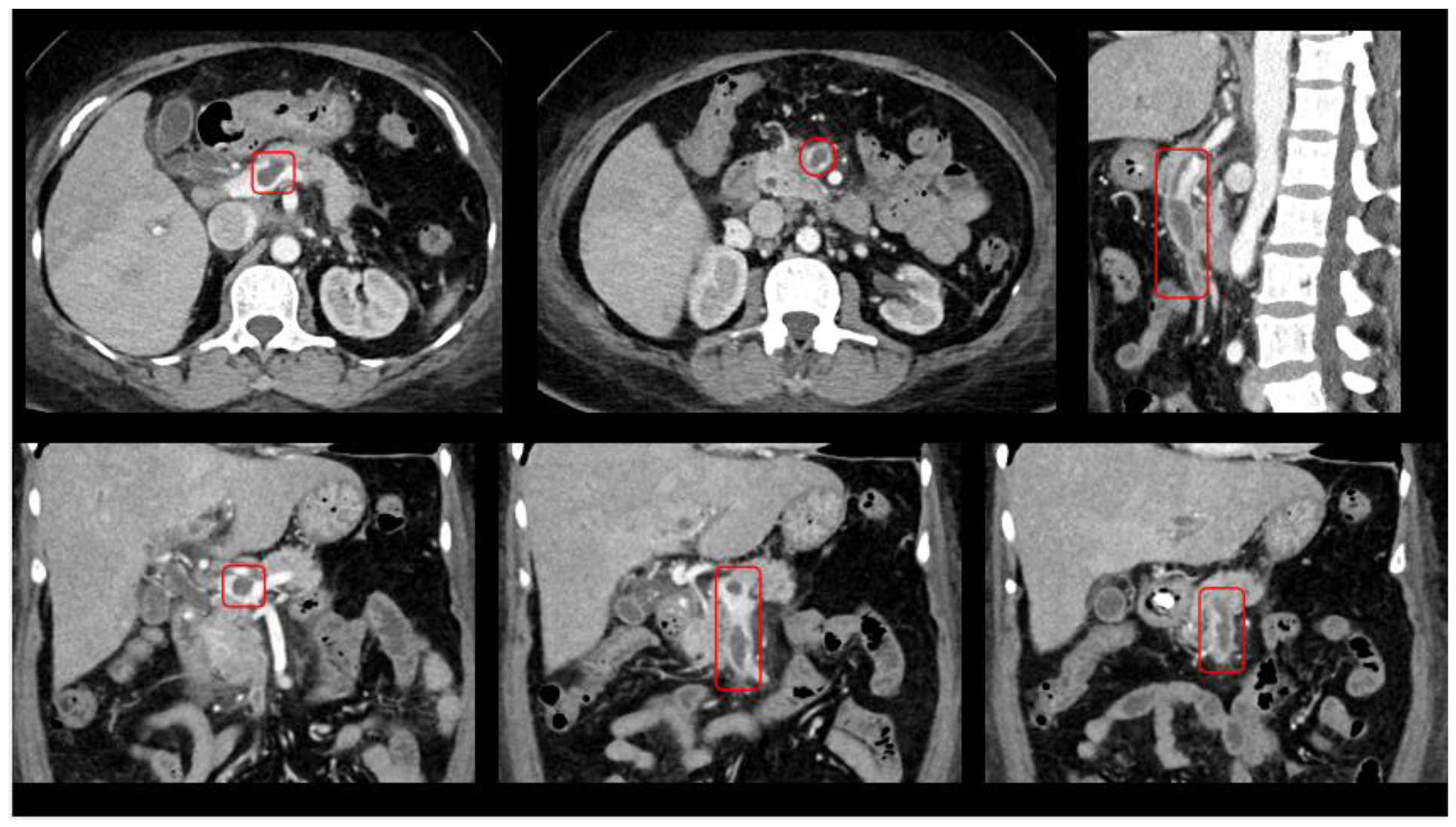
Background: Portomesenteric venous thrombosis is a rare disease, difficult to diagnose and can lead to mortality. Predisposing risk factors include pathologic conditions such as liver cirrhosis, malignancy, pancreatitis and other intra-abdominal infections or upper abdominal surgery. Pylephlebitis, a condition characterized by suppurative thrombosis of the portal vein can occur in patients with colonic diverticulitis.
Case presentation: This report discusses two cases initially both presenting with abdominal symptoms. Case 1 was a 69-year-old female who was admitted due to chief complaint of persistent diarrhea of 2 weeks duration. A whole abdominal CT scan with IV contrast revealed heterogeneous soft tissue density adjacent to the terminal ileum and cecum, considering abscess formation. Intraluminal filling defects involving the extrahepatic portal vein and superior mesenteric vein relating to thrombus formation were also seen. Case 2 was a 57-year-old female, hypertensive who presented with sudden-onset, diffuse, abdominal pain associated with vomiting and fever for one day. There was elevation of amylase and lipase while abdominal CT scan with IV contrast revealed necrotizing pancreatitis with beginning walled-off pancreatic necrosis. An incidental finding of filling defects along proximal portal vein with non-opacification of the splenic vein, likely from thrombus was also noted. In both cases, porto-mesenteric duplex scan were also performed. Acute venous thrombosis in the (1) main portal and splenic veins and in the (2) portal and superior mesenteric veins were seen in the case of necrotizing pancreatitis and ileocecal abscess, respectively. Empirical antibiotics and anticoagulation on Enoxaparin were initiated for both cases. Both cases were discharged stable and advised to continue warfarin for home management of thrombosis.
Conclusions: Portal mesenteric venous thrombosis is often neglected as part of differential diagnosis in patients presenting with acute abdomen. This type of venous thromboembolism in atypical location is a rare complication of intra-abdominal infections and must be recognized. Anticoagulation to prevent propagation of thrombosis must be weighed carefully against bleeding risk.
Poster 75 Panels.
Poster Number: 76
Abstract Number: 1280366
The burden behind a birthmark: Klippel-Trenaunay syndrome in a 29-year-old with lymphedema and a history of lower extremity deep vein thrombosis
St. Luke’s Medical Center
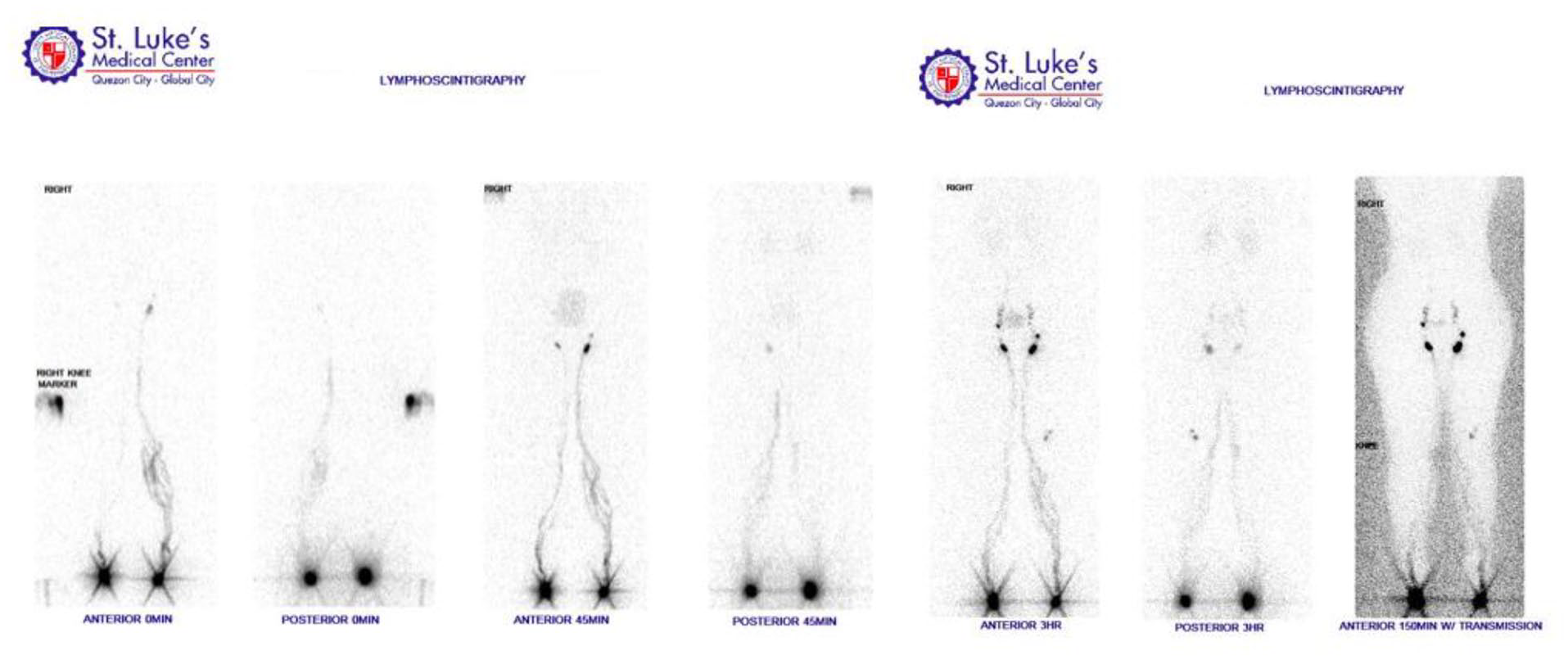
Background: Klippel-Trenaunay syndrome is a rare congenital disorder characterized by a limb affected with venous varicosities, limb hypertrophy and presence of capillary malformations or port-wine stains. Lymphedema is reported in 5% of these cases and syndromic patients who manifest lymphatic malformations have been identified to be associated with somatic mutations in the PIK3CA gene. Other clinical manifestations reported are superficial thrombophlebitis, deep venous thrombosis and gastrointestinal bleeding.
Case presentation: We present a 29-year-old case of Klippel-Trenaunay syndrome diagnosed in adulthood who presented with syndromic complications of deep venous thrombosis and subsequently lymphedema. She was initially seen at a clinic due to history of trauma from a vehicular-related accident developing asymmetric swelling of the right leg. A venous duplex scan done identified the presence of a subacute deep venous thrombosis partially occluding the right distal external iliac and common femoral veins. However, on physical exam and further history, she already had port wine stains on her right thigh and back area. The was also asymmetry of her lower limbs described as increasing girth of her right leg which was noticed by her family members during her late teenage years. After treatment with Rivaroxaban, repeat venous duplex scan showed resolution of deep venous thrombosis. However, there was still persistence of asymmetry and right leg swelling throughout the years. Lymphoscintigraphy was done showing slight asymmetric visualization of lymphatic vessels in the early images. A hypoplastic lymphatic tract in the right lower extremity is considered. Complete decongestive therapy was advised.
Conclusions: “Birthmarks” are skin irregularities visible at birth, often considered to be benign. However, it is important to identify that there are some that need medical attention. In a developing country such as the Philippines, proper education in recognition of these congenital syndromic conditions may aid in early assessment and management.
Poster 76 Panels.
Poster Number: 77
Abstract Number: 1273422
Finger ischemia attributed to oxymetazoline nasal spray
Alejandro Perez, MD, FSVM, RPVI
Providence Heart Institute
Background: Digital ischemia has previously been described with routine use of amphetamine and its related derivatives and arterial vasospasm has been documented with oral sympathomimetic for nasal decongestion.
Case presentation: 43-year-old woman presented with throbbing right thumb and second digit. This progressed to discoloration and pain worsened. Had been seen in the emergency department (ED) the prior 2 days. Patient did not recall any specific cold exposure and had not had trauma to hand. She is a non-smoker. Workup included digital testing showing abnormal arterial waveforms of the fingers on the right hand. Transthoracic echocardiogram demonstrated known bicuspid aortic valve without evidence of vegetations. CT chest angiography chest revealed no aortic dissection or periaortic inflammation. Patient had been prescribed nifedipine in the ED. Serology testing was normal for sedimentation rate, C-reactive protein, lupus (anti-nuclear antibody), rheumatoid factor, cyclic citrullin peptide antibody, lupus anticoagulant, beta-2 glycoprotein. Patient did have cardiolipin IgG elevation. Upon vascular medicine consultation patient revealed she has chronic nasal congestion and had used almost daily oxymetazoline nasal spray, an adrenergic agonist, for years. Outcome: Patient advised to stop all nasal decongestant therapy. In less than 3 weeks finger pain had resolved and had improvement of finger coloring.
Conclusions: Oxymetazoline nasal spray used for prolonged duration can cause digital ischemia.
Poster 77 Panel A and B.

Poster Number: 78
Abstract Number: 1273445
Interventional challenges in vasculitis
Parkview Medical Center
Background: This case highlights how coronary pathology presents in vasculitis.
Case presentation: A 49-year-old male, never-smoker presented to our hospital for a series of Acute Coronary Syndromes (ACS). The first in October 2019; angiogram revealed diffuse aneurysms and clot in the right coronary artery (RCA) and stenosis in the posterolateral branch (PLB). Post aspiration thrombectomy, and drug eluting stent (DES) to the PLB, patient was discharged on standard ACS meds. Coagulopathy workup was unremarkable. Follow up in November 2020, the patient was recommended reducing ticagrelor to 60mg twice daily (bid). The second ACS, one year later, revealed severe in-stent restenosis of the PLB stent. Patient had 2 DES placed in the PLB and was discharged on escalated therapy of rivaroxaban 2.5mg bid, and ticagrelor 90mg bid. Two months later the patient had COVID-19; during that admission he had two ACS events. The first showing mid-RCA stenosis and thrombosis of the same PLB; this was treated with only angioplasty. The next day, he had repeat ACS showing thrombosis of the RCA, but despite multiple attempts RCA recanalization was unsuccessful and discharged on medical therapy only. During clinic follow up, May 2022, the patient revealed that he had Kawasaki’s disease as a kid.
Conclusions: Coronary aneurysms are high risk because of slow flow and endothelial dysfunction that makes balloon dilation, stent sizing, and post interventional medical therapy difficult. Currently no standard guidelines exist to help providers treat this population. It may be beneficial to regularly follow up, monitor inflammatory markers (ESR, CRP correlated well with interleukin 6 and 8), and use CT or PET to follow active vasculitis and changes in aneurysms. Kawasaki’s disease is a vasculitis of small and medium-sized vessels and often presents in childhood. Prospective studies show that patients with coronary aneurysms tend to have systemic artery aneurysms, so it is important to screen other arterial beds. Valvular disease has also been found to co-exist in patients with vasculitis, and pre-existing disease should be followed with echocardiography.
Poster Number: 79
Abstract Number: 1277552
Aortoiliac chronic total occlusion (CTO) recanalization
Parkview Medical Center
Background: A 60-year-old female with a past medical history of supraventricular tachycardia (SVT), and bilateral DVT, atrial fibrillation on apixaban who reported lifestyle limiting claudication.
Case presentation: CT angiography of the abdomen and pelvis revealed chronic total occlusion (CTO) of the distal aorta and bilateral common iliac arteries. Patient was taken to the cath lab for intervention; ultrasound access was obtained in bilateral femoral arteries and left radial artery. With a pigtail positioned in the aorta, a glidewire was used for sub-intimal dissection from the proximal right common iliac artery to the infra-renal aorta. Pioneer IVUS-guided re-entry catheter was advanced over a miracle wire and needle puncture was performed to access the true lumen. These steps were repeated for the left common iliac artery. We then performed bilaterally simultaneous kissing balloon angioplasty of the infrarenal aorta and bilateral common iliac systems. Once aortoiliac recanalization was visualized, kissing VBX Balloon Expandable stents were deployed in bilateral common iliac arteries. The distal edge of the right external iliac artery stent showed a distal dissection, so a self-expanding Nitinol stent was deployed. Angiography showed excellent results and repeat pelvic arterial duplex 3 months after showed patent aortoiliac stents with no recurrent stenosis. She has been tolerating aspirin 81mg and apixaban 5mg bid for her atrial fibrillation well.
Conclusions: Furthermore, there is little published about successful revascularization in aortoiliac CTO. There has been growing success with stent-supported recanalization and this case illustrates how it can be a durable alternative to surgery in elderly patients or in patients with severe comorbidities. This case shows that percutaneous intervention should be considered prior to surgical bypass in such patients.
Poster Number: 80
Abstract Number: 1279536
Coronary arteriovenous fistula with peripheral arteriovenous malformation in a 20-year-old female: A serendipity or a mystery?
Zabrina Kay L. Rodriguez
HB Calleja Heart and Vascular Institute, St. Luke’s Medical Center Quezon City
Background: Arteriovenous malformations (AVM) are pathologic connections between arteries and veins. They may occur as an isolated lesion or in combination with other lesions, which may be part of a syndrome. Data on congenital peripheral AVM occurring concomitantly with a coronary arteriovenous fistula (CAVF) is limited.
Case presentation: A 20-year-old female presented with recurrent exertional chest pain not relieved with pain or anti-anginal medications, and easy fatigability of three years duration. Her previous medical history included recurrent AVM of the right leg despite percutaneous gel foam embolization six years ago. Her physical examination was unremarkable. Apart from a chest X-ray that showed cardiomegaly, preliminary work-up was essentially normal (Troponin, 12-L ECG, 24-hour Holter monitor, 2D Echocardiogram, Stress Echocardiography, Myocardial Perfusion Imaging). CT coronary angiography (CTA) showed a CAVF of the left circumflex artery and great cardiac vein. The patient is now referred to thoracic cardiovascular surgery service for surgical intervention.
Conclusions: We highlight the importance of increased clinical suspicion for CAVF for young patients with persistent chest pain, especially in the setting of previous congenital lesions. Further investigation is needed to determine whether an anomalous arteriovenous connection at one site predisposes an individual to having an arteriovenous connection at another. This is an underreported phenomenon that could be a part of a rare syndromic condition.
Poster Number: 81
Abstract Number: 1280495
A rare case of high take-off radial artery pseudoaneurysm after percutaneous coronary intervention-drug eluting stent (PCI-DES)
St. Luke’s Medical Center
Background: High take-off radial artery is a rare anatomic variant with no distinct predisposition and gender peculiarity. Radial artery (RA) anatomic variants can be seen in ~30% of individuals and published autopsy studies report its occurrence in ~15%. It is rare at 0.66% during PCI. RA puncture is the preferred access for most cardiovascular procedures. The tortuosity and flow dynamics related to anatomic variants may lead to procedural complications such as dissection, ischemia, aneurysm, and thrombosis.
Case presentation: This is a case of a 57-year-old, hypertensive, non-diabetic male, who underwent emergency PCI-DES via the right radial artery due to an ST segment elevation myocardial infarction. Two hours post-procedure, he had sudden right forearm pain and swelling with an 8x10cm hematoma formation. Arterial duplex of the upper arm revealed pseudoaneursyms. He underwent ultrasound-guided pseudo-aneurysm compression therapy. CT angiography of the upper extremity showed a high division of the right brachial artery dividing into the radial and ulnar arteries at the level of the proximal humeral shaft. He was discharged improved with direct-acting oral anticoagulation (DOAC).
Conclusions: This is a rare case of a high take-off radial artery pseudo-aneurysm. The pre-procedural duplex ultrasound evaluation of the upper extremity may help in detecting clinically significant anatomic variations so as to prevent future complications.
Poster 81 Panel.

Poster Number: 82
Abstract Number: 1268826
Rivaroxaban treatment failure during COVID-19 infection
Patrick Sullivan, MD, John Fish, MD, FSVM
Jobst Vascular Institute
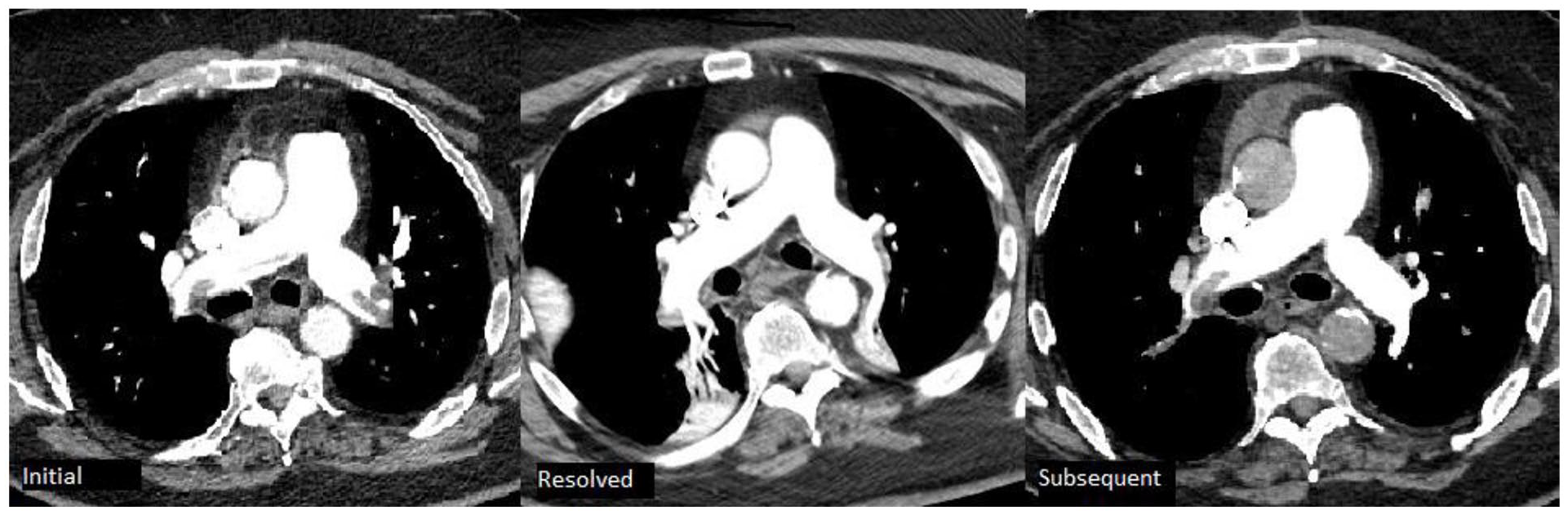
Background: The Coronavirus Disease 2019 (COVID-19) has been shown to Increase incidence of venous thromboembolism (VTE). We describe a novel case of rivaroxaban treatment failure in a patient with COVID-19 infection who previously demonstrated efficacious treatment of prior pulmonary embolism (PE) with rivaroxaban
Case presentation: A 75-year-old male patient originally presented for syncope and was found to have acute submissive PE on Computed tomography angiogram of his (CTA) chest. He was placed on heparin initially and he remained hemodynamically stable during his admission and was discharged home on rivaroxaban at standard induction dose. He presented again for shortness of breath 3 months later. CTA chest was repeated and demonstrated resolution of his prior PE. He was found to be positive for COVID-19 and admitted for further management, rivaroxaban was continued during his admission. Repeat CTA of his chest 2 weeks later demonstrated moderate right and small left PE without right heart strain. Vascular Medicine was consulted at that time. The patient reported taking his rivaroxaban as directed throughout the recommended course. He reported taking rivaroxaban with food. He said his son helped him with his medications and it was unlikely he missed any doses. He was able to get his medications from the Veterans Health Administration (VA) and had no issues with access to medications. Medication review revealed no drug interactions that would decrease efficacy of rivaroxaban. The patient’s weight of 116 kg was within the acceptable range for rivaroxaban use.
Conclusions: This case is unique in that timing of CTA scans demonstrated complete resolution of patient’s initial PE while taking rivaroxaban followed by new development of PE after COVID-19 infection despite continuation of rivaroxaban therapy.
Poster 82 Panels.
Poster Number: 83
Abstract Number: 1270834
Rampant misadventures: Coronary artery involvement in large vessel vasculitis
Alexander E. Sullivan, MD, Tara Holder, MD, Jacob Grand, MD, Thomas McLaren, MD, Aaron Aday, MD, S. Esther Kim, MD
Vanderbilt University Medical Center
Background: A 54-year-old man with known idiopathic aortitis presented with angina. He had abdominal pain 6 years prior with MRI showing aortitis extending from the celiac to left renal artery (Panel A). He received prednisone but was taken off immunosuppression after two years without recurrence or progression on serial imaging.
Case presentation: Three years later, he was found to have a left subclavian bruit. CTA demonstrated left subclavian and ostial vertebral lesions with enlarging aortic ectasia. Left upper extremity arterial duplex showed severe proximal left subclavian stenosis (Panel B). Renal duplex ultrasound showed 70-99% stenosis. ESR and CRP were normal, raising concern that lesions were chronic from prior vasculitic damage. Two months later, he developed angina and coronary angiography revealed a long, smooth 99% stenosis in the proximal LAD (Panel C). CMR demonstrated viable myocardium and patchy LGE throughout the aorta consistent with inflammation. He underwent bypass surgery with a free LIMA-LAD and SVG-OM1. At follow-up, he had no angina or evidence of disease progression on maintenance mycophenolate.
Conclusions: Coronary arteritis is a rare complication of systemic large vessel vasculitis, but typically portends a poor prognosis. The optimal timing and modality of revascularization is unknown and challenging in the setting of concomitant aortitis and left subclavian arteritis. In this case, we present a patient with multi-bed arteritis who underwent successful surgical revascularization of severe LAD disease.
Poster 83 Panels A-C.

Poster Number: 84
Abstract: 1280065
Venous stenting and sulodexide in case of metastatic cancer, extensive lower extremity acute venous thrombosis, and bleeding
St. Luke’s Medical Center
Background: Deep venous thrombosis is a common complication of malignancy. Prevention and timely treatment with an anticoagulant are critical in the management of these cases. However, bleeding may preclude appropriate treatment and alternative approach are often considered. Sulodexide, a purified glycosaminoglycan containing 80% heparan sulfate and 20% dermatan sulfate. It can be used to prevent recurrent venous thromboembolism after standard anticoagulation is discontinued. Endovascular venous stenting is also a useful technique to restore the venous flow and palliate the symptomatic patients with extrinsic compression.
Case presentation: This is a case of a 63-year-old Asian female with ovarian cancer stage IV with extensive deep venous thrombosis presenting with excessive vaginal bleeding and a two-month history of progressive unilateral leg swelling and tenderness. IVC filter insertion was done and was given sulodexide 600 LSU IV twice daily. However, her symptoms persisted and further work-up showed multiple enlarged and confluent mesenteric, pelvic and inguinal lymph nodes causing extrinsic compression of the right proximal to mid external iliac vein. Right femoral vein thromboembolectomy and right common iliac vein stenting was done to relieve the obstruction.
Conclusions: Managing complicated cases require careful consideration of suitable intervention/s. Every treatment should be individualized and it is imperative to do a risk to benefit analysis.
Poster 84 Panel.
Poster Number: 85
Abstract Number: 1271659
Poster Number: 86
Abstract Number: 1272774
Poster Number: 87
Abstract Number: 1273834
Stanford type A and Debakey type I extensive aortic dissection masquerading as atypical angina
Prima H. Wulandari
Harvard Medical School-Massachusetts General Hospital
Background: Aortic dissection is one of the acute emergency cases with high mortality. Despite high mortality imposed on this diagnosis, not all of the patients show the most common symptoms, such as sudden tearing pain in the chest. This case demonstrates the possibility of aortic dissection presented as atypical angina.
Case presentation: A 37-year-old obese male with uncontrolled hypertension history, complained of chest discomfort since 2 days prior that radiated to the back, with associated symptoms of sore back muscle and sweating. Complaints of epigastric pain and burping were also reported. Blood pressure was 170/110 mmHg, while physical examination revealed diastolic murmur grade II-IV on the intercostal space II. ECG showed sinus rhythm, normoaxis, left ventricular hypertrophy, T inverted in lead III and aVF. Initial laboratory results showed low platelet count, high CRP, high LDL, however normal serial CKMB and Troponin T hs. From echocardiography, there was left ventricular concentric hypertrophy, grade I diastolic dysfunction, mild AR, and dilatation of ascending aorta, global normokinetic with LVEF 64%. MSCT cardiac (triple rule out) was done and intramuscular bridging at mid LAD along with aortic dissection were found. Calcium scoring Agatston score was negative. Subsequent CTA thoraco-abdominal aorta showed extensive aortic dissection (Stanford type A, De Bakey type I) from the sinotubular junction through the ascending aorta, aortic arch, descending aorta, abdominal aorta, and to the right common iliac artery (+- 6 cm from bifurcation). The patient then underwent Bentall procedure and total arch replacement at tertiary hospital. After the procedure, he is currently doing phase II cardiac rehabilitation and he is being prepared to return to work.
Conclusions: This case describes an important role of clinical reasoning and comprehensive examinations in evaluating patients with atypical angina, in order not to miss the possibility of aortic dissection.
Poster 87 Panels.