
Abstract

Jay D. Coffman Young Investigator Award Presentations
In honor of Dr. Jay D. Coffman (1928–2006), distinguished internist and researcher of vascular medicine and clinical cardiology, founder and past President of the Society for Vascular Medicine (SVM), SVM sponsors an annual award in vascular medicine and biology research.
Poster Number: 01
Abstract Number: 1271409
Association of HIV infection with clinical features and outcomes of patients with aortic aneurysms
1Johns Hopkins University Hospital, 2Mayo Clinic Rochester, 3Wayne State University / Detroit Medical Center, 4National Heart Lung and Blood Institute
Background: Growing evidence suggests an association between human immunodeficiency virus (HIV) infection and higher rates of aortic aneurysms (AA), but data on the characteristics and outcomes of hospitalized patients with AA and HIV remain scarce
Methods: This is a cohort study of hospitalized adult patients with a diagnosis of AA from 2013 to 2019 using the US National Inpatient Readmission Database. Patients with a diagnosis of HIV were identified. Our outcomes included trends in hospitalizations and comparison of clinical characteristics, complications (i.e., aortic rupture and dissection) and mortality in patients with AA and HIV compared to those without HIV.
Results: There was an overall age-adjusted increasing prevalence of HIV among patients hospitalized with AA over the years (14 to 29 per 10,000 person-year; age-adjusted p-trend < 0.001) Figure). On univariate analysis, patients with AA and HIV were younger than those without HIV (median age: 60 vs 76 years, p < 0.001), and were less likely to have a history of smoking, hypertension, dyslipidemia, diabetes mellitus and obesity (Table). Thoracic aortic aneurysms were more prevalent in those with HIV (37.5% vs 26.7%, p< 0.001). On multivariable logistic regression, HIV was not associated with increased risk of aortic rupture (OR: 0.79 (0.61- 1.01), p=0.06), acute aortic dissection (OR: 0.73 (0.51-1.06), p=0.3), readmissions (OR:1.04, 95% CI: 0.95-1.13; p=0.4), or with increased rates of aortic repair (OR: 0.89 (0.79-1.00; p=0.05). Patients hospitalized with HIV and AA had a lower crude mortality rate compared to patients hospitalized with AA without HIV (OR:0.75 (0.63-0.91); p=0.004).
Conclusion: Hospitalized patients with AA and HIV likely constitute a distinct group of patients with AA; they are younger, have fewer traditional cardiovascular risk factors, and a higher rate of thoracic aorta involvement. Differences in clinical features may account for the lower mortality rate observed in patients with AA and HIV compared to those without HIV. Further prospective longitudinal studies are warranted to investigate the pathophysiology of AA in patients with HIV and address its impact on long term outcomes.

Baseline characteristics of patients admitted with aortic aneurysm (aa), stratified by presence or absence of HIV.
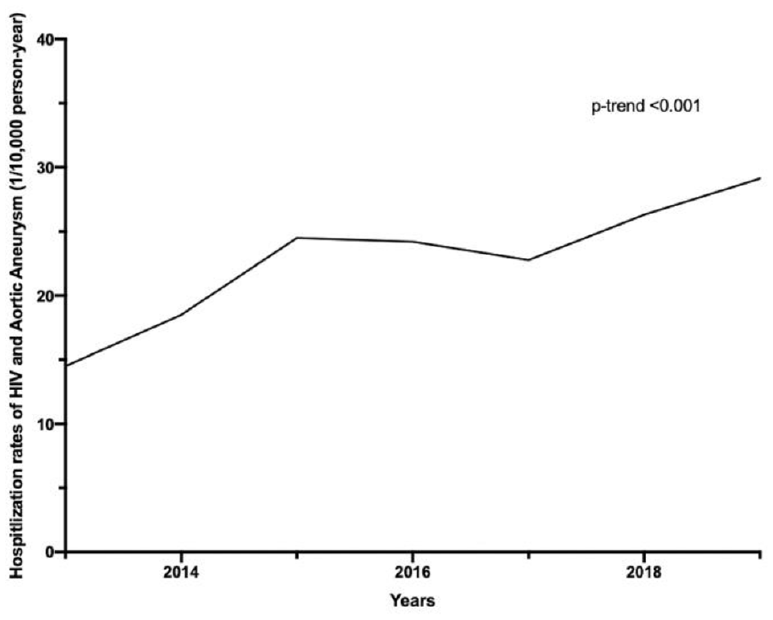
Temporal trend for hospitalizations of people living with HIV and aortic aneurysm.
Poster Number: 02
Abstract Number: 1273664
Characteristics of non-response to exercise therapy in people with peripheral artery disease: results from five randomized clinical trials
1University of Illinois at Chicago, 2Northwestern University, 3Stanford University
Background: Walking exercise is the first line therapy for lower extremity peripheral artery disease (PAD). Data from five randomized trials were combined to measure the effects of exercise, compared to control, on the presence of ischemic leg symptoms and stopping during the six-minute walk test (6MW) after exercise interventions. Characteristics associated with a poorer response to exercise in PAD were also identified.
Methods: Data were combined from five randomized trials of supervised or home-based exercise in PAD. At trial completion, proportions of people with exertional leg symptoms and rates of stopping during the 6MW were compared between the exercise and control groups.
Results: 707 people with PAD (46% women, 60% Black) were included. Exercise improved 6MW compared to control (mean difference: +35.49 meters (95% CI: 26.39-44.60). Compared to control, exercise reduced rates of stopping during the 6MW (25% vs 37%, p=0.002) but had no effect on exertional leg symptoms (82% exercise vs. 85% control, P= 0.24). Characteristics associated with 6MW stopping and leg symptoms at trial completion are in the Table.
Conclusion: Even after effective exercise interventions, most people with PAD reported leg symptoms with walking and 25% stopped during 6MW. Cigarette smoking and high BMI were modifiable risk factors associated with persistent leg symptoms and stopping during the 6MW, respectively, after exercise interventions.

Characteristics of persistent exertional leg symptoms and stopping during the 6MW at trial completion among those randomized to the exercise intervention.
Poster Number: 03
Abstract Number: 1273848
Coronavirus but not influenza virus infection induces the expression of both cellular and soluble urokinase plasminogen activator receptor
1University of Michigan; Jobst Vascular Laboratory, 2University of Michigan
Background: Urokinase plasminogen activator receptor (uPAR/PLAUR) is a cell surface receptor on monocytes and macrophages (MO/Mφs), which when cleaved, forms soluble uPAR (suPAR). Previous work has shown that uPAR is differentially induced in MO/Mφs after coronavirus (CoV) infection and contributes to hyperfibrinolysis. In contrast to cellular uPAR’s fibrinolytic function (implicated in CoV-induced coagulopathy), suPAR is a Mφ chemotactic factor implicated in perpetuating tissue injury after CoV infection. However, it is unclear if induced levels of cellular uPAR correlate with the elevated levels of suPAR after CoV infection and how suPAR expression is regulated after influenza virus (IAV) infection.
Methods: Published scRNA sequencing data (GSE149689) of PBMCs from patients (COVID-positive and IAV-positive) and healthy controls was analyzed. In vitro, we performed infections of immortalized murine Mφs (RAW264.7) with the CoVs MHVA59 or MHV1, or the IAV (A/PR/8/34; H1N1) at the indicated MOI for 24 hours. uPAR and urokinase levels were measured by ELISA. Urokinase activity of conditioned media was measured using a commercially available colorimetric assay.
Results: scRNA analysis revealed differential expression of PLAUR in MOs from COVID and IAV-positive relative to healthy controls, with the highest PLAUR expression in COVID-positive samples (Fig. A-B). Infection of RAW264.7 cells with CoV and IAV induced cellular uPAR expression, but only CoV infection induced suPAR expression (Fig. C). In contrast to uPAR, the expression of both cellular and soluble urokinase levels was induced after infection with either CoVs or IAV (Fig. D). Finally, induction of urokinase activity of conditioned media after viral stimulation was observed after infection with either CoVs or IAV (Fig. E).
Conclusion: CoV but not IAV infection induces the expression of both cellular and soluble uPAR in MO/Mφs. Both CoV and IAV induce the expression of cellular and soluble urokinase, and urokinase activity. Understanding this virus specific effect on uPAR/suPAR in innate immune cells may reveal the pathogenesis of virus-associated coagulopathy and tissue injury.

Results of scRNA analysis.
Poster Number: 04
Abstract Number 1269737
Effects of ischemic leg symptom-inducing exercise on simultaneous improvement in patient reported outcomes and six-minute walk distance in peripheral artery disease: the LITE randomized clinical trial
1University of Minnesota, 2Northwestern University, 3University of Maryland, 4University of Pittsburgh, 5University of Florida
Background: An optimal exercise program for peripheral artery disease (PAD) would improve both objective measures and patient reported outcomes (PROs). This post-hoc analysis of the LITE trial assessed whether walking exercise conducted at a pace inducing ischemic leg symptoms (high intensity) was more likely to improve both PROs and six-minute walk distance (6MW), compared to walking at a pace without ischemic leg symptoms (low intensity) and a non-exercise control group (control).
Methods: The LITE trial randomized 305 people with PAD to home-based exercise at a high intensity pace, low intensity pace, or control for 12 months. PROs were the Walking Impairment Questionnaire (WIQ) and the Short Form-36 (SF-36) physical function score. Participants were categorized according to whether they had any improvement in 6MW and each PRO at 12-month follow-up.
Results: Of 305 randomized, 242 people completed the 6MW and at least one PRO at baseline and follow-up (61% Black; 48% women). High intensity exercise was significantly more likely to improve both 6MW and each PRO, compared to the other groups (Table).
Conclusion: To improve both objective walking measures and PROs, patients with PAD should walk for exercise at a pace inducing ischemic leg symptoms, not at a pace without ischemic leg symptoms.

Chi-square tests comparing low intensity, high intensity, and control groups based on response to 6MW and each PRO (WIQ distance, speed, stair-climbing, and SF-36 physical function).
Poster Number: 05
Abstract Number: 1271503
Impact of cancer on outcome among hospitalized patients with venous thromboembolism: data from national inpatient sample
1Reading Hospital, 2Thomas Jefferson University Hospital
Background: Venous thromboembolism (VTE) is a leading cause of morbidity and mortality in hospitalized patients. Little is known about the impact of a cancer diagnosis on inpatients with VTE. We aim to find out the association of venous thromboembolism with the most common malignancies and compare the impact of VTE on mortality in patients with and without a cancer diagnosis.
Methods: We used the US National Inpatient Sample (NIS) database from the years 2016 to 2019 as our sample population. We used ICD-10 classification to identify patients with diagnoses of venous thromboembolism and malignancies. We used STATA version 13.0 (College Station, TX) to perform multivariable logistic regression analyses and Microsoft Excel for data representation.
Results: The final study population was based on 475,356 (weighted count = 2,376,779) inpatient hospital discharge records. The overall odds ratio of mortality in patients with compared to those without malignancy was 2.33 (2.26 – 2.41, p < 0.001). Lung cancer (2.6), pancreatic cancer (2.4), ovarian cancer (1.85), Hodgkin’s lymphoma (1.69), brain cancer (1.67), leukemia (1.26), renal and pelvis (1.2), colorectal cancer (1.18), and uterine cancer (1.16) were significantly associated with increased risk of VTE.
Conclusion: The risk of mortality with VTE in cancer patients varies with the type of malignancy. Awareness of the increased risk of VTE with different cancers and appropriate and aggressive pharmacologic and mechanical prophylaxis may be needed to improve outcomes in this subpopulation.

Forest plot comparing the odds ratio of mortality in venous thromboembolism with and without a cancer diagnosis.
Poster Number: 06
Abstract Number: 1273599
Increase in soluble cell adhesion molecules early after spinal cord injury
1Craig Hospital, 2University of Colorado
Background: Adults with spinal cord injury (SCI) not only sustain significant neurological challenges, but suffer from an accelerated form of cardiovascular disease (CVD). In fact, atherosclerotic vascular disease has been demonstrated in adults aging with SCI up to a decade earlier than in the general population, and myocardial infarction and cerebrovascular accidents are the leading cause of mortality and morbidity after the first year of SCI. In spite of initial clinical assumption, the increased rate atherosclerosis in adults with SCI is not primarily due to traditional risk factors. Driven by injury characteristics and ill-defined mechanisms, identifying early targets to prevent vascular disease after SCI is critically important. Increased expression of cell adhesion molecules is an early development in the pathogenesis of atherosclerosis. Soluble intracellular and vascular cell adhesion molecules (sICAM-1/sVCAM-1) are etiologically linked with atherosclerosis and have been demonstrated to be elevated in adults with chronic (>1 year) SCI. Whether cell adhesion molecules are elevated early after SCI is unknown. We tested the hypothesis that sICAM-1 and sVCAM-1 levels are elevated early after SCI.
Methods: Circulating sICAM-1 and sVCAM-1 concentrations were assessed in 16 uninjured adults (13 M/3 F; age: 35±3yr) and 16 adults with traumatic subacute (4-12 weeks) tetraplegic injuries (13 M/3 F; age: 33±3yr). None of the participants had a history of CVD or metabolic disease and were free of active infections.
Results: sICAM-1 (297±48 vs 226±102 ng/mL) and sVCAM-1 (716±259 vs 538±176 ng/mL) were significantly higher (~30%) in adults with subacute SCI compared with non-injured adults.
Conclusion: Cell adhesion molecules are elevated early after spinal cord injury. Elevations in sICAM-1 and sVCAM-1 suggest that subclinical vascular changes may be occurring much earlier after SCI than previously speculated. Further prospective work is needed to determine if sICAM-1 and sVCAM-1 is an early marker of accelerated atherosclerosis after SCI.
Poster Number: 07
Abstract Number: 1279002
High ankle brachial pressure index is associated with all-cause mortality
1Massachusetts General Hospital, Harvard Medical School, 2Lewis Katz School of Medicine at Temple University, 3Weil Cornell Medicine-Qatar
Background: A reduced ankle brachial index (ABI) correlates with adverse cardiovascular outcomes. In contrast, the association of high ABI (>1.4) is unclear. We studied the association of high ABI and all-cause mortality in the National Health and Nutrition Examination Survey (NHANES) and compared it with that of low and normal ABI.
Methods: We obtained ABI from participants age>40 years for survey years 1999 to 2004. We defined low ABI < 0.9, normal ABI 0.9-1.4, and high ABI was >1.4 or if the ankle pressures were >245 mmHg. All-cause mortality was linked to all NHANES participants for follow-up through December 31, 2019 from Centers for Disease Control and Prevention. Odds ratios (OR) were calculated from multivariable logistic regression.
Results: We identified 7639 NHANES participants with available ABI. Of these, 6787 (89%) had normal ABI, 646 (8%) had low ABI, and 206 (3%) had elevated ABI. Of participants with high ABI, 69% were men, 10% were smokers, 56% had hypertension, 67% had diabetes, 62% had hyperlipidemia, and 18% had concomitant coronary artery disease (CAD). Cumulative all-cause mortality was 33% for participants with elevated ABI, 37% for low ABI and 18% for normal ABI. High ABI was independently associated with elevated all-cause mortality (OR= 2.05, p < 0.0001) after adjusting for co-variates including CAD, current smoking, statin therapy, and eGFR< 30 (Figure).
Conclusion: A high ABI is associated with an elevated all-cause mortality, similar to low ABI, compared to normal ABI. Future research may assess benefits of cardiovascular secondary prevention measures in this group.

Adjusted odds ratios with 95% confidence intervals for cumulative all-cause mortality in NHANES participants.
Poster Number: 08
Abstract Number: 1278483
Determining the accuracy of pedal acceleration time in the diagnosis of significant peripheral artery disease using ankle-brachial index as a gold standard: a prospective validation study
St. Luke’s Medical Center Quezon City
Background: Peripheral artery disease (PAD) is a global burden that serve as a window to several cardiovascular diseases. Early recognition is key to prompt management of these patients. The ankle-brachial index (ABI) is a non-invasive way to determine the presence of significant lower extremity artery disease. However, it has certain limitations. These include the inability to tolerate ankle cuff pressures, presence of ulcers on the ankle area and challenges in interpreting incompressible values. There is a need for other diagnostic modalities that are tolerable for the patient and reproducible for technicians in diagnosing PAD. Pedal acceleration time (PAT) is a relatively new diagnostic procedure that insonates the pedal vessels of the lower extremities to determine the presence of lower extremity artery disease. PAT is a novel test that may be used as a substitute for ABI in classifying patients with PAD. It is a measure of tissue perfusion to the extremity. It is acquired by insonating the pedal arteries and taking their acceleration time (time from initial to peak blood flow) using Doppler studies.
Methods: This was a prospective validation study of patients who had their ABI and arterial duplex done in a tertiary hospital from July to November 2021.
Results: 104 subjects were included in this study. Out of the 104, 10 patients had discordant ABI and PATs for each of the extremities. The right lower extremity showed moderate agreement of the ABI with PAT (Kappa = 0.508). The left lower extremity also showed a fair agreement of the ABI with PAT (Kappa = 0.468). Most of the subjects had limbs falling under Categories 1 to 3 of the PAT Classification system.
Conclusion: There is a moderate agreement between ABI and PAT. Hence, PAT may be a surrogate diagnostic in diagnosing and classifying patients with PAD. However, further investigation on the relationship of ABI and PAT for patients falling under Category 4 may be explored in future research.

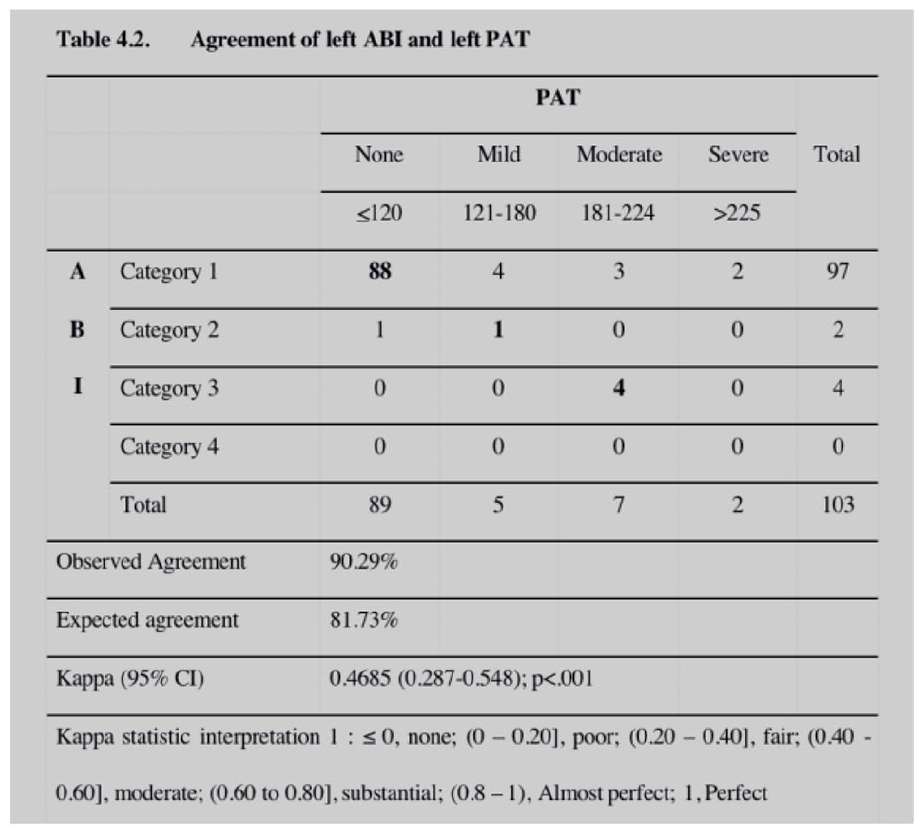
Agreement between ABI and PAT of the right (Table 4.1) and left (Table 4.2) lower extremities.
Poster Number: 09
Abstract Number: 1279484
Dietary patterns and young adult body mass change: A 9-year longitudinal study
1The University of Queensland, Australia, 2Princess Alexandra Hospital, 3University of Saskatchewan
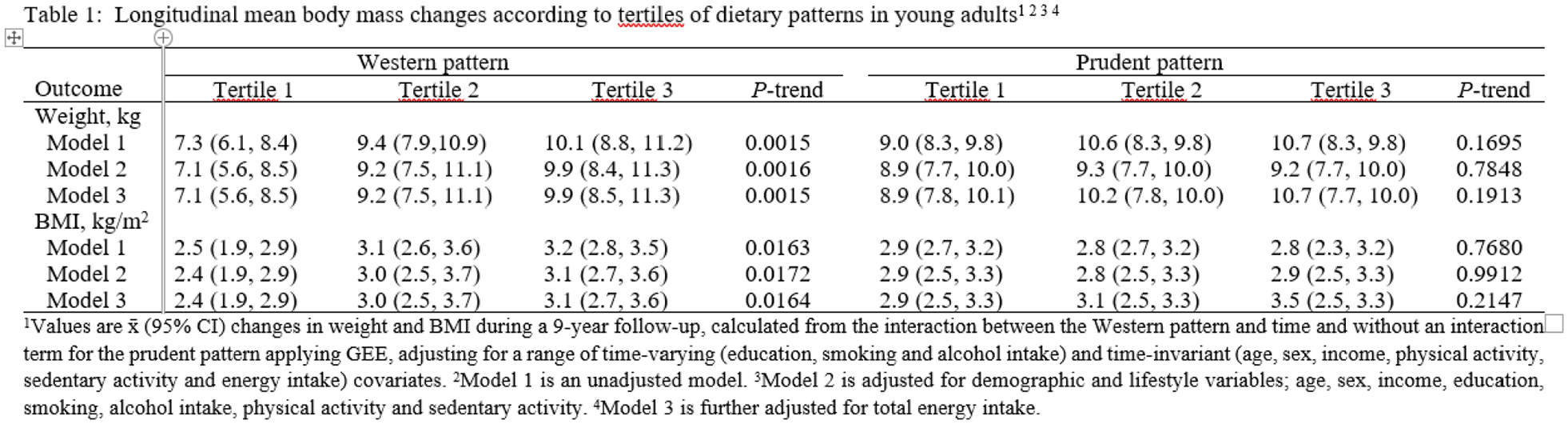
Background: We aimed to examine the associations of dietary patterns at 21-years with changes in body weight and body mass index (BMI) between 21- and 30-years
Methods: Western and prudent dietary patterns were identified applying principal component analysis to 33 food groups obtained by a food frequency questionnaire at 21-years using data from Australian birth cohort. Weight and height were measured at 21- and 30-years. We used generalized estimating equations to adjusted for concurrent changes in sociodemographic and lifestyle variables in evaluating the effects of dietary patterns on weight and BMI over time.
Results: In fully adjusted model, participants in the highest tertile of the Western pattern had a mean weigh gain of 9.9 (95% CI: 8.5, 11.3) kg compared to those in the lowest that had a mean weight gain of 7.1 (95% CI: 5.6, 8.5). The corresponding values for mean gains in BMI were 3.1 (95% CI: 2.7, 3.6) kg/m2 for young adults in the highest tertile compared to 2.4 (95% CI: 1.9, 2.9) for those in lowest. There was no evidence of significant association between the prudent pattern and mean changes in each outcome over time in this study.
Conclusion: The findings show that greater adherence to the Western diet over time increased weight, whereas the prudent diet had no significant affect. The adverse effects of the Western diet on weight gain in could partly be prevented through optimizing diet in early life.
Poster Number: 10
Abstract Number: 1279490
Dietary patterns and young adult risk of abnormal blood lipids: is there prospective associations?
1The University of Queensland, Australia, 2Princess Alexandra Hospital, 3University of Saskatchewan
Background: The extent to which dietary patterns influence the risk of abnormal blood lipids throughout young adulthood remains unclear. We aimed to investigate whether early young adulthood dietary patterns predict the risk of abnormal blood lipids during later young adulthood.
Methods: We used data from a long running birth cohort study in Australia. We derived dietary patterns using principal component analysis at the 21-year follow-up. After 9-years, fasting blood samples of participants were collected and their total, low-density lipoprotein (LDL) and high-density lipoprotein (HDL) cholesterols and triglyceride (TG) levels were measured. Abnormal blood lipids were based on clinical cut-offs for total, LDL and HDL cholesterols, and TG and relative distributions for total:HDL and TG:HDL cholesterols ratios. Log-binomial models were used to estimate risk of each outcome in relation to dietary patterns.
Results: Greater adherence to the Western pattern predicted increased risks of high LDL (RR: 1.47; 95%CI: 1.06, 2.03) and TG (1.90; 1.25, 2.86), and high ratios of total:HDL (1.48; 1.00, 2.19) and TG:HDL (1.78; 1.18, 2.70) cholesterols in fully adjusted models. Conversely, a prudent pattern predicted reduced risks of low HDL (0.58; 0.42, 0.78) and high TG (0.66; 0.47, 0.92) and high total:HDL (0.71; 0.51, 0.98) and TG:HDL (0.61; 0.45, 0.84) cholesterols ratios.
Conclusion: In conclusion. this is the first prospective study to show greater adherence to unhealthy Western diet predicted increased risks of abnormal blood lipids, whereas healthy prudent diet predicted lower such risks in young adults. Addressing diets in early course may improve cardiovascular health of young adults.
Poster Number: 11
Abstract Number: 1273501
Major bleeding, recurrence and mortality in chronically immobilized patients treated for venous thromboembolism
1Prisma Health - University of South Carolina School of Medicine, 2Massachusetts General Hospital, Harvard Medical School, 3Weil Cornell Medicine-Qatar, 4Parc Sanitari Sant Joan de Déu-Hospital General, 5University Hospital Hradec Kralove, 6Hospital Universitari de Girona Dr. Josep Trueta, 7Hospital Clínico San Carlos, 8Hospital General Universitario de Alicante, ISABIAL, UMH, 9Facultad de Medicina, Universidad Autónoma, Hospital Universitari Germans Trias i Pujol
Background: Immobility is highly prevalent and a well-defined risk factor for VTE. However, little is known about treatment patterns and outcomes of patients who are chronically (>8 weeks) immobile.
Methods: Chronically immobile patients from the Registro Informatizado Enfermedad TromboEmbolica (RIETE) who were diagnosed with VTE were included. For the purposes of the current abstract, treatment and outcomes including recurrent VTE and major bleeds were compared among patients presenting with PE or DVT.
Results: Of 4,612 chronically immobile patients (age 75.7±14.7, 34% male), 2,127 (46%) presented with PE. During the first 90 days of anticoagulation, recurrent VTE occurred in 1.3% of patients, while major bleeding occurred in 3.4% (Figure, Panel A). Intracranial bleeding occurred in 0.56%. Approximately two-thirds of recurrent VTE events were PE. After discontinuation of anticoagulation, recurrent VTE occurred in 8.2% of patients, while major bleeding in 0.88% (Figure 1, Panel B). During this period, death from recurrent PE occurred in 0.15% while death from major bleeding occurred in 0.59% of patients. Of note, 77% of patients received anticoagulation beyond 90-days. In multivariable analysis, major bleeding when anticoagulation was extended beyond 90-days was associated with anemia [odds ratio [OR] 1.73 (1.04-2.87)]. After stopping anticoagulation, VTE recurrence was inversely associated with long-term facility residence [OR 0.51 (0.28-0.92)], anemia [OR 0.63 (0.42-0.95)] and anticoagulation duration < 90 days [OR 0.38 (0.27-0.54)].
Conclusion: Chronically immobile patients presenting with VTE experience a high rate of adverse events including major bleeding and recurrent VTE. Treatment duration must balance between bleeding and recurrence risk, and associated mortality.
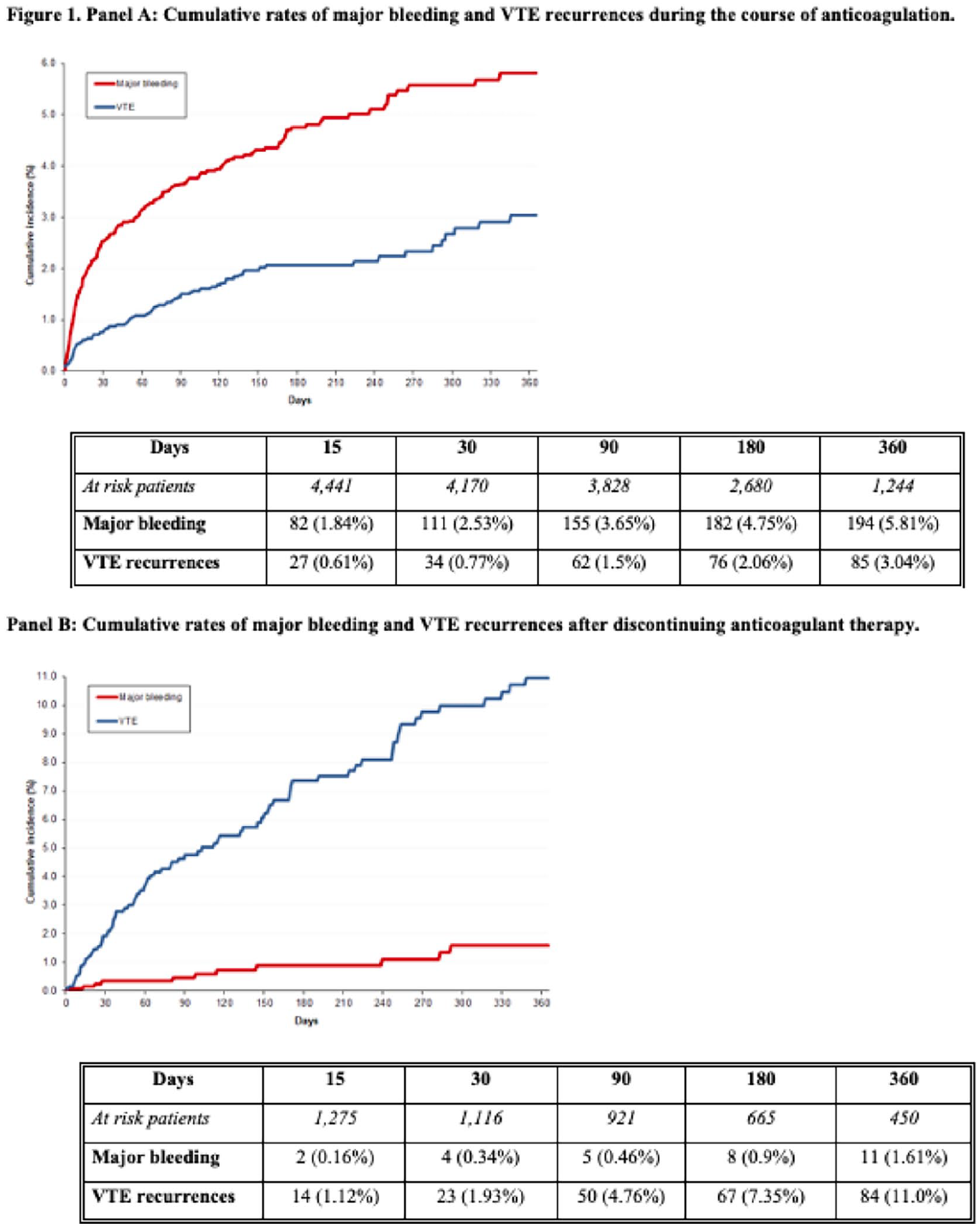
Cumulative rates of major bleeding and VTE recurrences.
Poster Number: 12
Abstract Number: 1278251
Living in food deserts and major adverse limb events in patients with peripheral artery disease
Saint Luke’s Mid America Heart Institute
Background: Major adverse limb events (MALE) represent an important clinical outcome for patients with PAD and disproportionally impact minority populations. As a marker of community health, living in a food desert (FD) may account for these differences.
Methods: Patients with PAD from a single-system registry were geocoded as living in a FD vs non-FD according to the USDA Food Access Research Atlas. FDs are census tracts defined by low income and poor food access (defined as proximity to a grocery store). The primary composite endpoint of MALE was defined as acute limb ischemia, major amputation, and limb revascularization. Cox regression models were used to examine the association of area characteristics (FD, poor access, low income) and MALE adjusted for traditional factors.
Results: From 2015 to 2021, 1,834 (15.4%) of 11,907 lived in FDs. Patients in FDs were more likely Black or Hispanic, residing in urban areas, had low vehicle access, and had a higher prevalence of hypertension, diabetes, and chronic kidney disease. Whereas the adjusted risk of MALE among those in FDs vs non-FDs was not different (hazard ratio 0.99 [95% CI, 0.83-1.19], p=0.952), those living in poor food access areas were associated with a higher adjusted risk of major amputation (HR 1.55 [1.07-2.23], p=0.019).
Conclusion: Poor food access may account for differences in amputation risk among minority populations. This may serve as an important target for advocacy and health policy. Future prospective studies should examine the impact of interventions that mitigate poor food access.
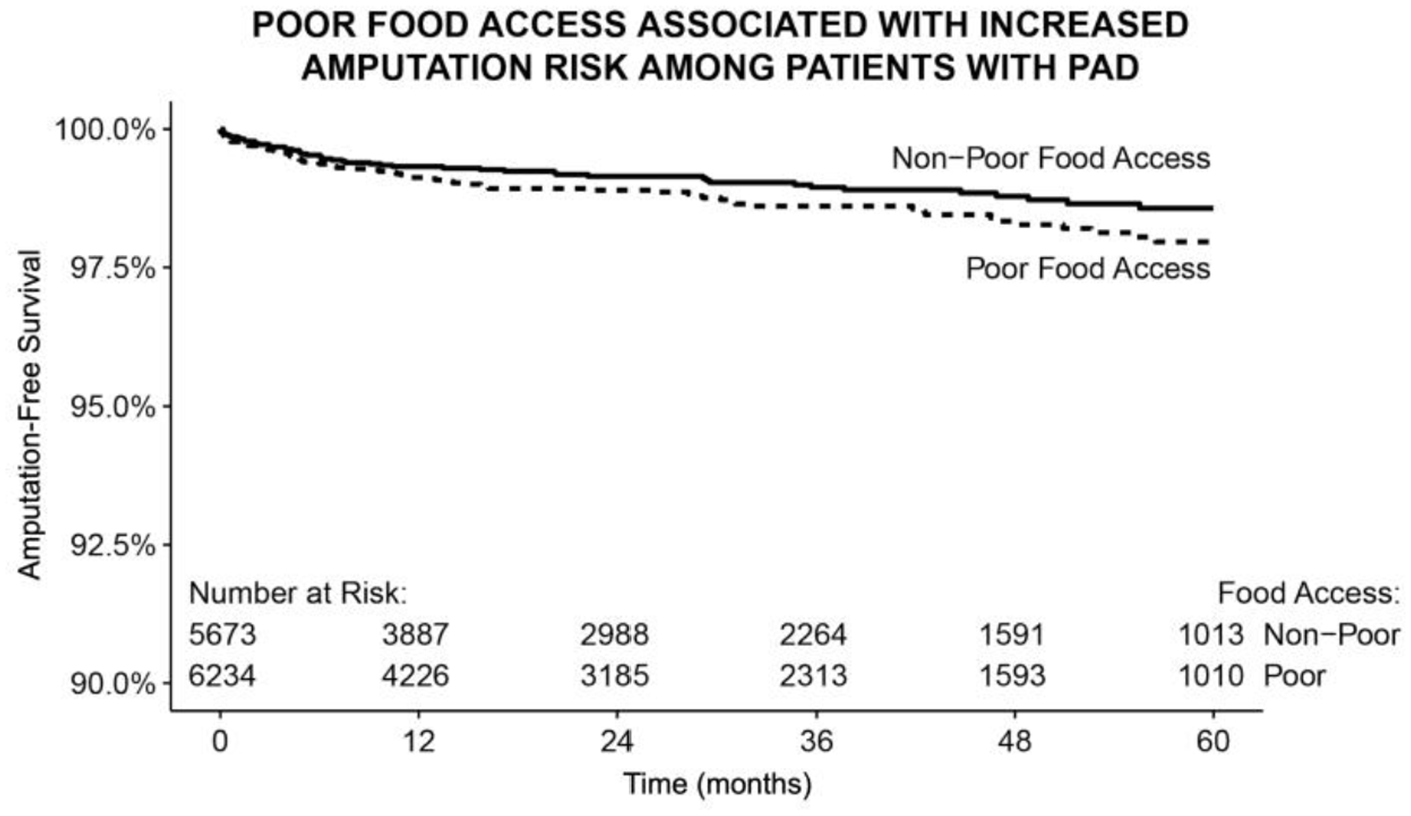
Poor food access associated with increased amputation risk among patients with PAD
Poster Number: 13
Abstract Number: 1273199
Post-pulmonary embolism syndrome: contemporary incidence and utilization of diagnostic testing in a national cohort
University of Michigan
Background: Symptoms of chest pain, dyspnea, fatigue, lightheadedness and syncope persisting more than 3 months after an acute pulmonary embolism (PE) are recognized features of post-PE syndrome. While Post-PE syndrome is increasingly recognized as an important sequela of acute PE, its contemporary incidence is unclear. Society guidelines recommend diagnostic evaluation of such patients, but the real-world utilization of diagnostic testing for identification of treatable causes of post-PE syndrome is unknown.
Methods: Retrospective cohort study of incident acute PE cases (Oct 1, 2016 - Dec 31, 2018) in a national administrative database, Clinformatics DataMart Database (Optum Insight, Eden Prairie, MN). Data were analyzed to identify ICD-10 symptom codes related to post-PE syndrome 3 to 12 months after an acute event. The utilization of diagnostic testing in the clinical workup of these patients was also assessed by CPT codes.
Results: Of 21,297 incident acute PE patients, 11,969 (56.2%) had at least one new symptom of post-PE syndrome. New dyspnea was noted in 3,268/15,203 (21.5%) patients without preceding dyspnea, followed by new malaise and fatigue in 2,894/15,643 (18.5%) patients without preceding malaise. Amongst the 11,969 patients with one or more new symptoms of post-PE syndrome, 3,242 (27%) received a CT pulmonary angiogram, 2,997 (25%) received an echocardiogram, and 325 (2.7%) received a ventilation-perfusion scan in the 3 to 12 month follow up period after an acute PE diagnosis.
Conclusion: Symptoms consistent with post-PE syndrome are common in the intermediate period following acute PE, occurring in over half of patients. Several diagnostic testing modalities are available to evaluate complications of PE, however these appear to be underutilized among symptomatic patients.
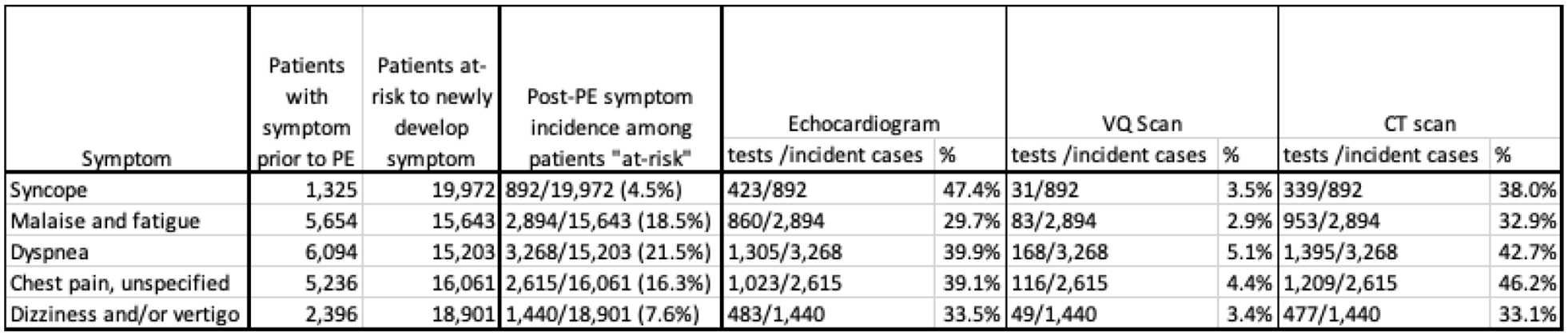
Incidence of persistent symptoms of post-PE syndrome, and utilization of key diagnostic testing modalities.
Poster Number: 14
Abstract Number: 1272909
Recurrent limb events after endovascular femoral revascularization and risk of death
1VA Boston Healthcare System, 2Brigham and Women’s Hospital, 3Maine Medical Center, 4Medical University of South Carolina
Background: Endovascular revascularization of the superficial femoral artery (SFA) may lead to recurrent ischemic syndromes, revascularization, or amputation. The impact of these events on mortality and cause of death is unknown.
Methods: We followed all patients having SFA endovascular revascularization for lifestyle limiting claudication or critical limb ischemia between 2003-2010 in 2 institutions in Boston, MA (VA Boston and Brigham and Women’s Hospital) for a median 9.3 (25%-75%: 6.8, 11.1) years. Any recurrent limb event after the initial SFA revascularization included recurrent claudication, limb ulceration or gangrene, repeat endovascular revascularization, surgical revascularization, or major or minor amputation. We used the National Death Index to determine all-cause mortality, cardiovascular mortality (coronary or cerebrovascular), or non-cardiovascular mortality. Cox-proportional hazards clustered by patient were used to estimate the hazard ratio (HR) and 95% confidence intervals (95%CI) for each endpoint by any recurrent limb event.
Results: A recurrent limb event occurred in 110 of 253 limbs and 83 of 202 patients. Recurrent limb events included 58 with claudication, 11 with ulcers or gangrene, 75 repeat endovascular revascularizations, 13 surgical revascularizations, and 16 amputations (multiple events in some limbs). At the index procedure, the average age was 68 (SD=11) years, 52 (26%) were current smokers, 52 (26%) had chronic kidney disease, 42 (21%) presented with critical limb ischemia. During follow-up there were 119 (59%) deaths, including 57 cardiovascular deaths and 62 non-cardiovascular deaths. A recurrent limb event was not associated with all-cause mortality (HR=1.0, 95%CI=0.7, 1.4), cardiovascular mortality (HR=1.6, 95%CI=0.9, 2.6), or non-cardiovascular mortality (HR=0.7, 95%CI=0.4, 1.1). Adjustment for significant factors associated with mortality (age, chronic kidney disease and critical limb ischemia) did not change these results.
Conclusion: Recurrent limb events contribute to patient morbidity, but do not increase the risk of all-cause or cause-specific mortality. Treatments that prevent recurrent limb events likely have a greater impact on morbidity than mortality.
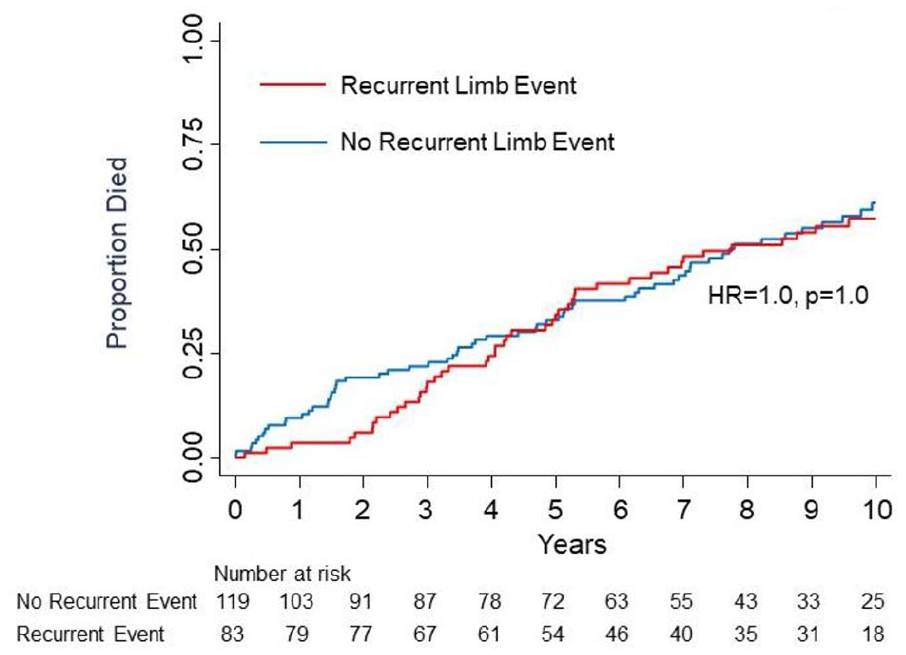
Event curves for all-cause mortality by recurrent limb event during follow-up.
Poster Number: 15
Abstract Number: 1279081
Natural history of segmental arterial mediolysis (SAM)
Mayo Clinic
Background: Segmental arterial mediolysis (SAM) is a disease of uncertain pathogenesis usually presents with arterial dissections of otherwise normal appearing arteries. The natural history, management and outcomes of these patients are largely undefined.
Methods: A single-center retrospective cohort study design was constructed to define SAM natural history, management and outcomes. Radiology reports with visceral artery dissection diagnosis were identified (January 1, 2000-December 30, 2021) across the Mayo Clinic enterprise. Charts underwent a manual review and other causes for arterial dissection were excluded including trauma, atherosclerosis, fibromuscular dysplasia, genetically mediated connective tissue diseases and confirmed vasculitis. Patient demographics, clinical presentation, management options and outcomes were collected.
Results: During the study timeframe, 147 patients (20% female, mean age 53 ± 11 years, 95% Caucasian, BMI 28 ± 8 kg/m²) with visceral artery dissection who met criteria were identified. Tobacco use was noted in 40%, hypertension in 38% and family history of dissection in 2%. Most cases were confirmed by CT angiography (99%). The most common presenting symptom was abdominal or flank pain (68%). Splanchnic arteries were involved in 73% (celiac 54%, superior mesenteric 31%, hepatic 16%, splenic 12%), renal 35%, iliac 14%, carotid 5%, and vertebral 3%. Associated aneurysms were noted in 41%. Antithrombotic management included warfarin (33%), low molecular weight heparin (4%), direct oral anticoagulants (4%), aspirin (53%) or clopidogrel (8%). Antihypertensives were used in 22% (Beta blockers 22%, ACE inhibitors 17%, angiotensin receptor blockers 8%). Statins were used in 18%. Organ infarction was common (34%) yet mesenteric ischemia was rare (1%). Few patients required either endovascular (6%) or surgical interventions (4%). Recurrent dissections (12%) were infrequent.
Conclusion: SAM is most commonly seen in middle-aged men predominantly affecting the splanchnic arteries. Despite organ infarction, conservative and medical management (including blood pressure control, antithrombotic agents) are associated with low recurrence rates and infrequent need for invasive procedures.
Poster Number: 16
Abstract Number: 1269941
Identifying genetic variants associated with cerebral atherosclerosis using an International Classification of Diseases (ICD)-10 based approach in the UK Biobank
University of Maryland School of Medicine
Background: Intracranial atherosclerotic disease (ICAD) is the leading cause of ischemic stroke in the United States. While associated with hypertension, diabetes, and smoking, genetic susceptibility and gene-environment interactions are thought to play a role. Understanding who may be at higher genetic risk can help guide preventative efforts. We aim to utilize the UK Biobank to identify genetic variants associated with ICAD.
Methods: The UK Biobank is a prospective cohort that contains data from over 500,000 individuals. We used Plink’s generalized linear model option to analyze associations between variants and cerebral atherosclerosis. Cerebral atherosclerosis was defined by the ICD-10 code I67.2. We compared cases to age, sex, and ancestry-matched controls in a ratio of 1:20.
Results: There were 384 cases of cerebral atherosclerosis and 7,680 controls. We identified 8 variants closely linked to 5 genes that had a p< 5x10-8 and a minor allele frequency of ⩾0.5%. Variants with the highest significance were identified close to sequences encoding KIAA1217 (KIAA1217: rs17513725; OR=1.56, p=1.86x10-9), USP44 (Ubiquitin specific peptidase 44: rs36064132; OR=2.06, p=1.26x10-8), METAP2 (Methionyl aminopeptidase 2: rs12818876; OR=2.01, p=1.51x10-8), TLR3 (Toll like receptor 3: rs146767297; OR=5.34, p=3.28x10-8), TBC1D5 (TBC1 domain family member 5: rs192892646; OR=4.12, p=3.64x10-8).
Conclusion: We identified multiple variants that were associated with cerebral atherosclerosis in the UK Biobank. Evidence suggests that ubiquitination is involved in the regulation of vascular inflammation and atherosclerotic plaque stability. USP44 was identified as part of a pathway responsible for foam cell formation. MetAP2 inhibitors have been shown to cause significant and sustained weight loss, a risk factor for atherosclerosis. In one study, TLR3 was up-regulated in human atherosclerotic tissue-derived smooth muscles, and in hypercholesterolemic mice, the deletion of TLR3 was associated with the accelerated onset of atherosclerosis. The mechanism explaining the association between both TBC1D5 and KIAA1217 and cerebral atherosclerosis is not known. Future studies are warranted to confirm the findings of this analysis.
Poster Number: 17
Abstract Number: 1268673
Evaluation of Takayasu’s arteritis disease activity by ultrasound localization microscopy
1Massachusetts General Hospital, 2Institute Physics for Medicine Paris, 3Georges Pompidou European hospital, APHP
Background: Use of sulphur hexafluoride microbubbles (MB) with ultrasound can provide arterial wall enhancement. The use of ultrafast imaging with MB super-localization offers the possibility of ultrasound localization microscopy (ULM) and thus a visualization of in vivo carotid vasa vasorum. We aim to perform in vivo Vasa vasorum imaging in the carotid wall in Takayasu’s arteritis and to provide a correlation with the disease’s activity.
Methods: Patients with Takayasu arteritis were consecutively included in the national referral centre. Assessment of activity was performed by NIH activity index, with measurement of biological inflammation, morphological evaluation by computed tomography (CT) angiography, and 18-fluorodeoxyglucose CT scan. Ultrafast ultrasound imaging was performed with a 7 MHz central frequency linear probe. A dedicated contrast imaging sequence (plane waves with 8 angles, frame rate 500 Hz, voltage 8 V, duration of 8 s), coupled with the intravenous injection of sulphur hexafluoride MB allow us to store the raw radio frequency data of the MB passage. After a pre-processing step to accumulate frames properly including a frames selection and a movement correction, the MB were localized then tracked, allowing reconstruction of the vasa vasorum. The inflammation was quantified through MB tracked and normalized for inter acquisition comparison.
Results: 16 patients were included. 5 patients (median age 35.8 [24.5–46.0] years, 3 women) had active disease and 11 patients (37.2 [31.7–47.3] years, 9 women) had quiescent disease. The passage of MB allowed the visualization of microvessels within the arterial wall for active cases (Figure). The number of MB detected per second in the wall was 118 [80–169] for active cases vs. 13 [10–15] for quiescent cases (p=0.0005) (Figure). The sum of the length of the tracks, i.e. the MB path per second of acquisition, was computed with a significant difference between the two groups (43.0 mm [32.9–65.5] in active TA vs 4.6 mm [2.9–5.4]).
Conclusion: ULM allows visualization of microvessels within the carotid wall, with significantly greater MB passage in active Takayasu arteritis.

Ultrasound localization microscopy of two cases of Takayasu arteritis: 1 active case (top) and 1 quiescent case (bottom).
Poster Number: 18
Abstract Number: 1269616
Randomized, controlled trial of a digital therapeutic app providing nutritional cognitive behavioral therapy for the treatment of Type 2 diabetes
Judith Hsia, MD1, Nicole L. Guthrie, MS2, Paul Lupinacci, PhD2, Ananda Gubbi, PhD3, Douglas Denham, DO4, Mark A Berman, MD2,
1University of Colorado, 2Better Therapeutics, 3CPC Clinical Research, 4Clinical Trials of Texas
Background: Type 2 diabetes (T2D) prevalence is increasing in the context of sedentary lifestyle and non-optimal diet. Successful adoption and maintenance of comprehensive behavioral changes to potentially lower vascular risk remain challenging. BT-001 is a digital therapeutic designed as a scalable, engaging, interactive mobile application that provides personalized, nutritional cognitive behavioral therapy (nCBT) to improve glycemic control.
Methods: Adults with hemoglobin A1c (A1c) >7% were randomized (1:1) to receive access to BT-001 or a control app, both on top of standard of care. The primary endpoint, treatment group difference in mean A1c change from baseline to 90 days, was assessed by analysis of covariance.
Results: Mean age of the 669 subjects was 58 years, body mass index 35 kg/m2, A1c 8.1%; 56% were female, 30% Black and 15% Latino. Treatment group difference in mean A1c change from baseline was -0.4% (95% confidence interval -0.5, -0.2; p< 0.001) (Figure). A dose response was observed, with greater A1c reduction among subjects completing more behavioral therapy. No adverse events were attributed to app use and no adverse device effects reported.
Conclusion: Delivery of a cognitive behavioral intervention via smartphone app can provide a scalable option for improving glycemic control in patients with T2D.
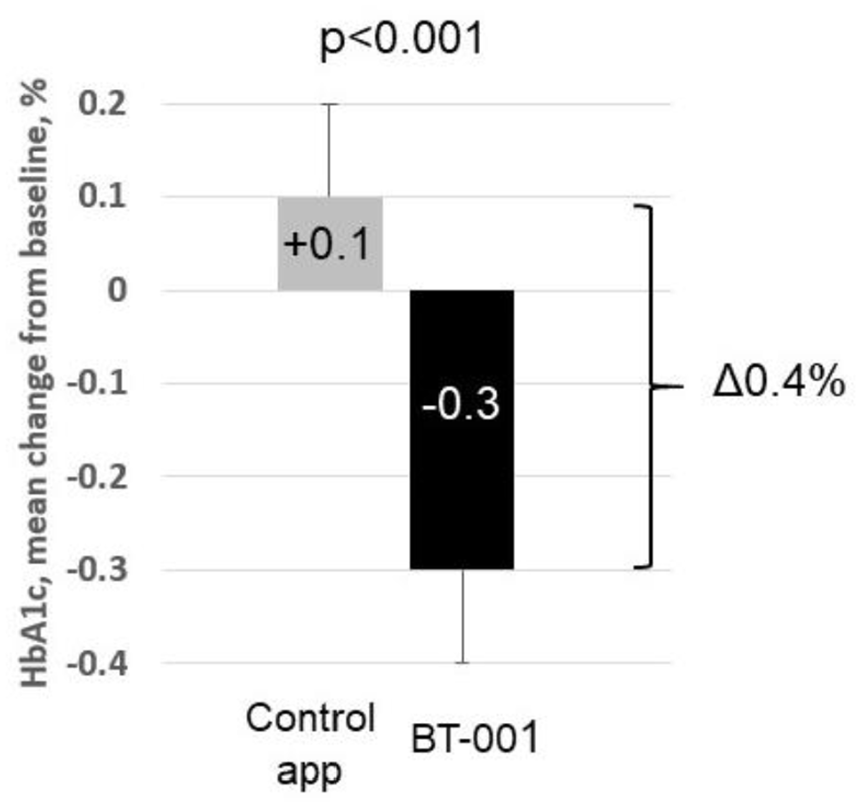
HbA1c change from baseline to day 90 (mean, 95% CI) by randomized treatment group.
Poster Number: 19
Abstract Number: 1262156
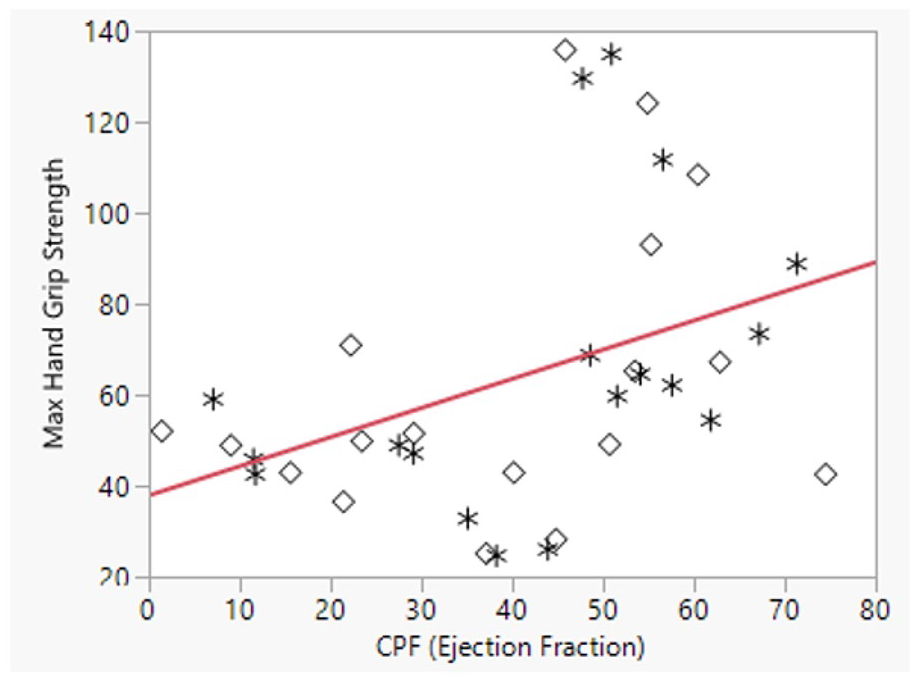
Relationship between hand grip strength and calf muscle pump function
1University of Missouri- Columbia School of Medicine, 2Mayo Clinic
Background: Hand grip strength (HGS) has been conventionally used to describe frailty and is associated with higher mortality. Reduced calf muscle pump function (CPF) has been shown to be an independent risk factor for venous thromboembolism (when CPF < 23%) and mortality (when CPF < 45%). We sought to evaluate the relationship between HGS and CPF in patients who present for venous plethysmography in the Gonda Vascular Center.
Methods: Consecutive patients referred to the Gonda Vascular Lab for non-invasive venous studies were identified and consented. Subjects underwent standard venous air plethysmography protocol. CPF was measured as an ejection fraction comparing refill volume after ankle flexes and passive refill volumes. HGS was obtained (3 trials per hand) using a dynamometer and the maximum value was recorded per hand. HGS and CPF were compared (right hand to calf, left hand to calf) and correlation between the measures was evaluated with an R2 value. Receiver operator curves (ROC) were used to determine optimal cutoff values of HGS to predict reduced CPF.
Results: A total of 18 patients (36 hand-calf pairs) were consented and evaluated. The mean age was 55.9 years and 67% were female (n=12). The mean weight was 88.2 kg and mean height was 169 cm (mean BMI 30.7). The median CPF (per calf), was 41% (SD 19.6) and the mean max HGS (per hand) was 64.1 lbs. Comparing each hand/calf pair, a weak positive correlation was identified between HGS and CPF (p-value=0.02, R2= 0.16). CPF was then stratified as reduced (< 45% or < 22%) or not reduced per limb and patients were categorized as reduced CPF if either limb had dysfunction. The mean of the lowest HGS (per hand) was used to predict a reduced CPF. A HGS < 59.7 was predictive of a reduced CPF (< 45%) with an area under the curve of 0.96 (p< 0.001) but was a poor predictor of more pronounced CPF dysfunction (< 22%), AUC 0.71 (p=0.07).
Conclusion: A weak correlation between HGS and CPF was observed per limb, indicating reduced muscle strength may be one explanation for reduced CPF. A HGS < 59.7 was strongly predictive of reduced CPF (< 45%) but was unable to accurately predict a CPF < 23%, indicating a potential independent role for CPF evaluation for venous thromboembolism risk prediction.
Poster Number: 20
Abstract Number: 1269972
Utilizing an International Classification of Diseases (ICD)-10 based approach to identify genetic variants associated with peripheral artery disease in a large-scale biomedical database
University of Maryland School of Medicine
Background: Peripheral artery disease (PAD) is recognized as a major cause of cardiovascular morbidity and mortality with an estimated prevalence of more than 230 million cases worldwide. While PAD is associated with risk factors such as smoking and diabetes, genetic factors likely have a role in PAD, especially in cases of premature PAD. Understanding who may be predisposed to PAD may help guide preventative efforts. We aim to utilize the UK Biobank to identify genetic variants associated with PAD.
Methods: The UK Biobank is a prospective cohort that contains data gathered from over 500,000 individuals. We used Plink’s generalized linear model option to analyze associations between single nucleotide polymorphisms (SNPs) and phenotypic manifestations of the disease. We defined PAD by selecting the ICD-10 codes I702, I7020, I7021. We compared unrelated cases to age, sex, and ancestry-matched controls with a case-to-control ratio of 20:1.
Results: There were 961 and 557 instances of peripheral artery disease as a primary or secondary diagnosis, respectively. We identified 102 variants closely linked to 16 genes that had a p < 1 x 10-6. Of those, 69 variants closely linked to the CDKN2B-AS1 gene met the threshold for statistical significance (5 x 10-8). All identified genes had a minor allele frequency of ⩾ 0.5%. Variants with the highest significance were identified in close proximity to sequences encoding CDKN2B-AS1 (CDKN2B antisense RNA 1: rs10757277; OR = 1.33, p = 1.2 x 10-11), LZTS1-AS1 (LZTS1 antisense RNA 1: rs181485652; OR 2.83, p = 7.31 x 10-8), LPA (Lipoprotein(A): rs55730499; OR = 1.44, p = 1.05 x 10-7) and TENM2 (Teneurin Transmembrane Protein 2: rs190548234; OR 1.99, p = 1.77 x 10-7).
Conclusion: We identified multiple genetic variants that were associated with the phenotype of peripheral artery disease in the UK Biobank. The rs10757277 variant was previously reported in patients with coronary artery disease and subclinical atherosclerosis, supporting the notion that it is likely involved in multi-system atherosclerosis. Although not reaching statistical significance, LPA is known to be associated with coronary artery disease. Future studies are warranted to confirm the findings of this analysis.
Poster Number: 21
Abstract Number: 1273833
Calf muscle pump function and mortality
Mayo Clinic
Background: Calf muscle pump (CMP) is a major contributor to cardiac preload. CMP failure has been associated with increased mortality. We sought to determine whether mortality outcomes were a graduated response to varying degrees of reduced CMP ejection fraction.
Methods: Consecutive adult patients who underwent venous air plethysmography testing at the Mayo Clinic Gonda Vascular Laboratory (January 1st, 2012 – January 1st, 2022) were divided into sextiles based on calf pump ejection fraction (EF): > 50%, 40 – 49%, 30 – 39%, 20 – 29%, 10 – 19% and < 10% for the assessment of overall survival. Patients with venous incompetence, venous obstruction, or unilateral calf pump dysfunction were excluded. Mortality rates were calculated using the Kaplan-Meier method.
Results: Over the study timeframe, 6,229 patients met the inclusion criteria. During the follow-up period, there were 408 deaths. Mortality rates were increased with decreasing CMP EF. Kaplan-Meier survival at 10 years demonstrated incremental mortality rate decrement with worsening EFs (Log-rank p< 0.001; Figure).
Conclusion: Reduced CMP function adversely impacts mortality rates which appear to be a graduated response. Mortality rates worsen with each 10% decrement in CMP EF.
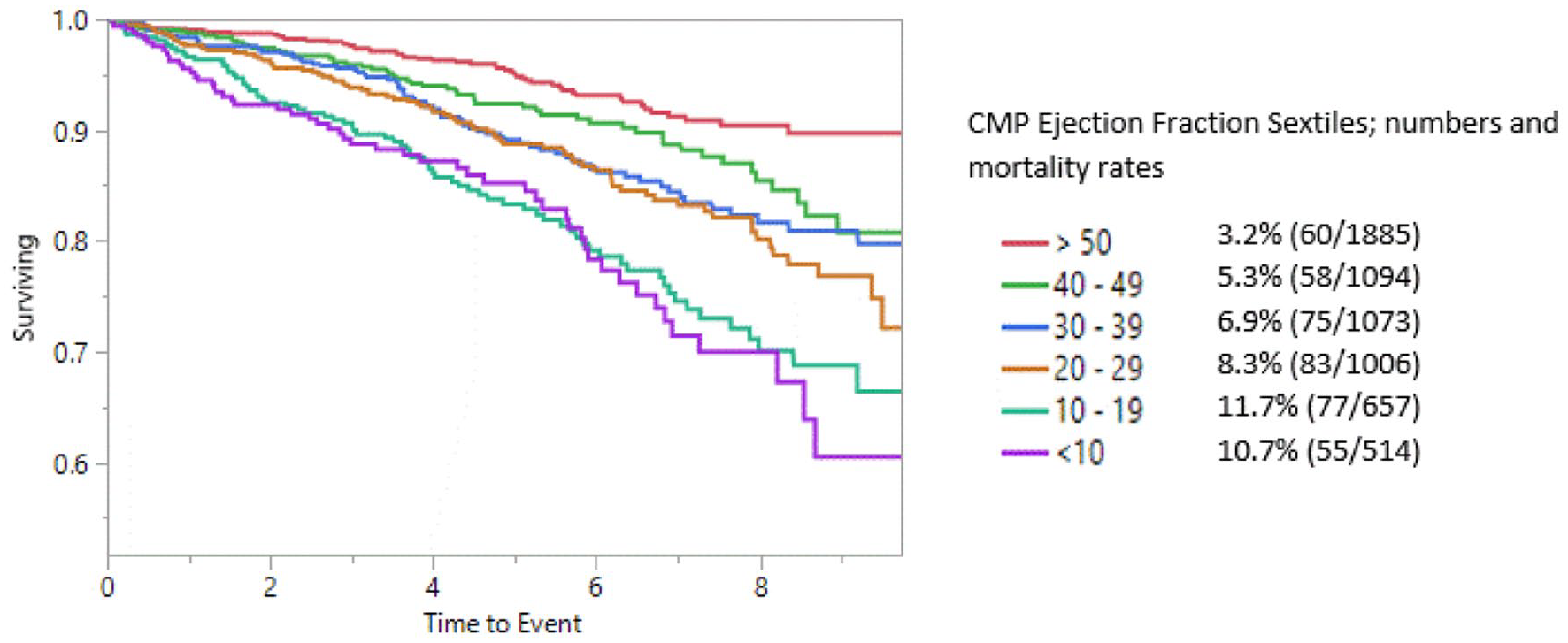
Kaplan-Meier survival analysis.
Poster Number: 22
Abstract Number: 1278736
Effect of course length on total distance walked during monitored 6-minute walk test within a randomized clinical trial
1CPC Clinical Research, 2University of Colorado Anschutz Medical Center, 3Harvard Medical School
Background: The 6-minute walk test (6MWT) is an established functional endpoint used in randomized trials of novel therapies and for registration. A limitation of functional outcomes, including 6MWT, is data variability which diminishes power to detect a significant difference between arms. Understanding the impact of test administration variations on total distance walked (TDW) is of importance. Due to differences in maximum available course lengths (CL) among sites, a common question is whether allowing multiple CLs within a study will add variability to TDW.
Methods: The Colorado Prevention Center functional core lab database was utilized. Tests completed in patients with amyloid heart disease, ATTR-CM, on two CLs (20 m and 30 m) were analyzed. The mean and standard deviation for TDW by CL were calculated on aggregate data.
Results: A total of 1,515 6MWTs from a Phase 3 registration pathway randomized trial of ATTR-CM conducted in 804 patients at 99 sites were included. Of these, 669 (44.2%) 6MWTs were conducted on a 20 m course and 846 (55.8%) on a 30 m course. The mean TDW was 346 m (SD 106.04) for 20 m courses and 347 m (SD 105.72) for 30 m courses. There was no significant difference in TDW by CL (p=0.54).
Conclusion: Using both 20 m and 30 m courses in a multisite trial using 6MWT as an outcome does not appear to result in significant differences in TDW. These observations may impact site feasibility for studies by including those that only have access to shorter courses. In addition, efforts to minimize variability may focus on aspects other than CL.
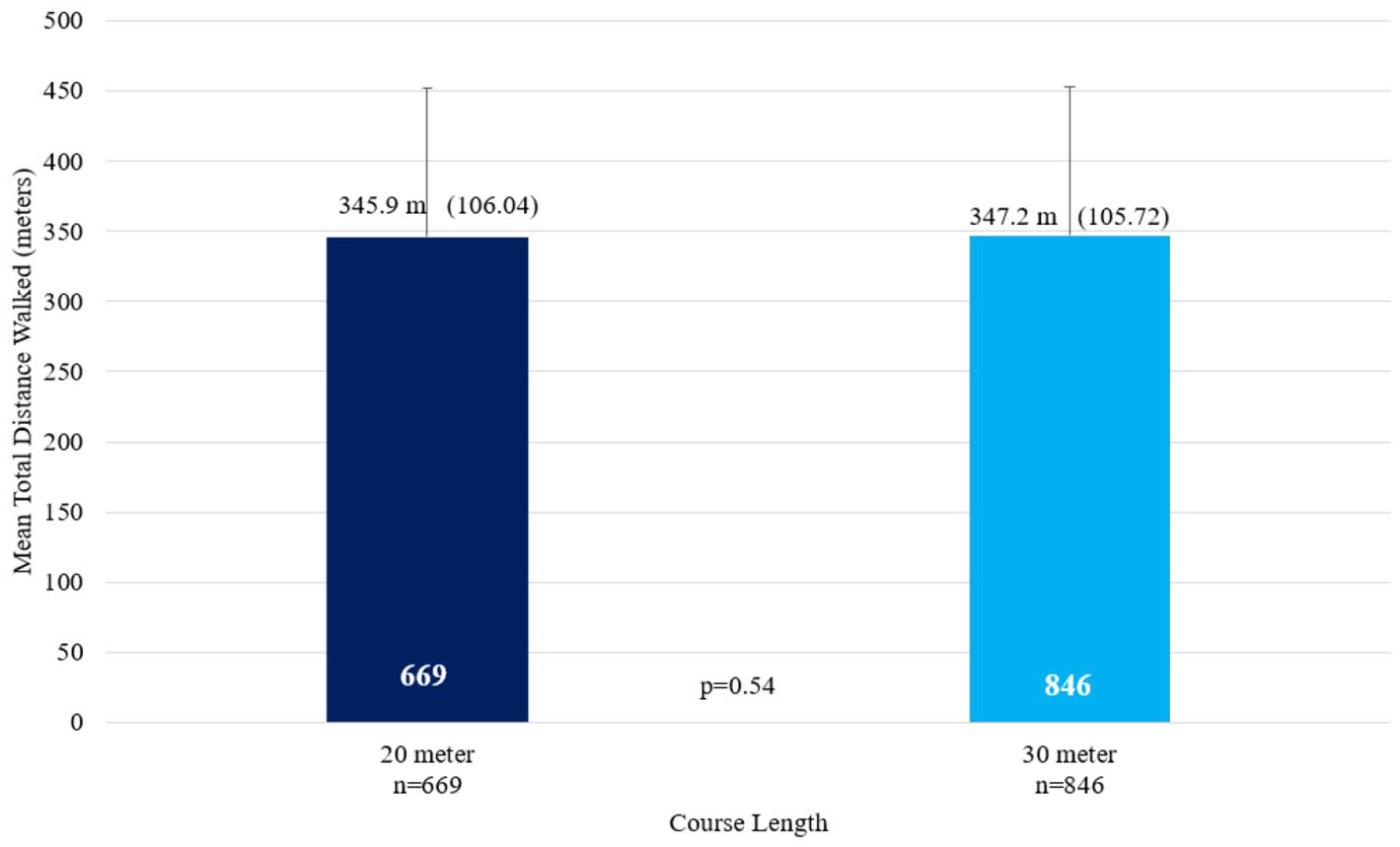
Total distance walked by course length.
Poster number: 23
Abstract Number: 1269060
Development and validation of knowledge attitudes and practices questionnaire on venous thromboembolism prophylaxis of internists in a tertiary hospital in Tarlac City, Philippines
Angela Apostol-Alday, MD, FPCP, FPCC, FPSVM1,
1Central Luzon Doctors Hospital, 2Jecsons Medical Center
Background: The leading cause of hospital-related death is venous thromboembolism (VTE). Venous thromboembolism is a preventable cause of in-hospital death and there are several guidelines that recommend VTE prophylaxis in different specialties. Currently there is no validated questionnaire to assess the knowledge, attitudes and practices (KAP) on VTE prophylaxis that is tailored for Filipino physicians. The researchers aimed to develop and validate a questionnaire assessing the knowledge, attitude and practices on venous thromboembolism prophylaxis of internists.
Methods: Literature review and focused group discussions were done during questionnaire formation. There were 10 participants in the pilot testing, 10 participants for face validity and three experts for content validity. Content validity was tested using Good and Scates. Internal consistency was tested using Cronbach’s alpha coefficient. Phase 5 was full validation based on the findings of the pilot study and there were 35 internists who consented to participate in this phase.
Results: The VTE-KAP questionnaire was considered applicable by the participants from the pilot testing, face validity and content validity. Average score using Good and Scates for content validity was 3.83 which is considered very good. The VTE-KAP questionnaire had 25 items under three domains: knowledge, attitude and practices which had 10, 20, and 5 items, respectively. The Cronbach’s alpha was 0.813.
Conclusion: The VTE-KAP questionnaire appeared to be valid and reliable for assessing KAP regarding VTE prophylaxis. Survey of internists from our institution showed that a good baseline knowledge on VTE prophylaxis and favorable response towards formulation, application and implementation of VTE prophylaxis protocol in the hospital. However, there were disparities in the knowledge and actual practice on VTE prophylaxis which seemed to be influenced by several factors: cost-effectiveness, local availability and practicality of the specific mode of prophylaxis. The VTE-KAP questionnaire has potential application in future large-scale surveys as it can serve as a starting point in the formulation, application and implementation of VTE prophylaxis protocol in the different hospitals.
Poster Number: 24
Abstract Number: 1276594
The association of clinical characteristics with insulin induced endothelial cell nitric oxide phosphorylation
1Boston Medical Center, 2Boston University School of Medicine
Background: Insulin has an important role in maintaining vascular endothelial function. Insulin mediates the endothelial cell (EC) nitric oxide (No) production which leads to vasodilation and increased blood flow. Insulin resistance decreases the NO bioavailability contributing to the development of cardiovascular disease. Phosphorylation of endothelial nitric oxide synthase (peNOS) results in activation of NO. We aimed to investigate the association between clinical characteristics and fold change in insulin induced peNOS.
Methods: We used data from isolated endothelial cells of 54 individual sample. We used bivariate correlation analysis to evaluate the association of the clinical characteristics including age, sex, race, BMI, glucose, total cholesterol, LDL, HbA1c and the presence of diabetes with fold change in insulin stimulated peNOS.
Results: Samples from 54 participants were included in the analysis. The mean age was 52 (SD ± 9), 55% of the participants were male and 33% were white. Mean BMI was 29 (SD ± 6). 59% had diabetes. Mean glucose, HbA1c, total cholesterol and LDL were 129 mg/dL (SD ± 56), 6.8 (SD ± 1.6), 189 mg/dL (SD ± 39) and124 mg/dL (SD ± 97) respectively. Higher BMI was inversely associated with insulin stimulated peNOS (Table). Also, glucose level, HbA1c, and diabetes were shown to decrease insulin stimulated fold change of peNOS. Sex, race and lipid levels did not show an association with change in peNOS.
Conclusion: Our results suggest that increased BMI, presence of diabetes, higher HbA1c and glucose levels have adverse effects on endothelial cell function, whereas no association between endothelial cell function and sex and race was found.

Correlation of clinical characteristics and insulin induced peNOS.
Poster Number: 25
Abstract Number: 1278363
Underuse of high intensity statins in carotid surgery patients
Fernando Belcastro, Pablo Elissamburu, Ghibaudo Sebastian, Ignacio De Luca
Instituto Cardiovascular de Buenos Aires (ICBA)
Background: Patients with carotid disease are at high risk of cardiovascular events and benefit from aggressive secondary prevention, the high intensity statins treatment should by prescribe; besides the statins are recommended in the perioperative field to reduce perioperative events due to pleiotropic effects. Little is known about patterns of statins use. In terms of type, intensity and the LDL target in the patients who goes to carotid surgery.
Methods: From October 2015 to October 2018, 248 consecutive patients undergoing CEA were analyzed in a retrospective study. We evaluated the use of statins, and the intensity of the treatment. The use, the type and the intensity of statins was examined in these patients. We followed the guidelines recommendations in this population in terms of the necessity of high intensity statins and the LDL target (less 70m/dl).
Results: Of the 248 patients 215 were taking statins, of these patients only 51.6% were treated with high intensity statins. With respect to the LDL target, only 38% reach to the LDL less 70 mg/dl. In the Table, we describe the use of type and statins dose.
Conclusion: Despite improvement in the use of cardioprotective medications over time, patients with carotid disease in carotid surgery plan remain with low compliance with the guidelines in terms of intensity and LDL target.
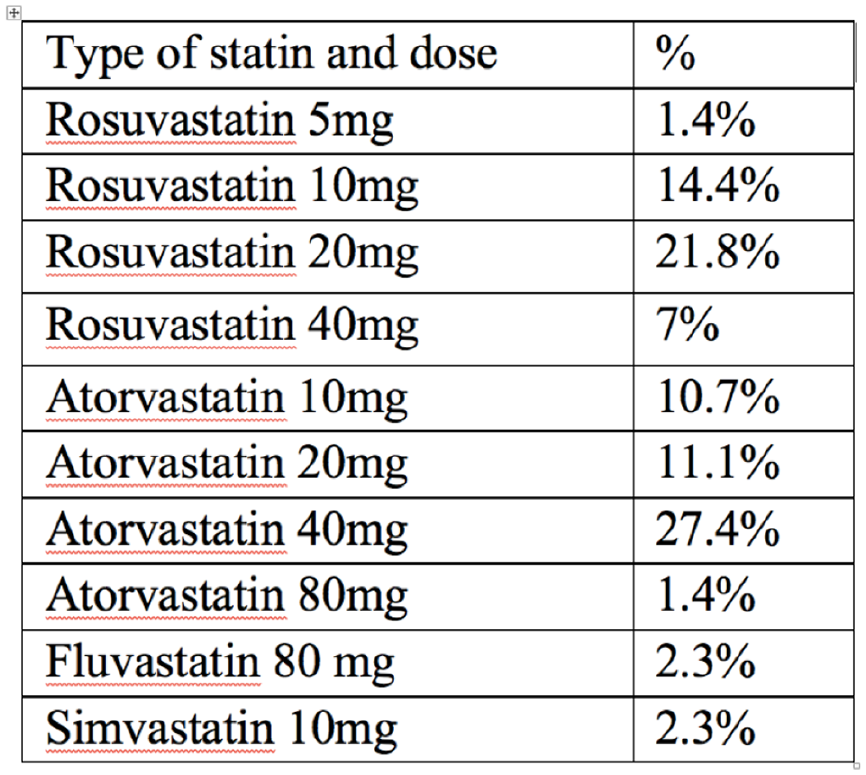
Types of statins and doses.
Poster Number: 26
Abstract Number: 1273765
Test re-test reliability of the Peripheral Artery Disease Quality of Life Questionnaire (PADQOL)
1Minneapolis VA Healthcare System, 2University of Minnesota
Background: The Peripheral Artery Disease Quality of Life Questionnaire (PADQOL) is a validated disease-specific questionnaire developed to assess the impact of PAD on patients’ perceptions of health-related quality of life, specifically the physical, psychosocial, and emotional impact PAD has on one’s life. The purpose of this study was to establish test re-test reliability of the PADQOL.
Methods: Eligible participants (n =52) completed five questionnaires at two time points: the PADQOL, Short-form 36 (SF-36), Profile of Mood States (POMS), Walking Impairment Questionnaire (WIQ), and a demographic form. Participants were recruited from prior studies and through targeted recruitment mailings. The time between timepoints was 2-4 weeks. Intraclass correlation coefficients were conducted to measure reproducibility (reliability).
Results: Intraclass correlations were as follows: Factor 1: social relationships and interactions 0.97 (CI 0.94 - 0.98), Factor 2: self-concept and feelings 0.95 (0.92 - .973), Factor 3: symptoms and limitations in physical functioning 0.93 (0.88 - 0.96), Factor 4: fears and uncertainty 0.93 (0.88 - 0.96), Factor 5: positive adaptation 0.84 (0.72 - 0.91), job interference 0.79 (0.62 - 0.88), sexual function 0.86 (0.75 - 0.93) and intimate relationships 0.77 (0.59 - 0.87). This study is limited by the small sample size and non-diverse sample.
Conclusion: These results indicate that the PADQOL is highly reliable. Overall, scores showed "high" (0.61-0.80) (job interference and intimate relationships) or "almost perfect" (0.81-1.00) reliability (Factors 1-5 and sexual function) (Cronbach α >0.8). The PADQOL provides a meaningful measure of disease impact and is a useful tool to assess the effectiveness of treatments based on patient-centered outcomes.
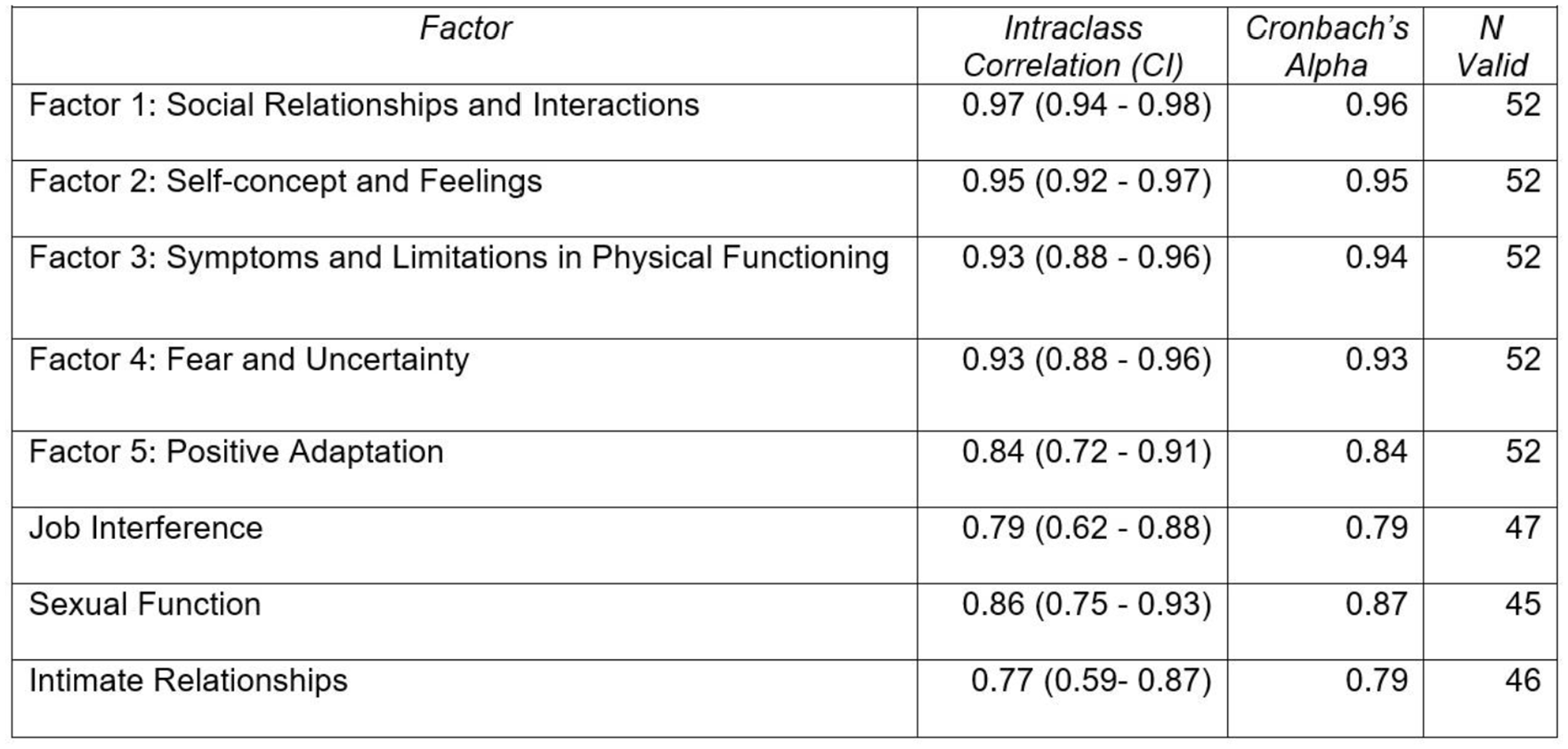
Intraclass correlation coefficients for PADQOL test retest.
Poster Number: 27
Abstract Number: 1273800
Development of a predictive screening tool for improved detection of peripheral artery disease (PAD): The PREDICT PAD study
1Minneapolis VA Healthcare System, 2University of Minnesota
Background: Of all the major manifestations of atherosclerosis, peripheral artery disease (PAD) is one of the most underdiagnosed and undertreated vascular diseases, due, in part, to the large number of individuals who experience atypical symptoms, yet our current screening tools are designed to detect those with classic symptoms. The purpose of this study was to determine which, if any, symptom descriptors accurately discriminate peripheral artery disease (PAD) from non-PAD in a community-based sample of individuals with self-reported persistent lower extremity symptoms of any kind.
Methods: Using a prospective cross-sectional design, symptom descriptors were linked to PAD disease status using diagnostic testing in individuals who report lower extremity symptoms (n = 25). Consecutive sampling was used to identify those with atypical symptoms in the population. Symptom descriptors were obtained via questionnaires and structured interviews. Symptoms were assessed pre and post physical function tests. Calf muscle tissue oxygenation level was measured using near infrared spectroscopy to further differentiate ischemic vs. non-ischemic symptoms during exercise. The primary outcome was the diagnostic accuracy of patient-reported symptoms that discriminate between PAD and non-PAD conditions.
Results: Four questions discriminated between groups. These were: “Does the pain/discomfort every disappear while you are walking?” “Do you have trouble keeping up with your friends or family?”, “Do you have pain or discomfort while sitting”, and “Where is the pain?”. Pain or discomfort while sitting occurred more frequently in the PAD group compared to the non-PAD group as well as pain or discomfort outside of the calf or thigh. Questionnaires had low sensitivity and specificity and were not more accurate following a bout of exercise.
Conclusion: Low diagnostic accuracy of the questionnaires may be attributed to the high prevalence of participants in the PAD group who experience pain while sitting and pain outside of the calf and thigh. Furthermore, inclusion of more women than men may have better represented the breadth of atypical symptoms experienced by those with PAD.
Poster Number: 28
Abstract Number: 1272900
Exercise therapy for symptomatic peripheral artery disease: could we do better?
University of Colorado School of Medicine
Background: Supervised exercise therapy (SET) carries a Class I recommendation for symptomatic peripheral artery disease (PAD). SET with lower extremity revascularization (LER) is superior to either therapy alone to improve function. CMS has covered SET since 2017; however, barriers to utilization remain including reimbursement ($56.85 per session vs. $118.55 for cardiac rehabilitation); lack of provider awareness and access. We evaluated referral of either home-based or SET in patients with LER for symptomatic PAD.
Methods: Medical records of patients who underwent LER from July 2016 to July 2021 at Denver Health and University of Colorado were reviewed for referral at any time to either home-based or SET.
Results: Among 1,103 patients, 35% were women, 19% Black, 21% Latino and 86% resided locally. The proportion with pre-procedural Rutherford class 2-5 was 7, 20, 22 and 42%, respectively. Overall, 10 patients (0.9%) were referred for home-based and 24 (2.2%) for SET – all by cardiologists (Figure). There were no institutional differences.
Conclusion: Despite a Class I recommendation in PAD guidelines, referral for home-based or SET was low in both a large academic medical center and an urban safety net hospital system.
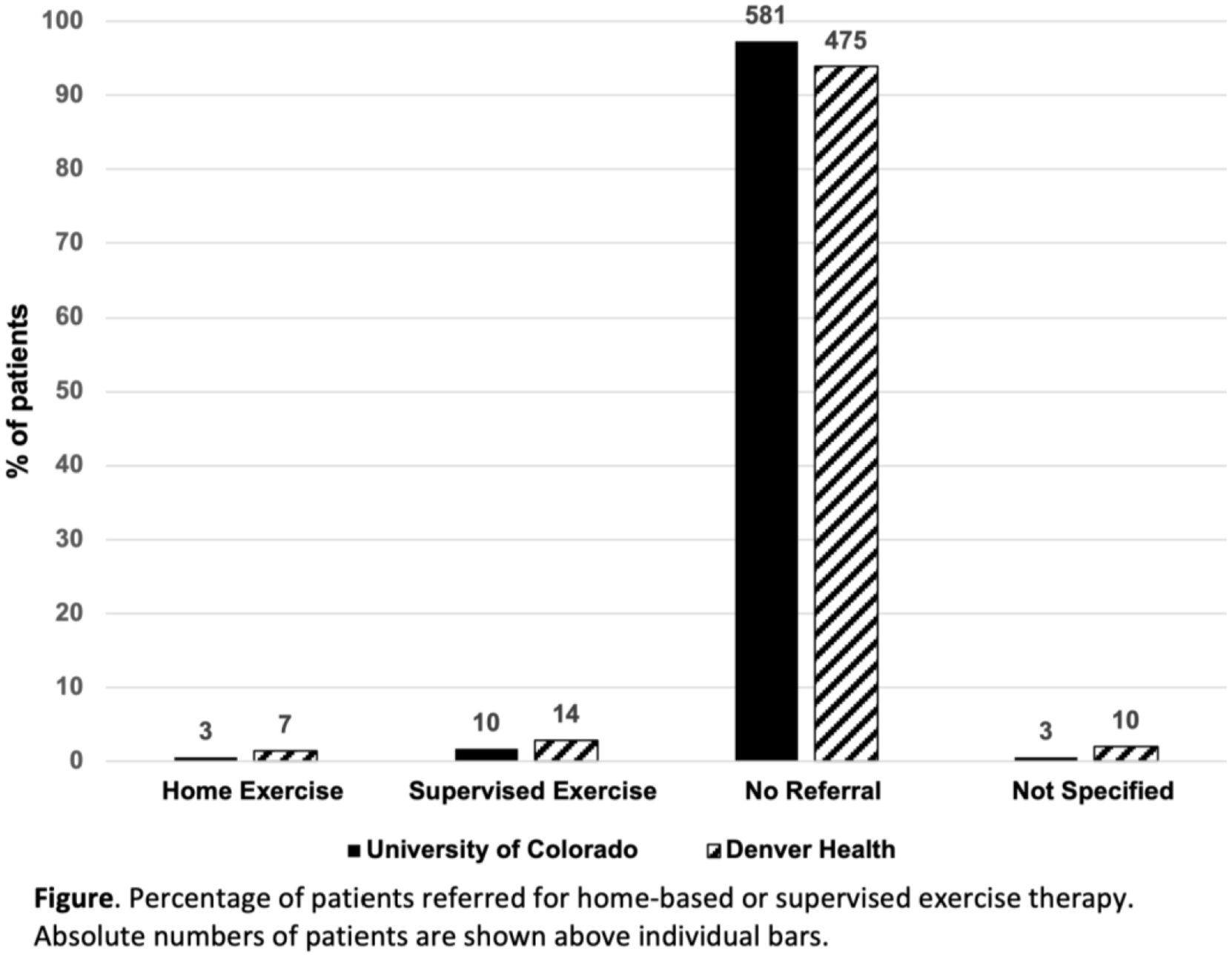
Rates of referral for exercise therapy in patients with symptomatic PAD.
Poster Number: 29
Abstract Number: 1272983
Sex differences in guideline-directed medical therapy in 2021-22 among patients with peripheral artery disease (PAD)
1CPC Clinical Research, 2University of Colorado School of Medicine
Background: Guideline-directed medical therapies (GDMT) for peripheral artery disease (PAD) include antiplatelets, statins, smoking cessation, blood pressure and glycemic control. The 2021 AHA Scientific Statement on PAD highlighted underuse of GDMT. Understanding whether these deficiencies differentially impact subpopulations with PAD may inform strategies to improve care.
Methods: To identify sex differences which could benefit from targeted efforts to implement GDMT, we extracted de-identified data from TriNetX for adults with healthcare encounters with a diagnosis of PAD from May 2021-April 2022 in the University of Colorado health system. Categories were compared by chi-square. The Colorado Multiple Institutional Review Board provided a waiver of informed consent.
Results: Among 9,810 patients with PAD, 50.1% (n=4,910) were women. Women were less likely than men to receive GDMT overall and in the subset with no history of coronary artery disease (CAD) (Figure, all p< 0.0001). Even among patients with concurrent diabetes or chronic kidney disease, women were less likely to receive angiotensin-converting inhibitors or angiotensin receptor blockers (all p< 0.0001).
Conclusion: Implementation of GDMT among PAD patients is particularly low among women regardless of CAD history.
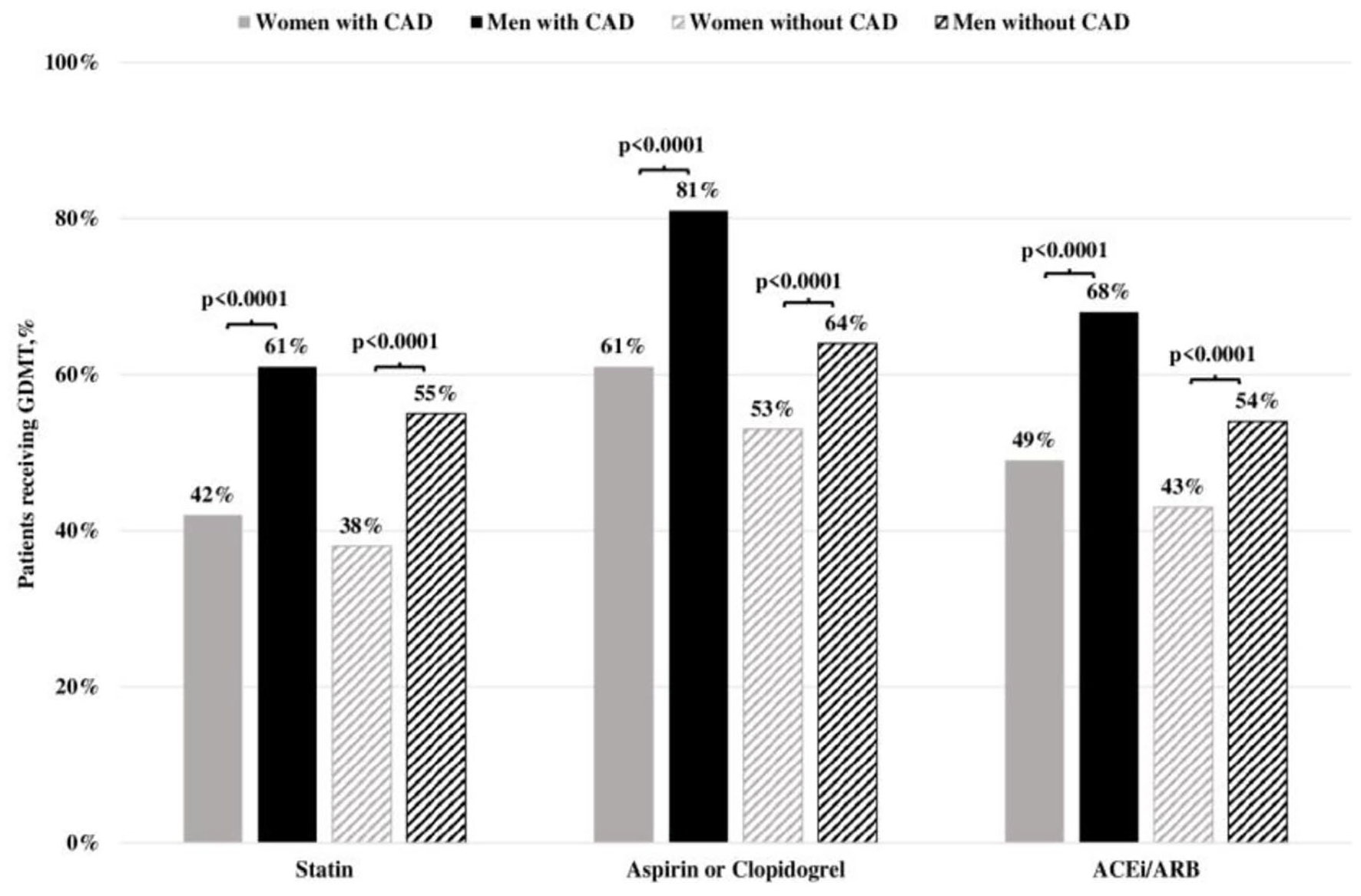
GDMT use in women and men with PAD with and without CAD.
Poster Number: 30
Abstract Number: 1272161
Guideline medication adherence patterns and physical activity in people with peripheral artery disease: a multiethnic study of atherosclerosis study
1Stanford School of Medicine, 2Stanford Vascular Surgery, 3Family Medicine and Public Health
Background: Patients with lower extremity peripheral artery disease (PAD) are recommended to take aspirin, statins and indicated antihypertensives to reduce the risk of major adverse cardiovascular events. However, trends in adherence to all three medications and their combined impact on patient-reported outcome measures such physical activity at home remains understudied.
Methods: We analyzed baseline and follow-up data from 6814 participants between 45 and 84 years from the Multi-Ethnic Study of Atherosclerosis Study (MESA). PAD was defined as having at least 1 exam with an ankle brachial index (ABI) < 0.9 across one of three exams in the 10-year duration of the study. Guideline therapy use in people with PAD was defined as taking aspirin, statin and indicated anti-hypertensives for at least one exam at the time of abnormal ABI or thereafter. Suboptimal therapy users were participants who were never on guideline therapy at any study visit. Physical activity data was derived from the MESA Typical Week Physical Activity Survey.
Results: Only 37.8% of participants were on guideline therapy for at least one exam, and only 2% were on guideline therapy for all three exams. Baseline factors associated with the odds of being on all three guideline-recommended therapies for at least one exam were being male OR: 1.53 (95% CI 1.18-2.00), having diabetes OR: 3.11 (95% CI 2.14-4.50), hypertension OR: 3.16 (95% CI 2.41-4.14), health insurance OR: 1.89 (95% CI, 1.04-3.43) and an ABI less than 0.6 at baseline OR: 2.96 (95% CI, 1.23-7.09). Multivariate linear regression models indicated no significant associations between guideline-therapy use and total reported physical activity (p=0.780).
Conclusion: We found underutilization and inconsistent use of guideline recommended therapy in a multi-ethnic cohort of people between 45 and 84 years with PAD. Those on guideline therapy were more likely to be men, have other comorbidities, more severe PAD and have health insurance compared to those on suboptimal therapy at baseline. Further research is needed to identify patient-centered outcomes modulated by medication adherence which may increase patient compliance with medication regimens.
Poster Number: 31
Abstract Number: 1257056
Acute lower limb arterial thrombosis in COVID-19 infected patients: Experience in a national hospital in Peru
Edgardo Rebagliati Martins National Hospital
Background: The COVID-19 pandemic has been associated with a series of clinical vascular conditions such as Acute Lower Limb Arterial Thrombosis (ALLAT) and has been associated with high morbidity and mortality and loss of the affected limb. The study aimed to describe the clinical and surgical characteristics of COVID-19 infected patients with ALLAT in a national hospital in Peru.
Methods: Observational, descriptive, and retrospective study conducted at the Edgardo Rebagliati Martins National Hospital from March 2020 to February 2022. The main variables considered were the clinical stage of COVID-19, laboratory tests, grade, time and location of ALLAT, treatment, type of amputation, mortality, and 30-day survival.
Results: 96 patients (mean age, 62.9 years) were analyzed, mainly males (61.45%), and the main comorbidity was diabetes (54.16%). The mean ALLAT time was 11.5 hours, and 25% of all patients had severe COVID-19 infection. The main Rutherford Score was IIB (32.29%), and the main affected arteries belonged to the femoro-popliteal (superficial femoral, 41.81%) and infra-popliteal (anterior tibial, 39.67%) segments. Thromboembolectomy (60.41%) was the main surgical treatment, and 55.17% of patients ended in amputation. Survival and 30-day mortality were 46.8% and 53.2%, respectively. The main causes of mortality were severe respiratory distress (69.41%) and septic shock (22.94%).
Conclusion: Early diagnosis and timely management of ALLAT determines an important factor for patient prognosis; however, associated comorbidities, the severity of COVID-19 infection, prolonged ischemia times, over-aggregated infection, and related hyperinflammatory states ultimately direct the patient’s fate towards a series of complications including amputation, functional limitation, and associated mortality.
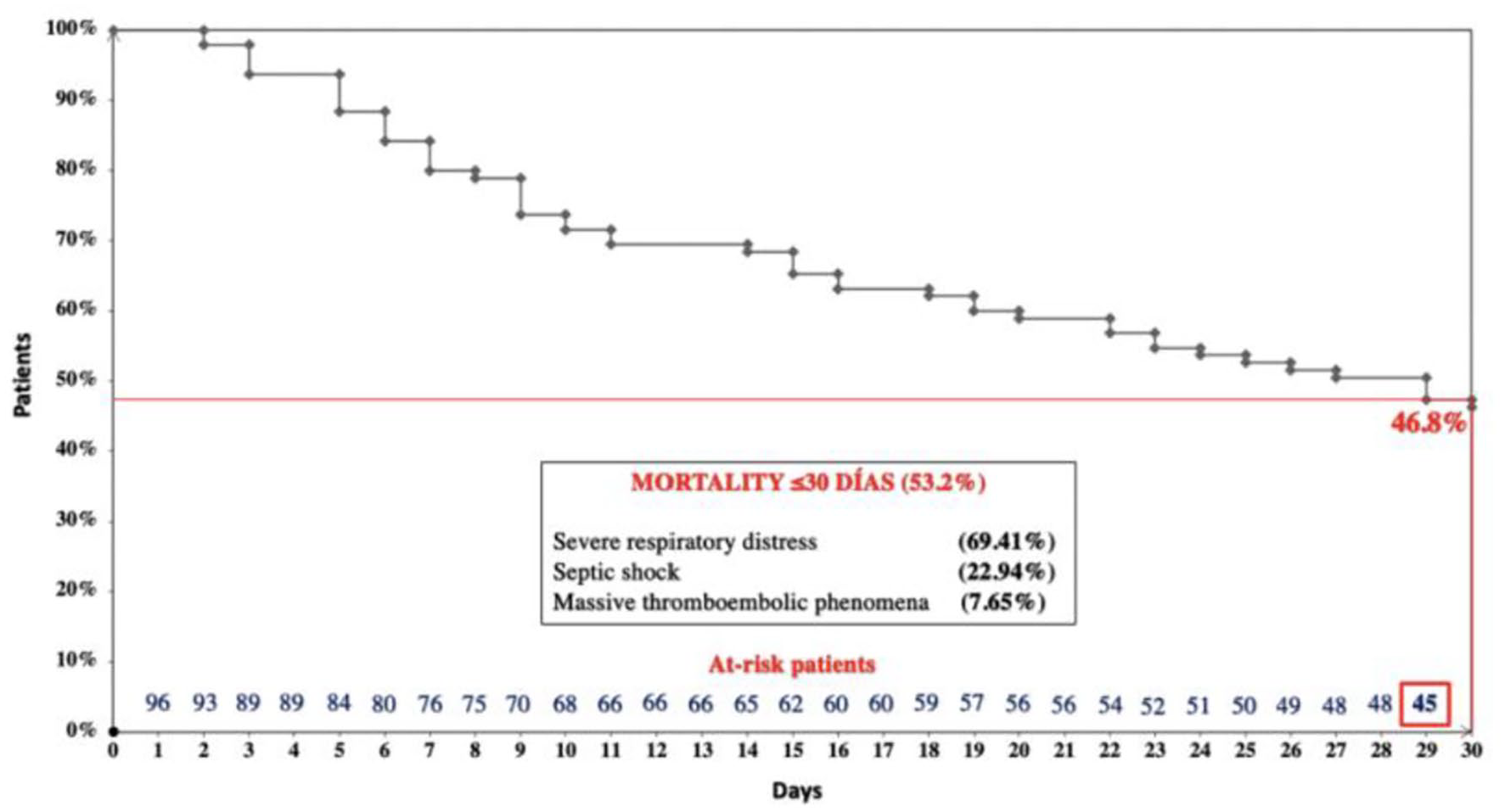
Kaplan-Meier survival curve and 30-day mortality (bottom panel) in patients with COVID-19 and ALLAT.
Poster Number: 32
Abstract Number: 1273679
Elevated circulating endothelial derived extracellular vesicles with periodontal disease
University of Colorado
Background: Periodontal disease (PD) is a progressive multidimensional inflammatory disease of the oral cavity. In addition to adverse oral health consequences, PD is associated with increased risk of cardiovascular disease (CVD), atherosclerotic vascular disease in particular. The direct, and indirect, effects of periodontal disease on vascular function and disease pathogenesis are not completely understood. Clinical interest in circulating extracellular vesicles, particularly endothelial cell-derived microvesicles (EMVs), has intensified due to their involvement in the development and progression of endothelial dysfunction and CVD. The purpose of this study was to determine if circulating EMVs are elevated in adults with periodontal disease, independent of cardiometabolic risk factors.
Methods: Peripheral blood was collected from 24 middle-aged adults: 12 without PD (8 M/4F; age: 50+3 yr) 12 clinically diagnosed with periodontal disease (7 M/5 F; 55+4 yr). All subjects were free of overt cardiovascular and metabolic disease as determined by physical examination, resting ECG and complete blood chemistries. Circulating concentrations of endothelial activation-derived (CD62e+) and apoptosis-derived (CD31+/CD42b−) extracellular vesicles were determined by flow cytometry. Extracellular vesicle size threshold was established using Megamix-Plus SSC calibrator beads and only events < 0.9 μm in size were counted.
Results: There were no significant differences between group in anthropometric, hemodynamic of metabolic risk factors. Circulating concentrations of activation-derived EMVs were not significantly different between the adults without vs with PD (42+7 vs 49+7 EMV/μL). However, apoptosis-derived EMVs were markedly higher (~30%; P< 0.05) in the adults with PD (172+9 vs 134+12 EMV/μL).
Conclusion: Periodontal disease is associated with elevated apoptosis associated EMVs. Apoptosis-derived EMVs are a known biomarker and mediator of endothelial dysfunction and have been linked to atherogenesis. Moreover, elevated CD31+/CD42b− extracellular vesicles are predictive of future CVD risk and events. EMVs may contribute to the vascular disease risk associated with periodontal disease.
Poster Number: 33
Abstract Number: 1269421
Approach to venous leg ulcers- should we determine subtypes?
Eri Fukaya, MD, PhD,
Stanford University
Background: We previously found leg bioimpedance to be a strong predictor for varicose veins using the UK Biobank data. Given these findings, we examined bioimpedance changes in chronic venous disease. Bioimpedance is associated with changes in intravascular volume, tissue water retention and may reflect change in the microcirculation. In our recent study, we found that bioimpedance correlated with increase in CEAP classification and that this may have a role in predicting venous leg ulcer (VLU) onset and healing. We recently separately presented data looking at the characteristics of VLUs at a tertiary wound center and found that patients younger than 60 years old had a greater BMI than those who were older than 60. Given these findings, we sought to analyze in a separate cohort to see if these findings would hold true. We hypothesize that VLUs may present with “subtypes” based on age, BMI, wound chronicity, calf dysfunction and optimal treatment algorithms may differ depending on the subtype.
Methods: Subjects are patients with CEAP C5 and C6 disease from the Stanford Vascular Center from 2020-2021. Data collection includes age, gender, BMI, CEAP and bioimpedance spectroscopy data (L-Dex score). Statistical significance was determined using t-tests.
Results: We acquired data on 24 patients with C5 and C6 disease. The mean age of patients was 64.3 years. The average body mass index (BMI) was 32.7 kg/m2 with age < 60 years being 39.8 kg/m2 and >60 years 30.4 kg/m2 (p< 0.05). Average L-Dex was 14.5 with < 60 years being 10.95 and >60 years 15.6. When looking specifically at patient with C6 disease, average BMI was 32.4 kg/m2 with < 60 years being 41.3 kg/m2 and >60 years 29.8 kg/m2. Average L-Dex was 18.1 with < 60 years being 12.6 and >60 years 19.81.
Conclusion: The data from our cohort suggests differences in VLU characteristics depending on patient age, BMI and bioimpedance. Mechanical factors causing edema may contribute more to VLUs in older individuals, while metabolic variables may be involved in younger patients. Given different presentation of VLUs in different populations, we should define the VLU subtypes and develop treatment strategies that best align with the subgroups.
Poster Number: 34
Abstract Number: 1273647
Influence of chronic spinal cord injury on coagulation and fibrinolytic factors
1University of Colorado, 2Craig Hospital, 3University of Novi Sad, 4University of Split School of Medicine, 5University of British Columbia
Background: The rates of cardiovascular and cerebrovascular disease in adults with spinal cord injury (SCI) range from 30% to more than 50% compared with 5-10% in non-injured adults of similar age. Ischemic heart disease and stroke are the leading causes of morbidity and mortality after the first year of SCI. The mechanisms underlying the heightened risk of atherosclerosis and thrombosis with chronic SCI are not well understood. Disruption in the coagulation-fibrinolytic axis is an important underlying factor in ischemic heart disease and stroke. The aim of this study was to determine the influence of SCI on coagulation and fibrinolytic factors.
Methods: Eighteen young and middle-aged adults were studied: 9 uninjured (7M/2F; age: 40+3 yr) and 9 cervical level spinal cord injured (7M/1F; 51+5 yr). All subjects were normotensive and free of overt cardiovascular and metabolic disease. Plasma coagulation factors (factors VII, VIII and X), fibrinolytic factors (tissue-type plasminogen activator [t-PA] and plasminogen activator inhibitor-1 [PAI-1] antigen and activity) and D-dimer were determined by immunoassay.
Results: Circulating levels of factor VII (69.5±5.2 vs. 69.9±5.3%), factor VIII (87.5±9.4 vs. 106.3±7.1%), and factor X (72.3±2.8 vs. 73.4±4.9%) were not significantly different between uninjured adults and adults with SCI. However, t-PA antigen (8.6±0.4 vs. 3.7±0.7 ng/mL), PAI-1 antigen (12.8±1.4 vs. 5.4±1.1 ng/mL), and PAI-1 activity (0.33±0.06 vs. 0.08±0.02 IU/mL) were markedly higher (~170%; P< 0.05) in SCI compared with uninjured adults. Although, t-PA activity (1.3±0.1 vs. 1.7±0.1 IU/mL) was not significantly different between the groups, the molar concentration ratio of active t-PA to active PAI-1 (1:0.21±0.05 vs. 1:0.06±0.02 mmol/L; P< 0.05), was significantly higher in SCI than uninjured adults, indicating reduced fibrinolytic potential in adults with SCI. Additionally, D-dimer was significantly higher (~55%) in adults with SCI (568.9±57.8 vs. 370.2±53.2 ng/mL).
Conclusion: Collectively, the results indicate a hypofibrinolytic state in adults with chronic SCI. Impaired fibrinolysis may underlie the increased atherothrombotic risk associated with SCI.
Poster Number: 35
Abstract Number: 1275864
Poster Number: 36
Abstract Number: 1273492
Pragmatic implementation science to assess lipid optimization in peripheral artery disease: design and conduct of the randomized optimize PAD-1 trial
1University of Colorado School of Medicine, 2Endpoint and Specialty Services, 3Harvard Medical School
Background: Underutilization of proven therapies in peripheral artery disease (PAD) remains a critical problem. Implementation science aims to improve this, but few trials exist. We describe a randomized trial designed with pragmatic elements in PAD patients.
Methods: OPTIMIZE PAD-1 was designed to evaluate the efficacy of a multidisciplinary vascular care team using an intensive lipid reduction program in PAD patients versus usual care. The primary endpoint is low density lipoprotein-cholesterol (LDL-C) reduction at 12 months. A second objective is to assess the impact of a structured quality assurance program (EQuIP) on variability in 6-minute walk test (6MWT) distance. Due to COVID-19, pragmatic aspects were introduced, including virtual consent/recruitment, home-based subject conducted lab testing, and virtually monitored home-based 6MWT.
Results: A total of 114 subjects with PAD were recruited over ~18 months at the University of Colorado and randomized to algorithm-driven lipid management by a multidisciplinary vascular care team with pharmacist support or to usual care (Figure). Subjects were also randomized to 6MWT conducted by site versus EQuIP staff. Potential participants and clinical events during follow up were identified via electronic medical records. Adjustments to enable remote study conduct were successfully implemented.
Conclusion: Pragmatic randomized trials in PAD patients are feasible to strengthen implementation science.
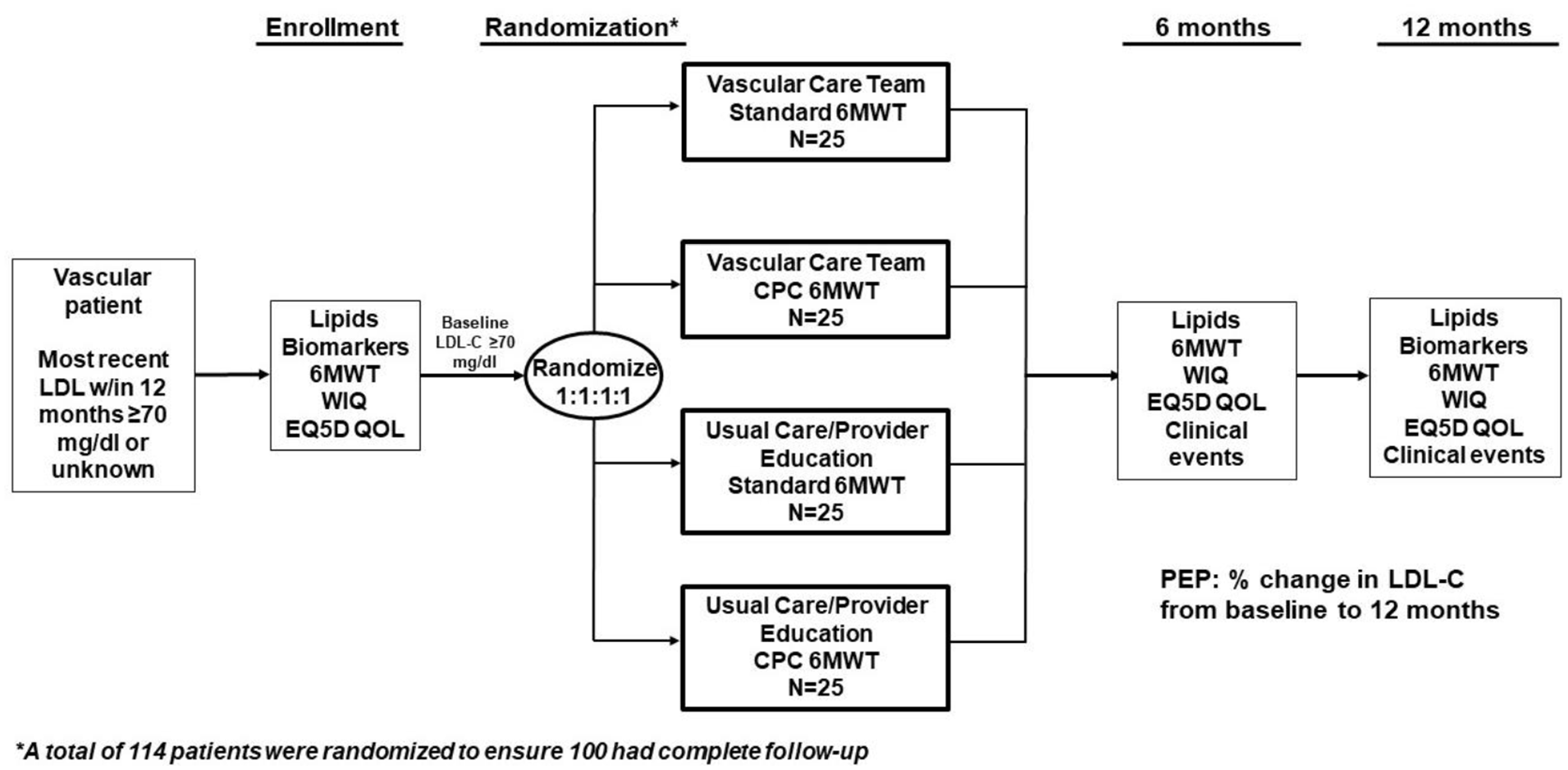
OPTIMIZE PAD-1 Study Design.
Poster Number: 37
Abstract Number: 1273820
Outcomes of large arterial vessel thrombosis in the setting of COVID-19
Staten Island University Hospital-Northwell
Background: COVID-19 infection can cause an array of symptoms including arterial thrombosis with an incidence of 4.4% however isolated large vessel thrombosis is even rarer. We present a review of the literature regarding large vessel (Iliac and aortic) thrombosis associated with COVID-19 infection and discuss the outcomes. In addition, we present a case that was infected with COVID-19 with presentation of isolated aortic thrombosis.
Methods: We performed a literature review using Pubmed keywords, “COVID-19”, “iliac,” “aortoiliac,” “aorta,” “thrombosis”. The articles were then narrowed to the ones only pertaining to aortic (AT) or iliac thrombosis (IT) with COVID-19 infection.
Results: Our literature review found 12 articles detailing a total of 14 cases of AT or IT in the setting of COVID-19 infection. Ages ranged from neonate to 85 years old. Incidence of smoking was 30% and diabetes was 25%. Mortality rate was noted to be 14% (2 out of 14 patients). Approximately, 50% (7 out of 14) of the patients were treated with surgery and 21% (3 out of 14) received anticoagulation. 64%, (9 out of 14) of the patients presented with symptoms of acute limb ischemia. Amputation rate was noted to be 7% (1 out of 14).
Conclusion: Large vessel thrombosis caused by COVID-19 infections seems to carry high mortality and amputation rates. To prevent devastating sequel of COVID infection with concurrent large arterial thrombosis we emphasize that physicians employ a high index of suspicion and urgent involvement of the vascular interventionists. The case that we presented emphasized the importance of understanding the effect of COVID-19.
Poster Number: 38
Abstract Number: 1273413
Neutrophil-to-lymphocyte ratio as a predictor of deep venous thrombosis in adults who underwent venous duplex studies: An analytical cross-sectional study at a tertiary referral center
St. Luke’s Medical Center Global City
Background: Thrombotic disorders are pro-inflammatory as much as they are hemostatic. The neutrophil-to-lymphocyte ratio (NLR) has been established as a marker of subclinical inflammation. NLR has not yet been established as a predictive marker of deep vein thrombosis (DVT). The study aims to determine the association of NLR and the presence of acute or subacute, lower extremity DVT among adult patients.
Methods: This was an analytical cross-sectional study utilizing chart review which included adult patients who underwent venous duplex study from July 2015 to December 2020 in a tertiary medical center. NLR was calculated based on a complete blood count (CBC) done within 24 hours of the venous duplex scan. NLR values of > 1.76 was considered positive for DVT based on related literature.
Results: There were 478 patients included in the study, of whom 140 (29%) were detected with DVT, 81 acute and 59 subacute, on venous duplex. The group with DVT had significantly higher neutrophil-to-lymphocyte ratios (median 2.65 [range 0.8–97]) compared to patients without DVT (median 2.2 [range 0.7–45]). Receiver-operating characteristic analysis yielded an AUC of 0.6068. The optimal cutoff of NLR for predicting DVT was ⩾ 2.1. This proposed cutoff value yielded a sensitivity of 72.86%, specificity of 46.50%, and overall diagnostic accuracy of 53.97%.
Conclusion: This cross-sectional study showed that NLR > 2.1 is associated with acute to subacute DVT among patients who does not have comorbidities or conditions that may affect the inflammatory parameters. Although NLR cannot replace venous duplex scan in diagnosing DVT, it can be used to screen DVT. This is a cheaper and more widely available test to use compared to D-dimer. Further investigating these parameters may be worthy as they have the potential to be an alternative, readily available and affordable diagnostic test.
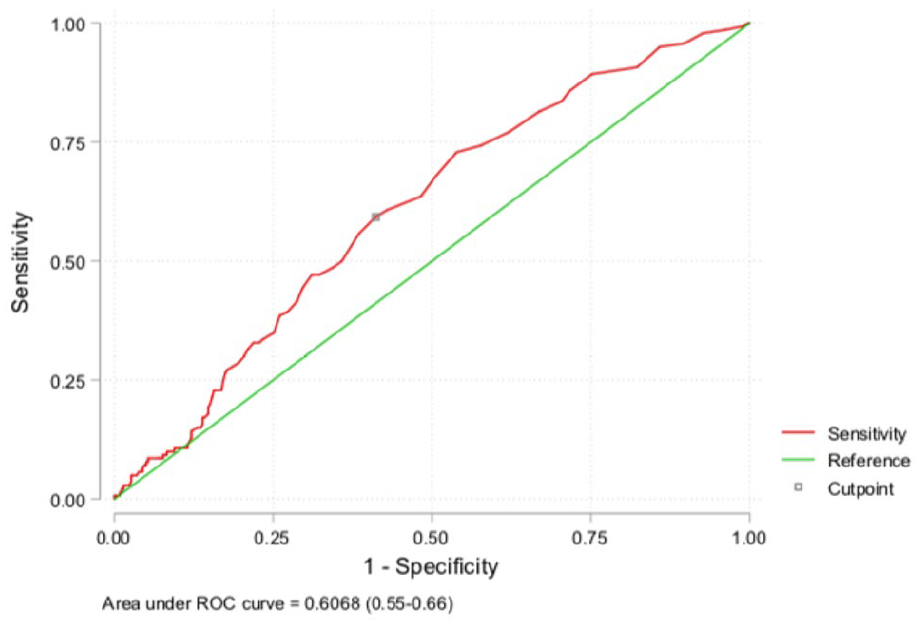
ROC curve of NLR for diagnosing DVT.

Association of NLR and DVT
Poster Number: 39
Abstract Number: 1271662
Therapeutic angiogenesis with implantation of hypoxia-induced mesenchymal stem cell
Hiroshima University
Background: Patients with chronic threatening limb ischemia have a significant risk of amputation. Therapeutic angiogenesis facilitating microvascular and surrounding tissue regeneration through angiogenic approaches, including cell therapy and gene therapy, has been investigated in preclinical models and in clinical trials. Hypoxia preconditioning enhances the abilities of mesenchymal stem cells (MSCs) for vascular regeneration. Implantation of hypoxia-induced mesenchymal stem cells (hi-MSCs) into ischemic muscle may further improve limb perfusion.
Methods: MSCs, hi-MSCs and phosphate-buffered saline (PBS) were intramuscularly implanted into ischemic hindlimb model. Restoration of blood flow and muscle perfusion was evaluated by laser Doppler perfusion imaging. Immunochemistry of hypoxia-inducible factor-1 alpha and vascular endothelial growth factor A were analyzed. In-vitro analysis of MSCs and hi-MSCs with endothelial cell-inducing medium showing expression levels of vascular endothelial growth factor, platelet endothelial cell adhesion molecule-1, and von Willebrand factor were performed.
Results: Blood perfusion recovery with enhanced vessel densities of ischemia limb were greater in hi-MSC group than in MSC or PBS group. Immunochemistry revealed that hi-MSCs had higher expression levels of hypoxia-inducible factor-1 alpha and vascular endothelial growth factor A than those in MSCs. With endothelial cell-inducing medium, hi-MSCs showed higher expression levels of vascular endothelial growth factor, platelet endothelial cell adhesion molecule-1, and von Willebrand factor compared to MSCs.
Conclusion: Implantation of hi-MSCs promotes neovascularization with the presence of higher expression levels of angiogenic cytokines including HIF-1α and VEGF. Future studies are needed to determine the role of hi-MSCs in therapeutic angiogenesis in order to confirm the efficacy, safety, and feasibility for clinical practice.

Serial laser doppler perfusion image (LDPI) studies after surgical induction of ischemia in PBS, MSC and hi-MSC implantations groups.
Poster Number: 40
Abstract Number: 1279181
Vasomotor dysfunction in complex regional pain syndrome responds to prostacyclin
Brigham and Women’s Hospital
Background: Complex regional pain syndrome (CRPS) represents a heterogenous grouping of phenotypes; a subgroup of these patients exhibit pronounced vasomotor instability. The underlying pathobiology leading to vascular dysfunction and the role of vascular-directed therapies are poorly understood.
Methods: Three patients were evaluated for leg pain with prominent intermittent cyanosis and coolness. All patients had a prior history of palliative below-knee amputation (BKA) in the contralateral lower extremity due to CRPS 1-3 years prior to presentation. Response to vasomotor-directed therapies was assessed through clinical exam and patient-reported symptoms.
Results: Patient 1 was a 22-year-old woman with a history of left BKA. Patient 2 was a 35-year-old woman with a history of right BKA. Patient 3 was a 52-year-old woman with a history of left BKA. Vasomotor changes at the time of presentation included dependent cyanosis, intermittent erythromelalgia, and coolness of the extremity. Peripheral angiogram in all patients showed no flow-limiting lesion but did demonstrate very slow filling of the distal vessels of the affected extremity, suggestive of microvascular dysfunction. All patients were initially started on doxazosin and a PDE5 inhibitor (either sildenafil or tadalafil) in a stepwise manner. After 3 months all patients reported improvement in vasomotor symptom burden, including decreased color change, improved temperature regulation, and decreased discomfort. After 1 year, patient 3 required BKA revision which resulted in poor wound healing and worsened vasomotor changes. This was unresponsive to further titration of oral vasodilators. She was trialed on a 5-day infusion of low-dose epoprostenol (up to 7 ng/kg/min) with dramatic improvement in wound healing. Patients 1 and 2 each subsequently also developed worsening vasomotor changes which was unresponsive to oral vasodilator augmentation but did respond to epoprostenol infusion.
Conclusion: CRPS can be associated with peripheral small vessel outflow obstruction. Vascular-directed interventions can improve vasomotor symptoms, and epoprostenol appears to demonstrate enhanced efficacy over oral vasodilator options.
Poster Number: 41
Abstract Number: 1279193
Clinical and imaging phenotypes from a registry of segmental arterial mediolysis (SAM)
1Brigham and Women’s Hospital, 2Vanderbilt University
Background: Segmental arterial mediolysis (SAM) is a non-inflammatory arteriopathy whose clinical characteristics and natural history remain poorly defined.
Methods: A retrospective, single-institution review of 31 patients presenting with arterial dissection, intramural hematoma, aneurysm, or occlusion between 2015 and 2021 was performed. To establish a non-invasive diagnosis of SAM, patients with FMD, inflammatory, or genetic arteriopathy were excluded by clinical, laboratory, and imaging criteria according to multidisciplinary guidelines. Patient demographics, clinical features, imaging findings, and management were assessed.
Results: The average age of patients was 54 years; 23% were female and 78% were male. Hypertension was present in 39% of patients and 6% had a pre-existing history of ischemic heart disease; 48% were current or prior smokers. In patients without diagnosed CAD, the 10-year ASCVD risk score was 8.3%. The average hemoglobin A1c was 5.7%. Acute onset abdominal pain (94%) was the most frequent presenting symptom. On average, two vessels were affected at the time of diagnosis, most often in the abdomen. Arterial dissection was present in 90% of patients, and intramural hematoma was seen in 26% of cases. The most affected vessel was the celiac artery (58%), followed by the superior mesenteric artery (45%), renal arteries (32%), and iliac arteries (29%) The vertebral and carotid arteries were each involved in < 10% of cases. Over the follow-up duration, all patients survived; three patients required intervention due to worsening clinical symptoms. Anticoagulation was utilized in 71% of cases, most commonly for 1-3 months. Long-term follow-up imaging was available in 24 patients; 9 (38%) had progression in lesion size after the first imaging study. After 1 year, 5 patients continued to show enlargement. All 3 patients requiring intervention showed enlargement in their lesion size on initial repeat imaging.
Conclusion: SAM demonstrates a male predominance, typically manifesting in middle-aged patients with low to intermediate cardiovascular risk. A subset of patients shows growth in size of the affected vascular segment, and this may be a risk factor to identify those needing future intervention.
Poster Number: 42
Abstract Number: 1272078
Institutional complications of arteriovenous fistulas in 2017: A retrospective review
SUNY Downstate Health Sciences University
Background: Arteriovenous fistulas (AVF) are a type of permanent vascular access available for hemodialysis. Although AVFs are preferred over other vascular modalities due to decreased long term vascular events, hemodialysis patients with AVFs still present with complications including mechanical, infectious, and vascular. Studies analyzing the complication rates of AVF are limited. Therefore, the purpose of the study is to assess the frequency and characteristics of complications of AVF present at our institution.
Methods: Charts of 356 hemodialysis patients at our institution were reviewed. 109 patients who had an AVF created in 2017 were studied. Patients were divided into complications and no complications groups. In addition to baseline demographics, outcome variables studied were complications (mechanical, infectious, and vascular). Complication rates, complication type, and average time a patient returned for revision surgery following AVF creation were determined.
Results: Of the 356 patients studied, 109 patients (30.6%) met inclusion criteria whereas 247 patients (69.4%) did not. Exclusion criteria included patients who were < 18 years old and patients who had an AVF created before 2017. 74 patients (67.9%) had at least one complication following AVF creation while 35 patients (32.1%) had no complications. Patient demographics were similar between patients with and without complications. Complications of AVF included stenosis, thrombosis, infection, malfunctioning AVF, failure of maturation, and hematoma. A patient returned for a revision procedure on average 2.28 times.
Conclusion: Our results demonstrate that surgery for AVF is associated with a high rate of complications in our institution for patients who had an AVF created in 2017. Complications with the greatest incidence included stenosis, malfunctioning AVF, and thrombosis. Knowledge about the specific complications endemic to our population might prevent serious morbidity and fatal outcomes.

Baseline demographics of patients who had an AVF created in 2017.
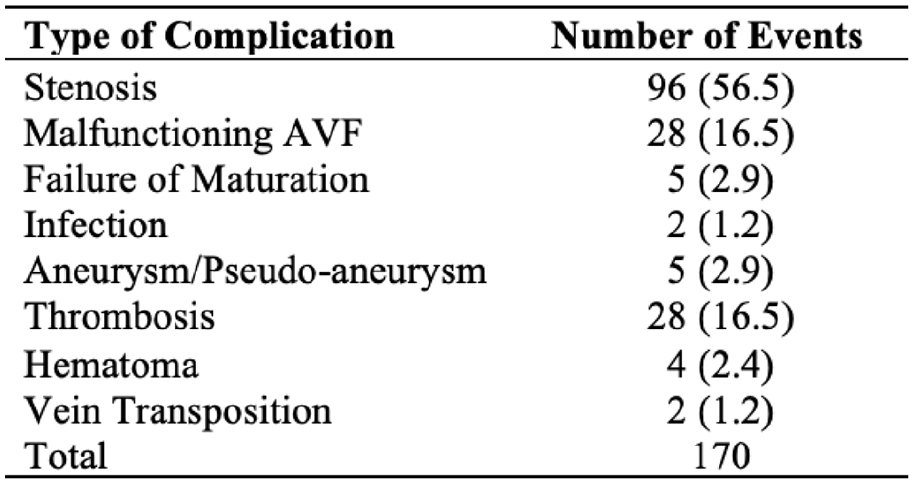
Complications.
Poster Number: 43
Abstract Number: 1278831
Optimal medical therapy in peripheral artery disease patients referred to a limb preservation program is poor
1Harvard Medical School, 2Massachusetts General Hospital
Background: Optimal medical therapy (OMT) has been substandard in peripheral artery disease (PAD) compared to coronary artery disease (CAD). We evaluated prevalence of OMT in PAD patients referred to a limb evaluation and preservation program (LEAPP).
Methods: LEAPP is a multidisciplinary program at Massachusetts General Hospital focusing on limb salvage for PAD. Patients are commonly referred by their primary care physicians but can be recruited by any other source. We collected information on risk-factors and reviewed existing treatments at the time of referral from electronic medical records.
Results: Of 82 patients referred to LEAPP from November 2021 to May 2022, 64% were men and 88% were European Americans. Mean age at referral was 69 years. A total of 76% had diabetes, 90% had hypertension, 91% had dyslipidemia, 77% were ever smokers, 82% were receiving antiplatelet therapy, 67% were receiving high-intensity statin, 73% were receiving angiotensin converting enzyme inhibitor or angiotensin II receptor blocker, 1% were receiving cilostazol, and 4% had already been referred for supervised exercise therapy. Patients with concomitant CAD received high rates of OMT, compared to without CAD (Table).
Conclusion: Despite clear evidence of limb and lifesaving benefits of OMT in PAD patients and despite multiple nationalized efforts to increase awareness and prevalence of OMT, the actual guideline concordance remains poor. The impact of a systemwide, multidisciplinary, limb evaluation and preservation program on OMT is yet to be seen.

OMT in PAD patients with or without concomitant CAD.
Poster Number: 44
Abstract Number: 1273315
Innovations in the vascular medicine fellowship training model featuring virtual inter-institutional cohort learning
1Boston University School of Medicine, 2Anticoagulation Forum
Background: Vascular diseases are common and remain undertreated. Many vascular medicine (VM) training programs include only one fellow, leading to a need for models to facilitate cross-institutional learning.
Methods: We designed and implemented a multi-institutional learning consortium to augment career development of trainees participating in the Anticoagulation Forum|Ansell VM Fellowship Program. The pedagogical model included a virtual curriculum focused on both clinical knowledge and career development. We evaluated outcomes via mixed method surveys.
Results: We report the interim findings involving 9 institutions (3 for both years 1 and 2/6 either year 1 or 2) and 12 fellows. The educational model includes on-site clinical training, along with inter-institutional cohort learning delivered through biweekly virtual seminars. Seminar topics include: core VM clinical areas with cases (75%), professional development (15%), and research skills (10%). All fellows reported agreement that the seminar series provided networking opportunities and improved understanding of VM. The year 1 cohort (2020-2021) was neutral about the program’s efficacy in promoting connections between co-fellows. In response to this feedback, we added pre-work before each session for the year 2 cohort (2021-2022), which was completed by fellows in rotating pairs. This change resulted in all year 2 fellows reporting agreement that the program “helps form a connection with other fellows.” Themes of open responses included connection with faculty across multiple institutions, mentoring, and connection with co-fellows.
Conclusion: The inter-institutional fellowship model represents an innovative educational approach that facilitates virtual training and mentoring through a structured, multi-component seminar series. The program elements may be scalable across a larger group of VM fellowships.
Poster Number: 45
Abstract Number: 1273807
Increasing access, quality, and convenience of care through a specialty-matched telenursing platform for vascular and wound patients - a pilot study
1PocketRN, 2Stanford School of Medicine
Background: A 2021 survey found that 22% of the nursing workforce may leave their current positions in the next year due to factors such as insufficient staffing, workload, and the emotional toll. This nurse staffing crisis demands innovative solutions to nursing care. Nurses can be an excellent resource for patient education and clinical triage but are rarely utilized outside of in-person roles for vascular and wound patients. This pilot implements a Telenursing Platform (TP) that matches patients on-demand to nurses via video visit based on specialty area to access from their home.
Methods: We conducted a 9-month pilot study with 64 patients and 20 nurses to look at feasibility, adoption, acceptability, and clinical appropriateness of the TP based on qualitative interviews and surveys of both patients and nurses who used the platform, quantitative data on the number, duration, type, and result of each video visit compared to baseline call statistics, and chart review. The TP provided patients with access to RNs including after-hours staffed by specialty and generalist nurses working from home. TP visits included both RN initiated follow up visits and patient-initiated visits for urgent needs.
Results: Based on 20 interviews (11 patient, 9 nurses) and 128 video visits, nurses perceived TP to be a valuable platform for patient questions, reinforce education, and transmit information to caregivers. Access to a knowledgeable party reduced patient distress and patients were more comfortable in their home compared to clinic to receive information on their care. Patient noted using the TP to resolve concerns without going to the emergency department. Nurses also reported that the TP enables higher quality of care compared to phone calls. The main barrier to access for patients was the lack of comfort with technology.
Conclusion: Early results suggest that utilizing nurses in a new care model via a TP for vascular and wound care is feasible, acceptable, and clinically appropriate based on the qualitative interviews analyzed using thematic network analysis, surveys noting >90% acceptability, and visit results noting clinically appropriate care upon chart review. Adoption, however, requires up front human resources to train patients with the technology.
Poster Number: 46
Abstract Number: 1273811
Poster Number: 47
Abstract Number: 1267916
Clinical significance of right heart thrombus with and without an underlying pulmonary embolism
1Harvard Medical School, 2Massachusetts General Hospital, 3Prisma Health - University of South Carolina School of Medicine, 4Beth Israel Deaconess Medical Center, 5Columbia University
Background: Right heart thrombus (RHT) is a rare but serious form of venous thromboembolic disease that may be associated with pulmonary embolism (PE). Studies have demonstrated that RHT denotes worse survival in those also with an acute PE. However, the prognosis of patients with RHT presenting without an underlying PE remains ill-defined.
Methods: We conducted a multicenter observational cohort study to compare patients presenting to our institutions with RHT with and without an underlying PE. The primary endpoint was 90-day all-cause mortality. We utilized multivariable regression to compare outcomes in RHT patients with and without a PE.
Results: Of 455 patients with RHT, 66 (14.5%) had a PE at admission. The average age of the cohort was 62.2±19.3, 47.3% were female, and 22.2% had active malignancy. Patients with PE were more likely to present with dyspnea (50.0% vs. 30.1%, p< 0.01), syncope (15.2% vs. 3.6%, p< 0.01), and persistent hypotension (27.3% vs. 13.1%, p< 0.01) while patients without PE were more likely to be asymptomatic (21.9% vs. 7.6%, p=0.01). Advanced therapy was more often utilized in patients with versus without PE (36.4% vs. 9.5%, p< 0.01). PE in the setting of a RHT was associated with an increased hazard of 90-day mortality (HR 2.06, 95% CI 1.21-3.52, p< 0.01; Figure). Additionally, these patients had a higher risk of in-hospital mortality (OR 2.73, 95% CI 1.18-6.09, p< 0.01) and admission to the ICU (OR 6.03, 95% CI 3.10-12.27, p=0.02).
Conclusion: Patients presenting with RHT and an associated PE had a more severe clinical presentation, required more advanced therapies, had more ICU admissions, and had reduced survival compared to those without a concomitant PE. RHT in the setting of acute PE represents a unique clinical entity which is associated with a worse prognosis versus patients with only RHT.

Kaplan-Meier curves for 90-day all-cause survival analysis comparing patients with a right heart thrombus with and without an underlying PE (Log-rank: p < 0.01).
Poster Number: 48
Abstract Number: 1271812
Functional and quality of life outcomes after treating pulmonary embolism with mechanical aspiration thrombectomy with lightning 12: interim analysis of the strike-PE study
1Massachusetts General Hospital, 2Harvard Medical School, 3David Geffen School of Medicine at UCLA, 4Miami Cardiac & Vascular Institute, 5Sentara Vascular Specialists, 6Thomas Jefferson University Hospital
Background: Little is known about functional and quality of life outcomes after treatment of pulmonary embolism (PE).
Methods: STRIKE-PE is a prospective, multicenter study of adult patients with clinical signs and symptoms of acute PE and a right ventricle/left ventricle (RV/LV) ratio of 0.9 or greater who receive frontline endovascular treatment with Lightning 12. Functional (6-minute walk test, Borg scale, and NYHA Class) and quality of life (Pulmonary Embolism Quality of Life [PEmb-QoL] Questionnaire and EQ-5D-5L) outcomes were collected at baseline or discharge and at 90 days. This study will enroll approximately 600 patients who will be followed up to 365 days.
Results: This interim analysis includes 48 patients enrolled in 15 sites (Table). The PE category was submassive in 93.6% of patients and massive in 6.4% of patients. The distance covered by the 6-minute walk test increased by 112 meters from discharge to 90 days (P < .001). At 90 days, the median Borg scale at rest was 0 (no dyspnea), a decrease of 4 points (P < .001), and the NYHA Class was I in 90% of patients. The overall PEmb-QoL Questionnaire score improved (decreased) by 16.2 points from discharge to 90 days (P =.015). The EQ-5D-5L Visual Analog Scale score improved (increased) by 10 points from baseline to 90 days (P =.004).
Conclusion: Patients with acute intermediate-risk and high-risk PE appeared to experience improved functional outcomes and quality of life at 90 days after mechanical aspiration thrombectomy with Lightning 12.

Functional and quality of life outcomes after treating PE with mechanical aspiration thromboectomy with Lightning 12. Data are presented as mean (SD), median [IQR], or percent (n/N).
Poster Number: 49
Abstract Number: 1273842
The relationship of fasting triglycerides and non-fasting triglycerides concentrations in abdominal aortic calcification: An insight from NHANES
Harvard Medical School-Massachusetts General Hospital
Background: Abdominal aortic calcification (AAC) has been known as a risk factor for cardiovascular disease due to its common pathophysiological pathways with coronary artery disease. Additionally, increasing evidence suggests that arterial calcifications increased the risk for cardiovascular diseases.
Methods: We analyzed the data of patients with calcification in their abdominal aorta from the National Health and Nutrition Examination Survey (NHANES) 2013–2014. Dual-energy X-ray absorptiometry (DXA scans) were obtained and samples with completed DXA scans were included. We collected 3140 samples and validated the images in a 24-point method (ACC-24). We carried out binary logistic regression to examine the association between demographic characteristics (age, sex, educational level, and income), risk factors for cardiovascular diseases (LDL-C, HDL-C, triglycerides (fasting and non-fasting), body mass index, systolic blood pressure, diabetes, and smoking status), ongoing medications (antihypertensives, statins, and anti-platelets), and AAC status (patients with a score ⩾2 on the AAC-24 were considered AAC positive). For analysis purposes, abnormal distribution were categorized.
Results: Individuals with positive AAC were found to be older compared to negative AAC (mean age of 65.5 ± SD 11.7 versus 56.1±11.1 years). Positive AAC was also associated with higher systolic blood pressure (131.3±19.5 vs 125.8±18.4 mmHg), and higher BMI (28.7±5.8 vs 27.6±4.8 kg/m2). We found a strong relationship between positive AAC and plasma triglyceride concentration. Univariate analysis found that the risk of developing AAC was twice as high in groups with measured fasting triglycerides higher than the first quartile, compared to those in the first quartile. The relationship persisted when the analysis was adjusted for demographic characteristics, cardiovascular risk factors, and ongoing medications. An analogous pattern was also seen with non-fasting triglycerides.
Conclusion: We found a strong relationship between AAC and plasma triglyceride concentration. Further study is essential to determine the validity of this finding in external cohorts, and whether triglycerides reduction poses an effect to the progression of AAC.
Poster Number: 50
Abstract Number: 1273724
Pyoderma gangrenosum and venous ulcers: A case series of potential masquerade and a culprit for delay in diagnosis
1University of Maryland Medical Center-Midtown, 2St. Georgie’s University, 3University of Maryland
Background: Delayed venous ulcer (VU) healing could be multifactorial including other comorbid conditions such as pyoderma gangrenosum (PG). PG, an uncommon yet highly destructive inflammatory condition, could be easily misdiagnosed as a venous ulcer due to similarities in presentation. The purpose of this review is to highlight a series of 5 cases with PG and to show healing rate after appropriate diagnosis and management.
Methods: This is a retrospective review of cases of venous ulcers that were later diagnosed as PG at the wound center over 30 months.
Results: All patients were diagnosed with venous ulcers and treated with high degree compression and standard wound care. 80% of wounds increased in size from initial presentation after standard therapy with mean healing rate of -80.2% (SD ±85) raising suspicion for pathergy. Skin biopsies were obtained due to poor healing which showed clinicopathologic evidence for PG. Percent of healing and mean healing rate after appropriate treatment for PG with corticosteroids and immunomodulators at 1 month (mean 58.95% with SD ± 20.5), 3 months (mean 79.4% with SD ± 8.5), and 6 months (mean 96.1% with SD ±0.2) are noted in the Figure.
Conclusions: PG should be considered as an alternative diagnosis in non-healing venous wounds. PG can present overlying areas of CVI which can complicate clinical diagnosis. Misdiagnosis of PG can lead to delay in treatment and complications including severe pathergy reaction from inappropriate management. Although an overwhelming majority of lower extremity ulcers are due to venous causes, it is important to consider alternative diagnoses and obtain further workup including skin biopsy in patient with persistent non-healing ulcers to rule out less common etiologies. Finally, immunosuppression may have a role in some non-healing ulcers.
