
Abstract
Background:
Circulating angiogenic cells (CACs) are indicative of vascular health and repair capacity; however, their relationship with chronic e-cigarette use is unclear. This study aims to assess the association between e-cigarette use and CAC levels.
Methods:
We analyzed CAC levels in 324 healthy participants aged 21–45 years from the cross-sectional Cardiovascular Injury due to Tobacco Use study in four groups: never tobacco users (n = 65), sole e-cigarette users (n = 19), sole combustible cigarette users (n = 212), and dual users (n = 28). A total of 15 CAC subpopulations with four cell surface markers were measured using flow cytometry: CD146 (endothelial), CD34 (stem), CD45 (leukocyte), and AC133 (early progenitor/stem). Generalized linear models with gamma distribution and log-link were generated to assess association between CACs and smoking status. Benjamini-Hochberg were used to adjust p-values for multiple comparisons.
Results:
The cohort was 47% female, 51% Black/African American, with a mean (± SD) age of 31 ± 7 years. Sole cigarette use was significantly associated with higher levels of two endothelial marker CACs (Q ⩽ 0.05). Dual users had higher levels of four endothelial marker CACs and one early progenitor/stem marker CAC (Q ⩽ 0.05). Sole e-cigarette users had higher levels of one endothelial and one leukocyte marker CAC (Q ⩽ 0.05).
Conclusion:
Dual use of e-cigarettes and combustible cigarettes was associated with higher levels of endothelial origin CACs, indicative of vascular injury. Sole use of e-cigarettes was associated with higher endothelial and inflammatory CACs, suggesting ongoing systemic injury. Distinct patterns of changes in CAC subpopulations suggest that CACs may be informative biomarkers of changes in vascular health due to tobacco product use.
Introduction
Tobacco smoking is a major risk factor for cardiovascular disease (CVD). 1 The association between tobacco use and CVD is well known. However, studies focusing on the effect of tobacco on vascular function, and more specifically vascular self-repair in electronic cigarette (e-cigarette) users, is sparse. The use of e-cigarettes is rising globally, even among tobacco naïve individuals, and a quantification of their effect on key metrics of cardiovascular health are urgently needed.2–4 Thus, rigorous empirical methodology is needed to elucidate the effect of e-cigarette use on vascular health.
Vascular health is a complex phenomenon. A heterogeneous progenitor cell population known as circulating angiogenic cells (CACs), previously called endothelial progenitor cells, with distinct surface markers (endothelial, stem, late/early progenitor, or leukocytic) contribute to vascular repair.5,6 Although CACs are categorized by their lineage of origin, the presence of surface markers depicting these origins are associated with corresponding vascular functions including endothelial development, angiogenesis, and a pro-inflammatory state.7,8 CACs mobilize from the bone marrow in undifferentiated form and reside in multiple tissues including circulating blood.9,10 Arterial wall CACs persist in a dormant state until the time of their activation triggered by vascular insult.11,12 Following vascular damage, CACs participate in endothelial regeneration by homing to the sites of such damage. 6 CACs have been found to aid in endothelial repair postinjury and are measurable in peripheral blood, which makes them promising markers of vascular health.13,14 CACs have been associated with CVD risk factors and circulating levels of CACs have been found to be predictive of CV events.15,16
Combustible cigarette smoking has been shown to have an association with CAC levels in healthy people.17–19 Further, previous studies have found that acute smoking leads to increased CAC levels, whereas chronic smoking leads to decreased CAC levels in peripheral blood.20,21 However, little is known about the relationship between e-cigarette use and CAC levels.
Accordingly, in this study, we sought to examine the association between e-cigarette use and CACs, which could be a biomarker of vascular health. We hypothesize that in comparison with never tobacco users, current e-cigarette use is associated with altered CAC levels. The primary objective of this study is to compare CAC levels in sole e-cigarette users versus those in dual users and in never tobacco users. The secondary objective is to compare CAC levels in sole e-cigarette users and sole combustible cigarette users.
Methods
Study design
The Cardiovascular Injury due to Tobacco Use (CITU) study is a cross-sectional observational study to evaluate the cardiovascular effects of conventional and new and emerging tobacco products. The study design was published previously.22,23 Briefly, healthy male and female participants between the ages of 21 and 45 years were recruited from Boston University (Boston, MA) and University of Louisville (Louisville, KY) for a 2-hour in-person visit that consisted of a physical exam, vascular testing, and surveys about their lifestyle and habits including tobacco use. Participants were identified via broad recruitment strategies including flyers, social media postings, presentations, etc. Prior to study visits, study staff screened all participants for Inclusion/Exclusion (I/E) criteria as well as what type of tobacco products were used (Table S1 in the online supplementary material). I/E were reviewed at the beginning of the study visit in addition to CO measures to identify baseline levels of CO that would disqualify the participant as unfasted (typically around 10 ± 2 ppm but based on total cigarettes per day and predicted 24-hour fast). Biospecimens were collected from all participants after a 6-hour fast from any tobacco products. Participants were never or current users of tobacco products without established CVD risk factors. All participants provided written informed consent, and all study protocols were approved by the University of Louisville and Boston University institutional review boards (IRB # 12.0590 and H-32613, respectively).
Study participants
Tobacco use categories were defined by self-report and refined by urinary cotinine levels as detailed in Table S1 (online). Participants were classified as never tobacco users if they had smoked fewer than 100 cigarettes in their lifetime, were not current smokers or users of other tobacco products, and had a urinary cotinine level less than 10 ng/mL. Sole e-cigarette users were defined as participants who currently use e-cigarettes at least 5 days per week and have not used combustible cigarettes for ⩾ 3 months. Combustible cigarette smokers were defined based on current smoking of at least 5 days per week, having smoked ⩾ 100 cigarettes in their lifetime, and no current e-cigarette use for ⩾ 3 months. Dual combustible and e-cigarette users were defined as participants who reported current use of both combustible and e-cigarettes, at least 5 days per week, with a lifetime usage of ⩾ 100 cigarettes. I/E criteria are further detailed in Table S1 (available online).
Circulating angiogenic cells
Different subpopulations of CACs were measured in the peripheral blood using a seven-color flow cytometry procedure on fresh blood specimens as previously described.14,24 Briefly, fresh venipuncture blood was collected in a 10 mL BD vacutainer (BD, Franklin Lakes, NJ, USA) mononuclear cell preparation tube, which was spun at 1600 g for 30 minutes at room temperature. The tube was stored in an upright position for 24 hours postspinning, after which it was processed and analyzed under a standardized operating protocol at the University of Louisville.
CACs were measured by flow cytometry as previously described.14,24,25 Briefly, CACs were defined as CD14 negative cells and differentiated into 15 subtypes based on positive, negative, or low (dim) marker expression of CD45 (leukocytic), CD34 (stem), CD146 (endothelial), or AC133 (early progenitor) surface markers. Individual CACs and their surface marker phenotypes are detailed in Table S2 (available online).
Statistical analysis
The primary objective of this study was to compare CAC levels in sole and dual users with never tobacco users. The secondary objective was to compare CAC levels between sole e-cigarette versus sole combustible cigarette users. Participant characteristics are expressed as mean with SD for continuous variables, and percentages for categorical variables. Comparison of clinical characteristics was performed with one-way ANOVA for continuous variables and with Pearson’s chi-squared or Fisher’s exact tests for categorical variables. In CAC subgroups with values below the limit of detection (LOD), values were computed by dividing the lowest measurable value by two.
Because CAC measurements were positive, and heavily right-skewed, generalized linear models (GLM) with gamma distribution and log-link were generated to examine the association between CACs and smoking status. For parameter estimation, we performed a sensitivity analysis between Fisher and hybrid methods. In the Hybrid method, Fisher scoring iterations were performed before switching to the Newton-Raphson method. We found no significant difference between these two methods and therefore used the hybrid method for all parameter estimations. The models were adjusted for: age, sex, race, ethnicity, and site of enrollment. Interactions between adjustments and log CAC levels were tested. To account for multiple comparisons, the Benjamini-Hochberg correction was set at a false discovery rate (FDR) of 25%. 26
Statistical significance was assessed at alpha less than or equal to 0.05. A two-sided post hoc power calculation for a sample size of 324 participants yielded an 88% power using an ANCOVA fixed effects model with an expected medium effect size of 0.25 SD units and an alpha of 0.05. All statistical analyses were performed using SPSS, version 28 (IBM Corp., Armonk, NY, USA). Power calculation was performed using G*Power, release 3.1.9.4.27,28
Results
Of the 608 participants enrolled in the CITU study, 52 were removed due to missing key demographic data, and 95 were removed because their tobacco product use classification was outside the scope of the current study (Figure S1 in the online supplementary material), including former smokers/users, current user of tobacco products not investigated in this study (i.e., cigars, bidi/cigarillos, pipes, hookah, or smokeless tobacco), infrequent/irregular tobacco users, and participants with partially completed surveys of tobacco product use. Among those with complete demographic and tobacco group information, 137 were missing CAC measurement data (Figure S1 online). The final dataset included 324 participants, of which 65 were never tobacco users, 19 were sole e-cigarette users, 212 were sole cigarette users, and 28 were dual users. General characteristics of the cohort included in the final dataset are presented in Table 1. The final dataset (n = 324) was 44% female, 48% Black/African American, with a mean age of 31 ± 7 years. Mean age, sex, race, body mass index (BMI), and the remaining clinical characteristics of participants in the final dataset were similar to participants excluded from analysis due to missing CAC measurements (n = 137) and are described in Table S3 (available online).
Patient cohort characteristics.
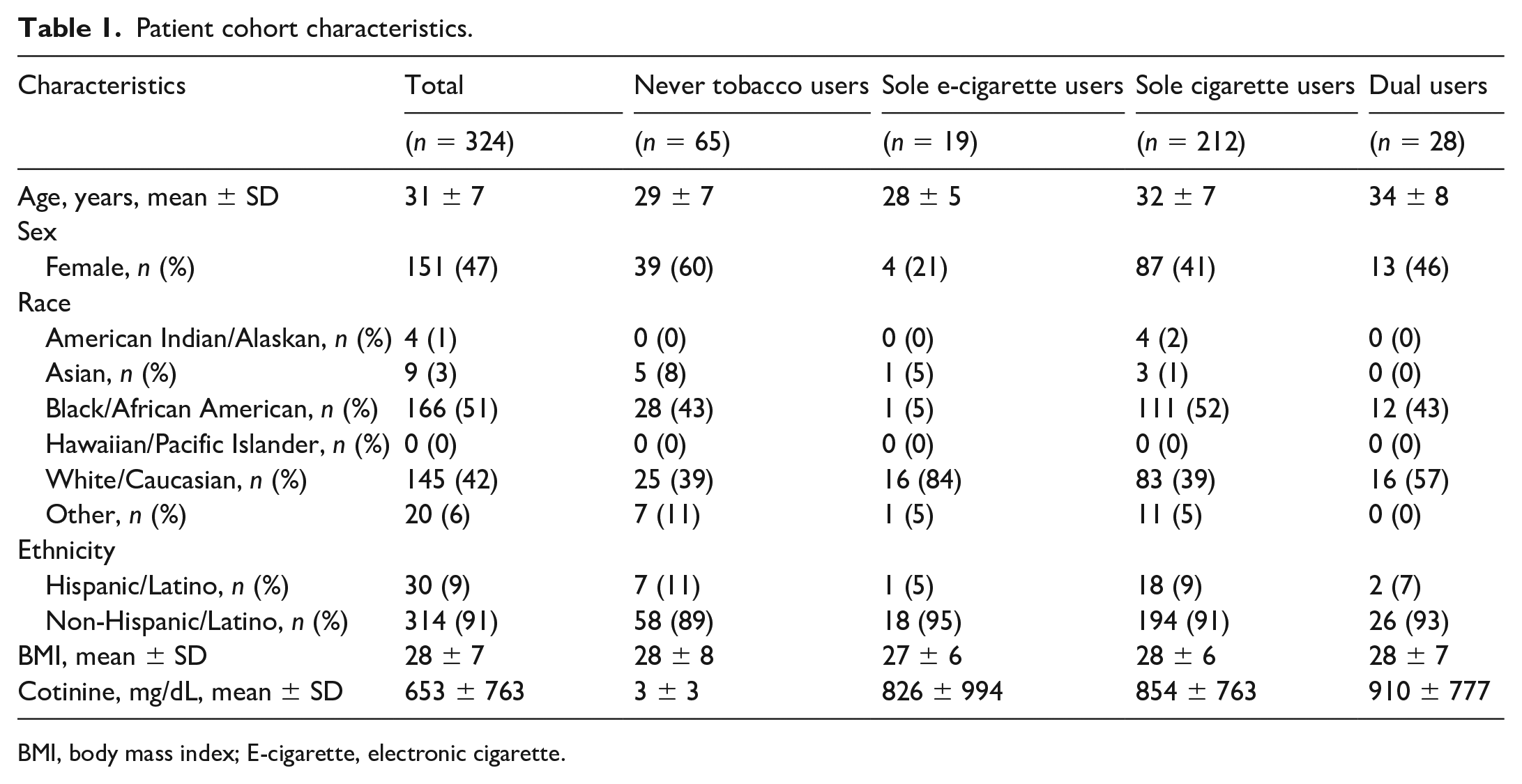
BMI, body mass index; E-cigarette, electronic cigarette.
Sole cigarette users
Among current sole cigarette users, we observed higher levels of two CAC subsets in comparison with never tobacco users: CAC 5 (β = 0.4; 95% CI: 0.2; p = 0.03) and CAC 10 (β = 0.3; 95% CI: 0.2, 0.4; p = 0.004) (Table 2, Figures 1–3). Both CAC subsets that were higher in sole combustible cigarette users were characterized by CD146+, which represents a population of endothelial lineage cells. Furthermore, two CD34+ positive CAC subpopulations, CAC 9 (β = −0.2; 95% CI: −0.4, −0.1; p = 0.04) and CAC 15 (β = −0.3; 95% CI: −0.5, −0.1; p = 0.04), were both significantly lower among current sole cigarette users (Table 2, Figure 4, and Figure S2 online).
Multivariable adjusted associations between tobacco product use and circulating angiogenic cell levels.
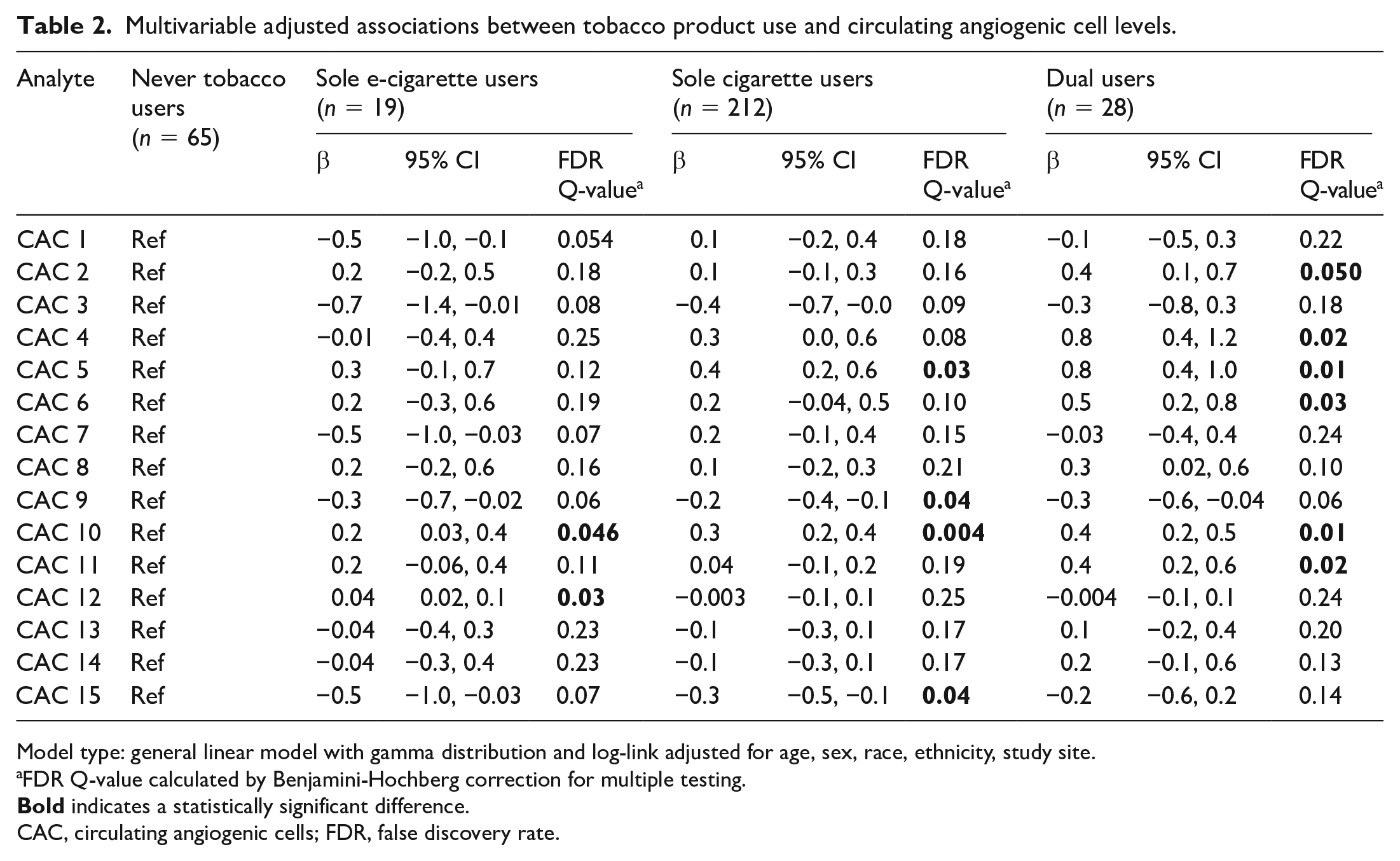
Model type: general linear model with gamma distribution and log-link adjusted for age, sex, race, ethnicity, study site.
FDR Q-value calculated by Benjamini-Hochberg correction for multiple testing.
CAC, circulating angiogenic cells; FDR, false discovery rate.
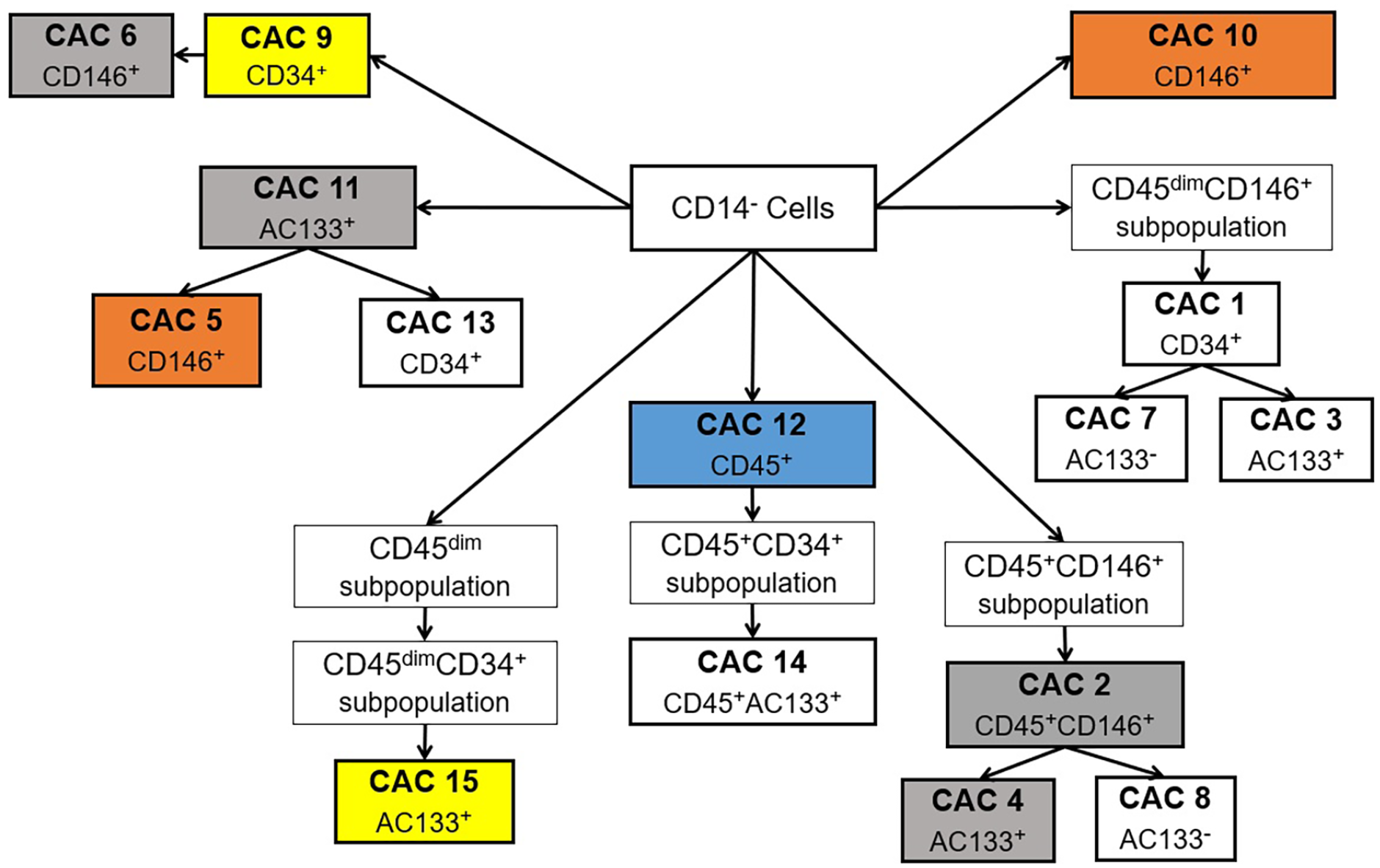
Association between tobacco product use and circulating angiogenic cells via the flow cytometry gating scheme.
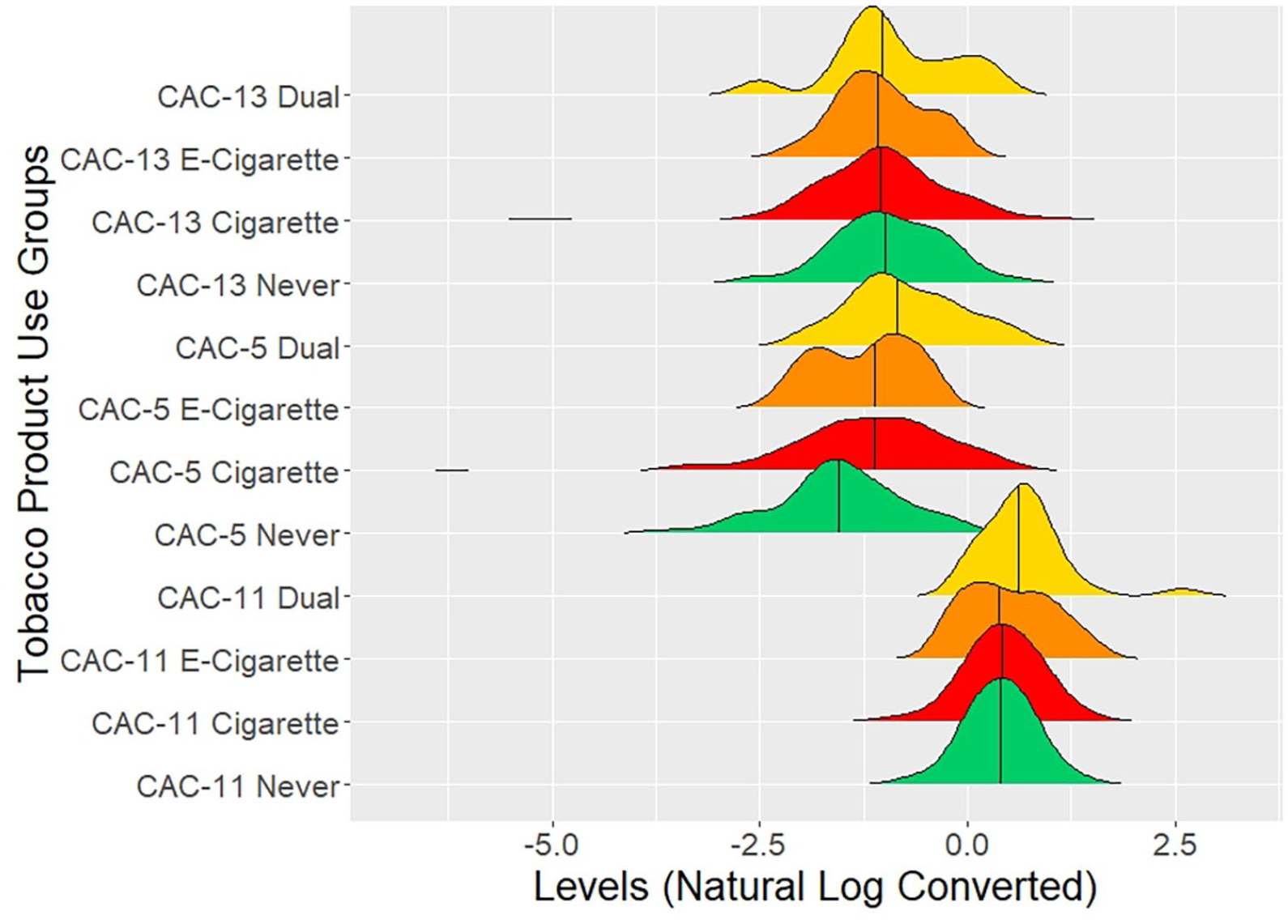
Circulating angiogenic cell levels among tobacco product use groups with a primary flow cytometry gate of early progenitor/stem surface marker (AC133+).
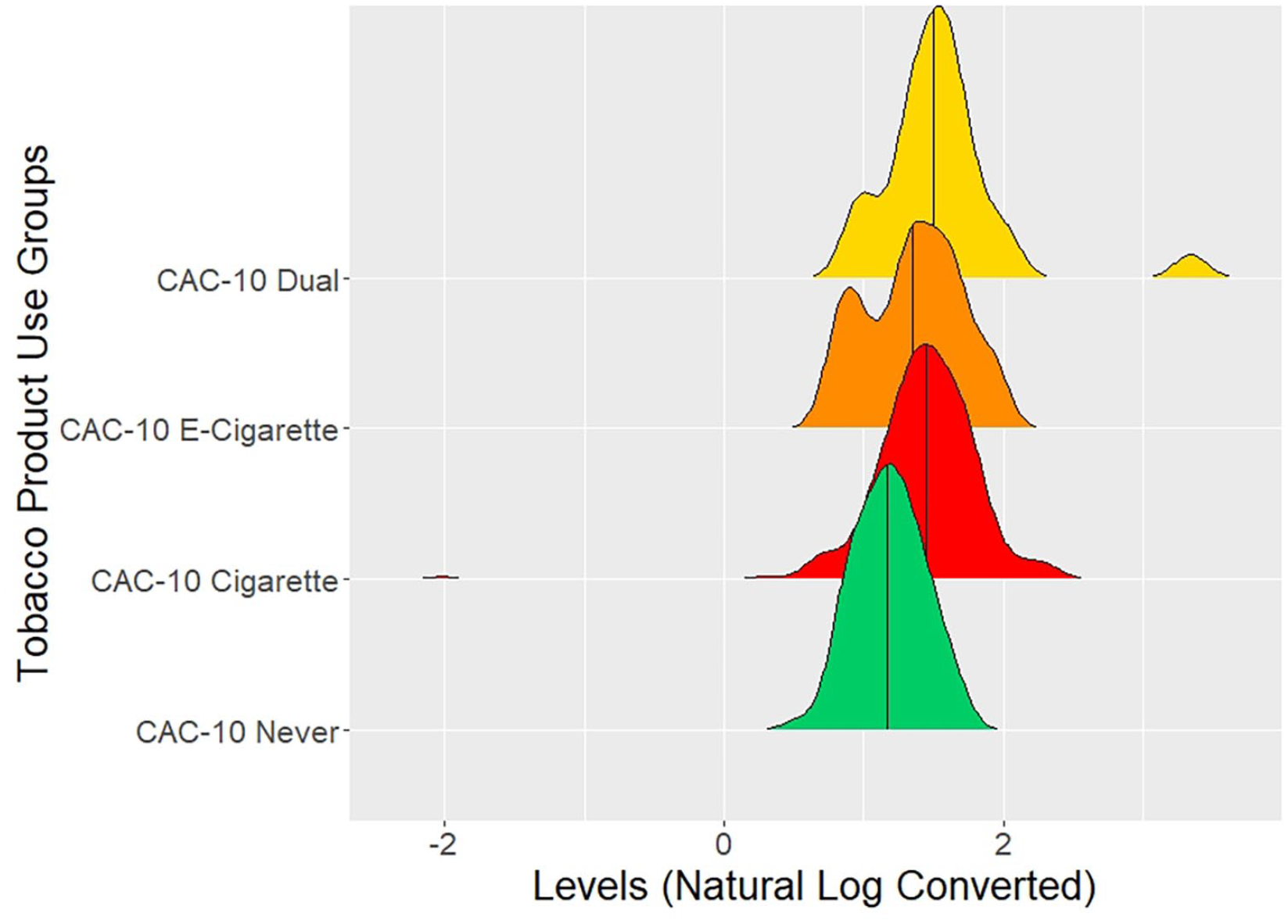
Circulating angiogenic cell levels among tobacco product use groups with a primary flow cytometry gate of endothelial surface marker (CD146+).
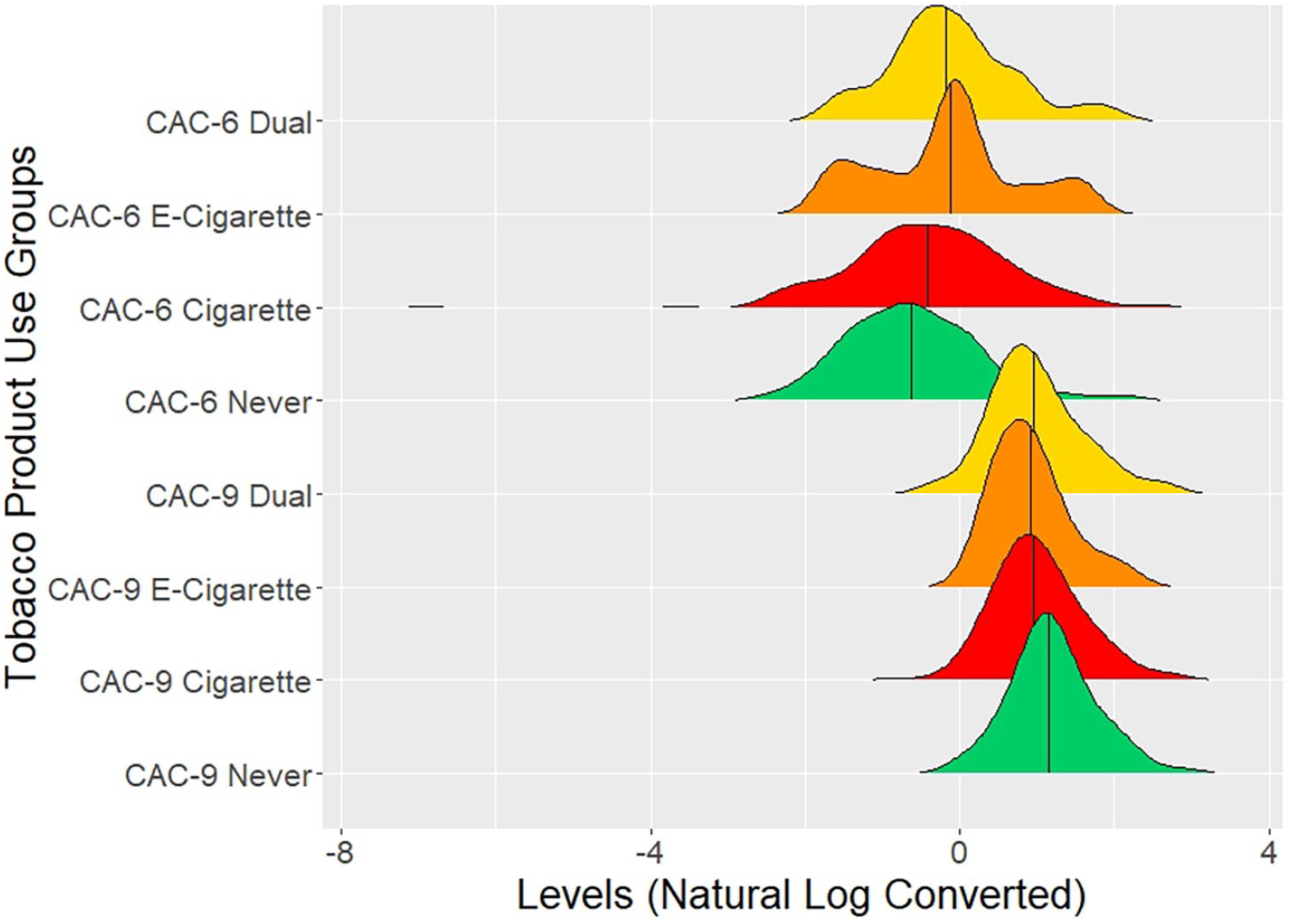
Circulating angiogenic cell levels among tobacco product use groups with a primary flow cytometry gate of stem surface marker (CD34+).
Dual users
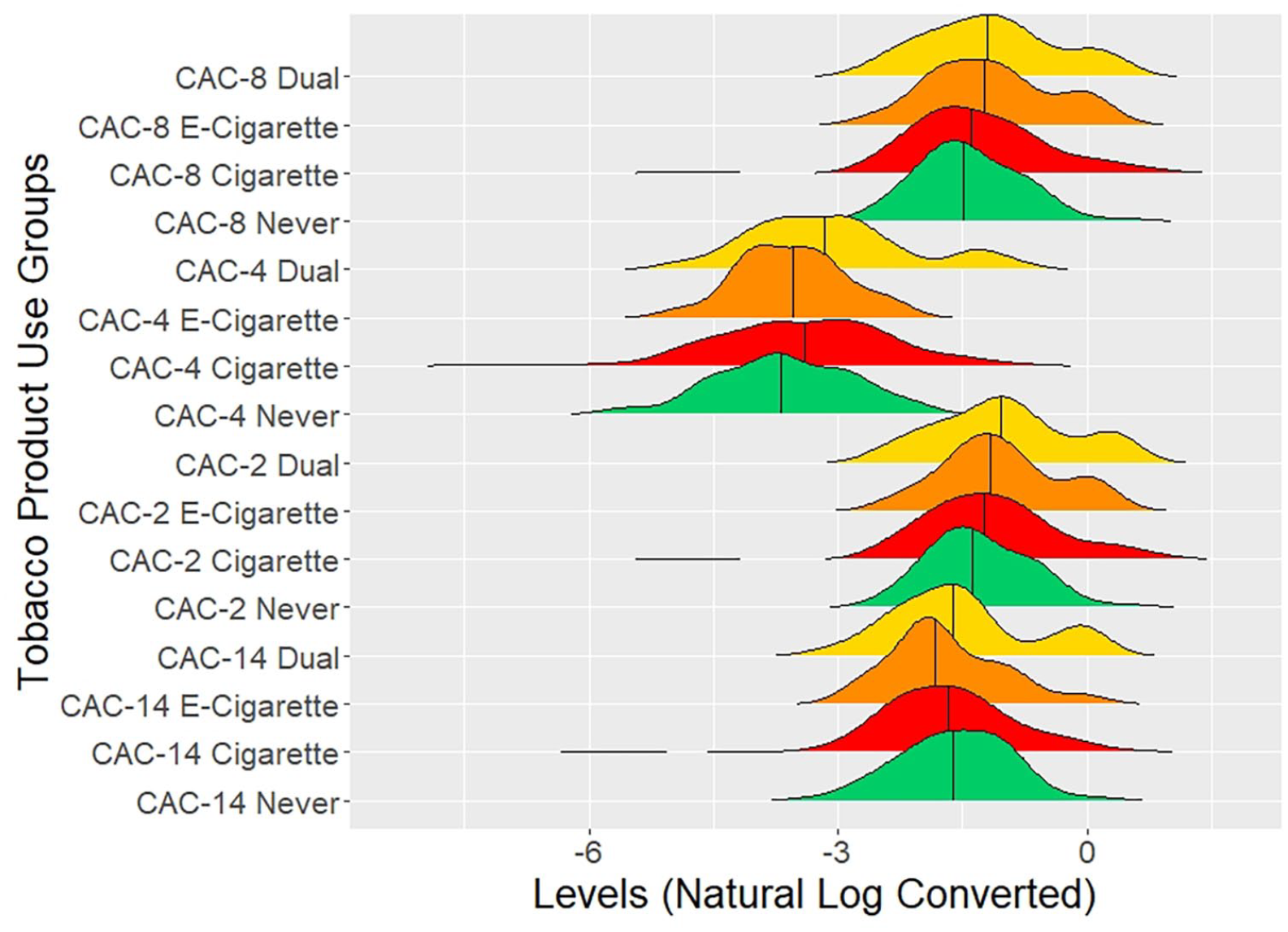
Dual users displayed the greatest number of CAC subsets that were higher than never tobacco users (Table 2 and Figure 1). Similar to sole cigarette users, two CD146+ CAC subpopulations, CAC 5 (β = 0.8; 95% CI: 0.4, 1; p = 0.01) and CAC 10 (β = 0.4; 95% CI: 0.2, 0.5; p = 0.01), were also higher in dual users (Figures 2 and 3, respectively). Two additional CD146+ CAC subpopulations, CAC 6 (β = 0.5; 95% CI: 0.2, 0.8; p = 0.03) and CAC 4 (β = 0.8; 95% CI: 0.4, 1.2; p = 0.02), were also higher in dual users (Figures 4 and 5, respectively). The levels of CAC 2 (β = 0.4; 95% CI: 0.1, 0.7; p = 0.50 ), which is positive for stem (CD34), leukocytic (CD45), and endothelial (CD146) markers, were higher in dual users (Figure 5). In addition, CAC 11 (β = 0.4; 95% CI: 0.2, 0.6; p = 0.02), an AC133+ (early progenitor/stem cell) subpopulation, was higher in dual users (Figure 2).
Circulating angiogenic cell levels among tobacco product use groups with a primary flow cytometry gate of positive leukocytic surface marker (CD45+).
Sole e-cigarette users
Sole e-cigarette users, as compared to never tobacco users, showed higher circulating levels of two CAC subsets: CAC 10 (β = 0.2; 95% CI: 0.03, 0.4; p = 0.046) and CAC 12 (β = 0.04; 95% CI: 0.02, 0.1; p = 0.03) (Table 2, Figures 1 and 6). CAC 10 is a pure endothelial (CD146+) subpopulation, whereas CAC 12 is a leukocyte (CD45+) marker subpopulation. When compared with sole combustible cigarette users, sole e-cigarette users did not show any statistically significant associations with any CAC subtypes (Table 3).
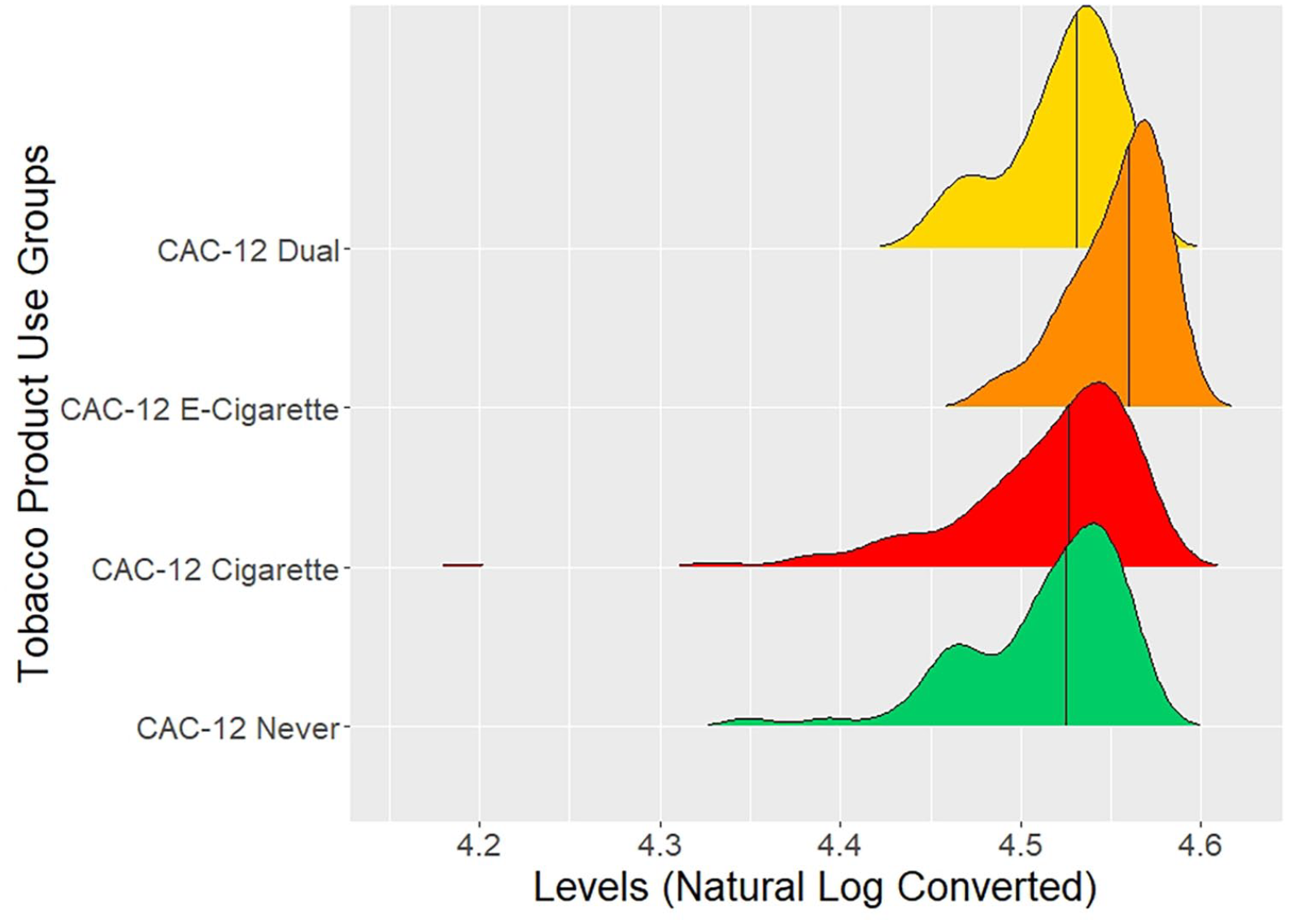
Circulating angiogenic cell levels among tobacco product use groups with a primary flow cytometry gate of CAC 12 (also positive leukocytic surface marker [CD45+]).
Multivariable adjusted associations of circulating angiogenic cell levels between sole cigarette users and sole electronic cigarette users.
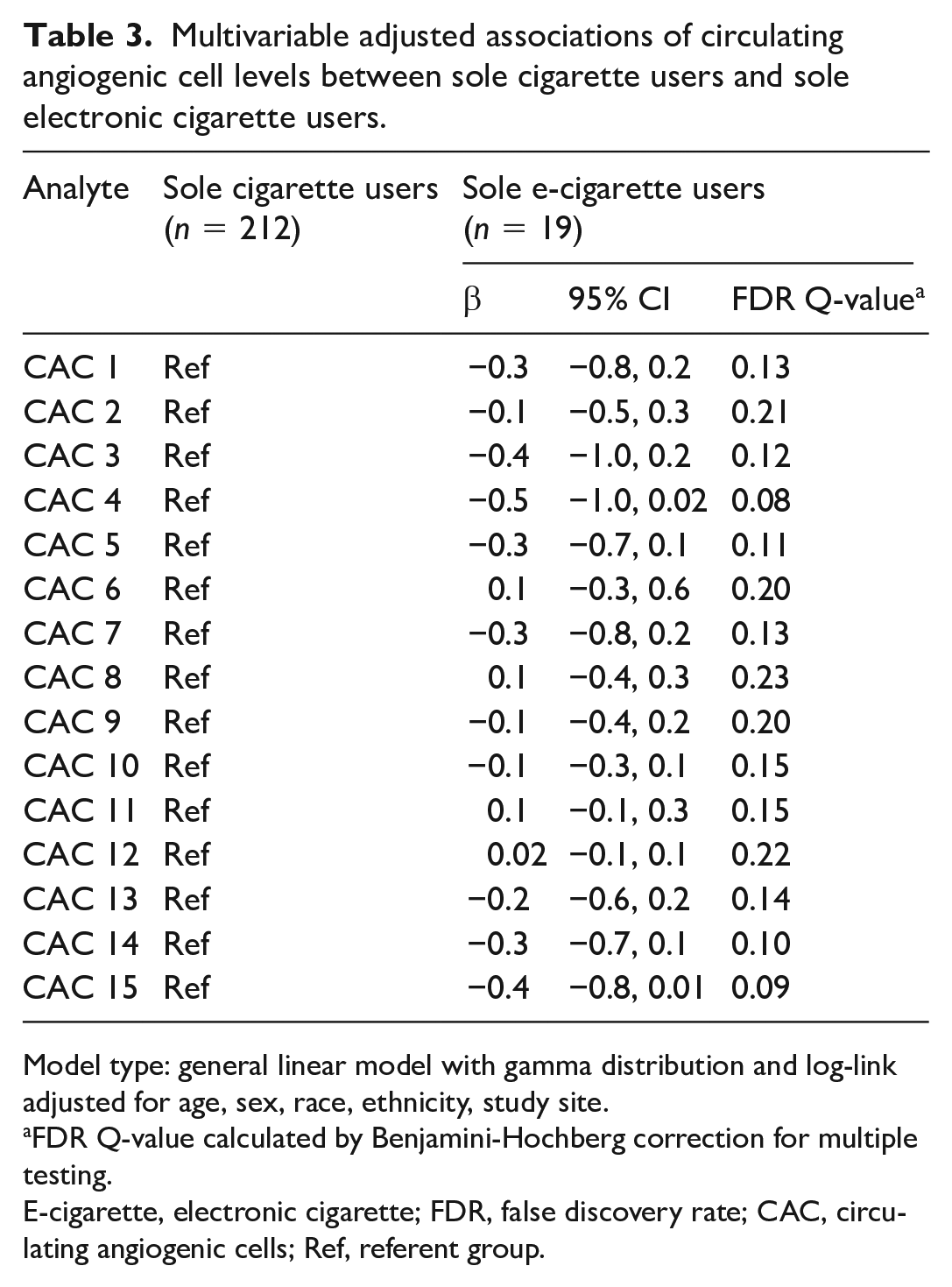
Model type: general linear model with gamma distribution and log-link adjusted for age, sex, race, ethnicity, study site.
FDR Q-value calculated by Benjamini-Hochberg correction for multiple testing.
E-cigarette, electronic cigarette; FDR, false discovery rate; CAC, circulating angiogenic cells; Ref, referent group.
Discussion
In this cross-sectional study of otherwise healthy participants, we found distinct profiles of CACs associated with tobacco use. In users of combustible cigarettes, both alone and combined with e-cigarettes, we observed higher circulating levels of CACs characterized by endothelial surface markers whereas lower circulating levels of CACs with stem surface markers. Dual users had higher levels of additional CACs expressing early progenitor cell surface markers. In sole e-cigarette users, we observed an association with higher levels of two CAC subpopulations, one with endothelial surface markers and one with leukocytic surface markers. Overall, these findings suggest that the use of e-cigarettes and combustible cigarettes have differential associations with circulating populations of cells with regenerative potential (i.e., CACs).
The findings of previous studies suggest that smoking combustible cigarettes has a variable relationship with CAC levels. Acute smoking induces direct endothelial injury, stimulating CAC mobilization from the vessel wall leading to higher measured levels in the blood.19,21,29,30 The chronic use of combustible cigarettes has been reported to be associated with lower levels of CACs, potentially reflecting depletion of these cells in circulation due to repetitive cycles of endothelial injury and repair.6,19,29,31,32 In the present study, we measured the levels of these cells in participants who briefly fasted from tobacco to measure chronic exposure. Nevertheless, we found higher levels of CACs with endothelial surface markers in all three study groups, an observation which is consistent with the notion that use of tobacco smoking products induces ongoing vascular injury. Reasons for such discordance between different studies are unclear, but it is possible that our findings reflect the relatively young age of our study participants who continue to mobilize vascular CACs in response to the ongoing injury from exposure to combustible cigarettes. Although less is known about the relationship between e-cigarettes and CACs, it has been reported that in healthy cigarette smokers, acute use of e-cigarettes results in elevation of a single CAC population (CD309+/CD34+) with endothelial and stem surface markers at 1 hour postuse that returned to preuse levels at 24 hours. 30 These results are backed by the findings in our study where both endothelial and stem surface marker CACs were higher in the e-cigarette use group. Nonetheless, the effects of chronic e-cigarette use remain unknown. Similarly, our study also provides clear evidence that the chronic use of e-cigarettes is additionally associated with higher levels of CACs with an inflammatory/hematopoietic phenotype.
We found that the cell populations affected by e-cigarette use were different from those affected by the use of combustible cigarettes or dual use. Consistent with previous work, we observed higher effect size (β coefficient) among dual users as compared to combustible or e-cigarette users on the levels of CACs with endothelial surface markers, which alludes to the combined effect of combustible and e-cigarette exposure. It is interesting that a greater number of endothelial surface marker-associated CACs were higher in dual users than in sole combustible cigarette smokers or sole e-cigarette users. This could reflect additional injury related to exposure to additional deleterious tobacco products or to more frequent use as e-cigarettes are often used in areas where traditional cigarettes are not allowed. It is also possible that the additional higher levels of CACs among dual users reflects an intermittent use of combustible cigarettes and a return to the ability to mount an acute injury response. Moreover, the CAC subsets associated with dual use may reflect additional exposure to components in e-cigarettes among people who also use combustible products.
Among the sole e-cigarette users, we observed an association with one CAC with a leukocytic surface marker and one CAC with endothelial cell markers. These findings suggest that CAC subsets with pro-inflammatory and endothelial surface markers are higher among e-cigarette users. The association of CAC subsets with endothelial as well as inflammatory cell surface markers with sole e-cigarette use suggests that local vascular injury from e-cigarette use may be associated with a more general systemic injury which leads to increased recruitment of hematopoietic cells from the bone marrow. Nonetheless, our results should be interpreted with some caution given the smaller number of individuals in the sole e-cigarette group. It remains possible that with a larger number of e-cigarette users, changes in other CAC populations may become evident.
Information about the patterns of changes in CAC levels in e-cigarette and tobacco product users has the potential to contribute to our understanding of the specific health effects of these products as well as to identify new biomarkers of specific tobacco product exposure. CACs are validated biomarkers of ongoing vascular injury and of the capacity for vascular repair.13,14 Previous work has shown that CACs can promote neoangiogenesis by localizing to the site of injury and invoking short-term secretion of paracrine factors.29,33–36 The paracrine effect may explain the singular functional outcome (i.e., vascular repair) by complex cell populations expressing a variety of cell surface markers. Although the associations between different potentially overlapping CAC subtypes with tobacco use are challenging to relate to specific events inside the vascular wall, differences in CAC levels across tobacco user groups may have utility as biomarkers reflecting dynamic patterns of vascular and systemic injury due to the use of different tobacco products. Given the long latency period between tobacco exposure and the occurrence of clinical cardiovascular events, intermediate biomarkers such as CACs, which reflect vascular injury, are valuable. The current study provides evidence that CACs have the potential to be developed as surrogate biomarkers of vascular health, independent of their influence over vascular function, which was not the focus of this study. Therefore, it will be important to continue to assess CAC levels with tobacco product transitions in longitudinal studies of tobacco product use.
Study limitations
Despite its many strengths – comprehensive assessment of different CAC subpopulations in a large cohort of individuals using different tobacco groups, the inclusion of a referent group, 51% Black/African American study participants, and directly validated use of specific products – the current study has several limitations. First, the sample size of the sole e-cigarette users and dual users was smaller in comparison with the two referent groups – never tobacco users and sole cigarette users. Moreover, the cross-sectional and observational nature of the study precluded any temporal evaluation of tobacco product use and CACs. In addition, there may be residual confounding due to differences between the tobacco product users, though the inclusion of young individuals without existing cardiovascular disease or risk factors limits the effects of confounding. The study largely included e-cigarette users, who currently or previously used combustible cigarettes, which does not provide information about sole e-cigarette use with no prior use of combustible products. Finally, the field of e-cigarettes is a rapidly evolving arena, and the e-cigarette products used by participants in this study are earlier generations than the most common current e-cigarette or vaping products. A larger study with a balanced cohort is needed to appreciate the entire spectrum of effects of e-cigarettes on cardiovascular health and cardiovascular disease risk.
Conclusions
The present study provides information about the associations of novel tobacco product use with known markers of vascular injury. Importantly, users of combustible cigarettes, e-cigarettes, and dual product users display higher levels of CAC subtypes with endothelial surface markers suggestive of ongoing vascular injury. In addition, sole e-cigarette users showed higher levels of CAC subtypes with endothelial surface markers or inflammatory (leukocytic) markers, suggestive of vascular injury. These findings support measurements of CAC levels as dynamic markers of vascular health in tobacco product users. Additional longitudinal studies of CAC subtypes are needed in tobacco product users who switch to e-cigarette use.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X221126205 – Supplemental material for Association of electronic cigarette use with circulating angiogenic cell levels in healthy young adults: Evidence for chronic systemic injury
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X221126205 for Association of electronic cigarette use with circulating angiogenic cell levels in healthy young adults: Evidence for chronic systemic injury by Alok R Amraotkar, Ugochukwu S Owolabi, Marina V Malovichko, Sana Majid, Robert M Weisbrod, Emelia J Benjamin, Jessica L Fetterman, Glenn A Hirsch, Sanjay Srivastava, Ram Poudel, Rose Marie Robertson, Aruni Bhatnagar, Naomi M Hamburg and Rachel J Keith in Vascular Medicine
Supplemental Material
sj-pdf-2-vmj-10.1177_1358863X221126205 – Supplemental material for Association of electronic cigarette use with circulating angiogenic cell levels in healthy young adults: Evidence for chronic systemic injury
Supplemental material, sj-pdf-2-vmj-10.1177_1358863X221126205 for Association of electronic cigarette use with circulating angiogenic cell levels in healthy young adults: Evidence for chronic systemic injury by Alok R Amraotkar, Ugochukwu S Owolabi, Marina V Malovichko, Sana Majid, Robert M Weisbrod, Emelia J Benjamin, Jessica L Fetterman, Glenn A Hirsch, Sanjay Srivastava, Ram Poudel, Rose Marie Robertson, Aruni Bhatnagar, Naomi M Hamburg and Rachel J Keith in Vascular Medicine
Footnotes
Acknowledgements
We would like to thank the participants for agreeing to participate in this study. We would also like to thank the study staff and trainees who provided their valuable contribution for the success of this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Research reported in this publication was supported in-part by the National Heart, Lung, and Blood Institute of the National Institutes of Health under Award Numbers U54HL120163 and P50HL120163. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the US Food and Drug Administration.
Data availability statement
Primary de-identified data supporting the findings of this study are available through the American Heart Association Tobacco Regulation and Addiction Center upon request.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.