
Abstract

Retinal vein occlusion (RVO) is an important cause of loss of visual acuity in older people and the second cause of retinal vascular disease after diabetic retinopathy. Pooled data from population studies suggest that over 28 million adults are affected by this condition in the world, and this number is expected to increase in the next decades.1,2 Advances in therapeutic possibilities with anti-vascular endothelial growth factor (VEGF) agents have revolutionized the treatment of this disease. Other therapeutic approaches include use of laser, steroids, and surgery. In addition, strict control of cardiovascular risk factors such as hypertension or diabetes is required in order to reduce the risk for recurrent RVO. 3 Recurrent RVO may lead to a subsequent worsening in visual prognosis, higher requirement of local therapies, and an increment in health care costs.4 –6 However, little is known about which patients are at increased risk for recurrences. A better understanding of at-risk patients could likely help to design better prevention strategies and to detect recurrent RVO earlier.
For many years, RVO has been considered as an atypical form of venous thromboembolism (VTE), although recent data suggest a particular behavior in which arterial involvement is crucial.
7
This is why we recruited patients with RVO into the RIETE registry. RIETE (
Consecutive patients with RVO confirmed by fundus examination and fluorescein angiography were enrolled in RIETE. Patients were excluded if they were currently participating in a therapeutic clinical trial with a blinded therapy. The study protocol was approved by the Ethics Committees of the Hospital Universitari Germans Trias i Pujol (Badalona, Spain) and the Institutional Review Board of NorthShore University Health System (Evanston, IL, USA). All patients (or their relatives) provided written or oral consent for participation in the registry, in accordance with local ethics committee requirements.
The following parameters were recorded when the index episode of RVO was diagnosed: demographics, coexisting conditions such as cardiovascular risk factors, risk factors for VTE, laboratory data at baseline, and concomitant drugs. Patients were managed according to the clinical practice of each participating hospital. After discharge, all patients were followed up in the outpatient clinic. All outcomes were classified as reported by the clinical centers.
We firstly conducted a descriptive analysis of baseline characteristics, systemic treatment, and outcomes of patients with RVO. Then, Cox proportional hazard models were used to identify patients at increased risk for recurrent RVO. Covariates included in the adjusted model were those for which a statistically significant difference (a threshold p-value of 0.1 was set to assess the significance of differences) was found between the two subgroups, and a forward selection was used for the covariate selection in the multivariable model. Statistical analyses were conducted with IBM SPSS Statistics for Windows, Version 20.0 (IBM Corp., Armonk, NY, USA).
Up to March 2021, 555 patients with RVO were enrolled in RIETE. Of these, 39% had central vein thrombosis, 51% branch vein thrombosis, and 7.0% had hemiretinal vein thrombosis. Their mean age was 65 ± 14 years, 44% were women, 64% were hypertensive, 36% had hyperlipidemia, 27% diabetes, 17% were current smokers, and 52% underwent thrombophilia testing (Table 1). Interestingly, the classic risk factors for VTE (recent surgery, immobility, estrogen use or cancer) were uncommon. Overall, 30 patients (5.4%) received anticoagulant therapy, 108 (19.5%) received antiplatelet drugs (aspirin 93, clopidogrel 15), and 417 (75.1%) did not receive any antithrombotic drug.
Uni- and multivariable analysis for recurrent retinal vein occlusion.
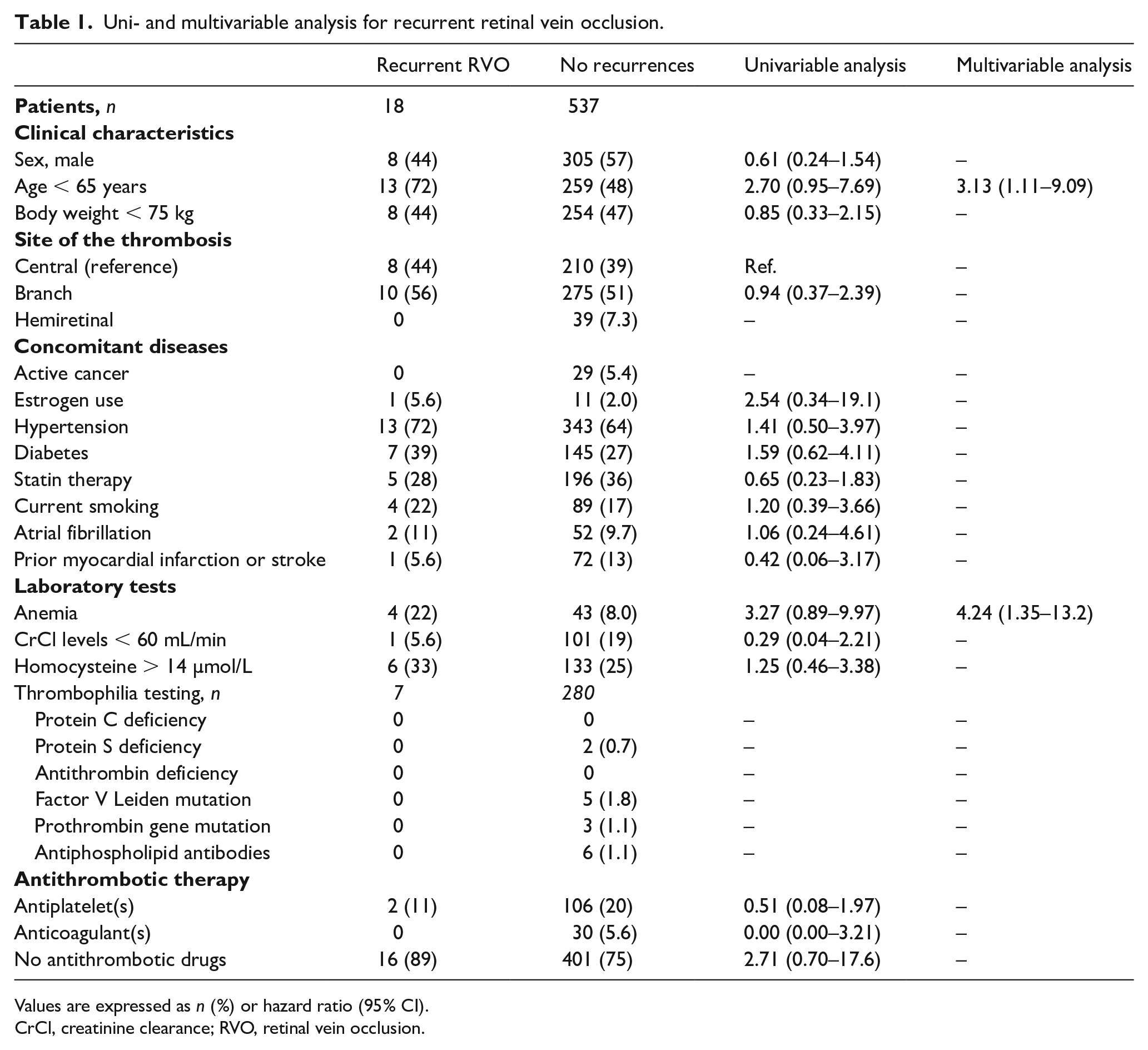
Values are expressed as n (%) or hazard ratio (95% CI).
CrCl, creatinine clearance; RVO, retinal vein occlusion.
During follow-up (median, 897 days), 18 patients (3.2%) developed recurrent RVO (1.23 events per 100 patient-years). On multivariable analysis, only age < 65 years (adjusted hazard ratio [HR]: 3.13; 95% CI: 1.11–9.09) and anemia at baseline (adjusted HR: 4.24; 95% CI: 1.35–13.25) were independently associated with an increased risk for recurrent RVO (Table 1).
The current study has a number of limitations that should be addressed. First, RIETE is an observational registry, and as such we cannot compare the effectiveness and/or safety of different therapies. However, our data are hypothesis generating and may help in designing specific trials to validate our findings. Second, selection bias could have skewed the study sample, since RIETE is a registry and patients were not randomly allocated but received the prescription of their doctor’s choice. Third, we do not have enough data to assess the influence of elements that may change during the course of the disease and could be associated with the risk for recurrent RVO, such as renal function, use of concomitant medications, or presence of concomitant diseases. The RIETE registry did not capture data regarding adjunctive ophthalmological therapies for RVO that may have had an impact on outcome or recurrence. Finally, the sample size of patients entering into the multivariable analysis was rather small.
The rate of RVO recurrences in our cohort was consistent with previously reported data.4,5 Unfortunately, only two variables (age and anemia) were independently associated with an increased risk for recurrent RVO. Half of the 555 patients in our cohort (49%) were aged < 65 years, and their risk for recurrent RVO was threefold higher than in those aged ⩾ 65 years. To our knowledge, these findings have not been reported thus far and warrant further investigation. In the literature, only hypertension,3,9 hyperlipidemia, and hyperhomocysteinemia6,10 have been associated with an increased risk for recurrent RVO, but with a low level of evidence. None of these variables was associated with an increased risk in our cohort. Further studies with large samples of patients are needed to confirm the relationship between recurrent RVO and age < 65 years or anemia.
In conclusion, among 555 patients presenting with RVO, 15 (3.2%) developed recurrent RVO during follow-up (median, 897 days). On multivariable analysis, age < 65 years and anemia were independently associated with an increased risk for recurrent RVO.
Footnotes
Appendix
Acknowledgements
We express our gratitude to the RIETE Registry Coordinating Center, S&H Medical Science Service, for their quality control data, logistic and administrative support, and to Prof. Salvador Ortiz, Universidad Autónoma Madrid and Silvia Galindo, both Statistical Advisors in S&H Medical Science Service, for the statistical analysis of the data presented in this paper.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
We express our gratitude to Sanofi Spain, Leo Pharma and Rovi for supporting this Registry with an unrestricted educational grant. Sanofi, Leo Pharma, and Rovi had no access to the data at any time nor did they have any influence or implication on the preparation of the manuscript.