
Abstract

What is external iliac artery endofibrosis (EIAE)?
External iliac artery endofibrosis (EIAE), also known as ‘cyclist’s iliac syndrome’, is an uncommon condition typically affecting young high-endurance athletes. Though EIAE was first described in the 1980s as a cause of lower leg pain in professional cyclists, it is still largely misdiagnosed. 1 Moreover, arriving at the correct diagnosis can be difficult since vascular disease is unexpected in young healthy athletes.
Arteries are the blood vessels that carry oxygenated blood to the organs and tissues of the body. The external iliac arteries are the main blood supply to the muscles in the legs. EIAE leads to restriction of blood flow that is not related to atherosclerotic plaque (calcification from cholesterol plaque or fatty deposits). The vessel blockage (stenosis) in EIAE can be caused by endofibrosis – a thickening of the intima, the inner layer of the vessel wall – or by kinking of the artery. In either scenario, the blood flow to the leg is reduced, which decreases oxygen delivery to the muscles and causes symptoms. EIAE has been mostly reported in cyclists, but cases have been reported in other endurance athletes including triathletes, runners, cross-country skiers, rowers, and rugby players. 2
What arteries are involved in EIAE?
Most cases (more than 90%) of EIAE, as the name suggests, involve endofibrosis and/or kinking of the external iliac artery. However, in a small number of cases, other arteries of the legs, including the common iliac, common femoral, or deep femoral arteries, have been involved. 3 EIAE is frequently diagnosed only on one side of the body, with the left side being more commonly affected than the right. 4
What causes EIAE?
The short answer is that we are still not sure. However, some theories have been postulated. 1 The likely cause is that repeated direct mechanical stress leads to the development of fibrous tissue and subsequent narrowing inside the artery. The external iliac artery is the most commonly damaged due to its anatomical position and attachment to the psoas muscle during hip flexion (Figure 1). 1
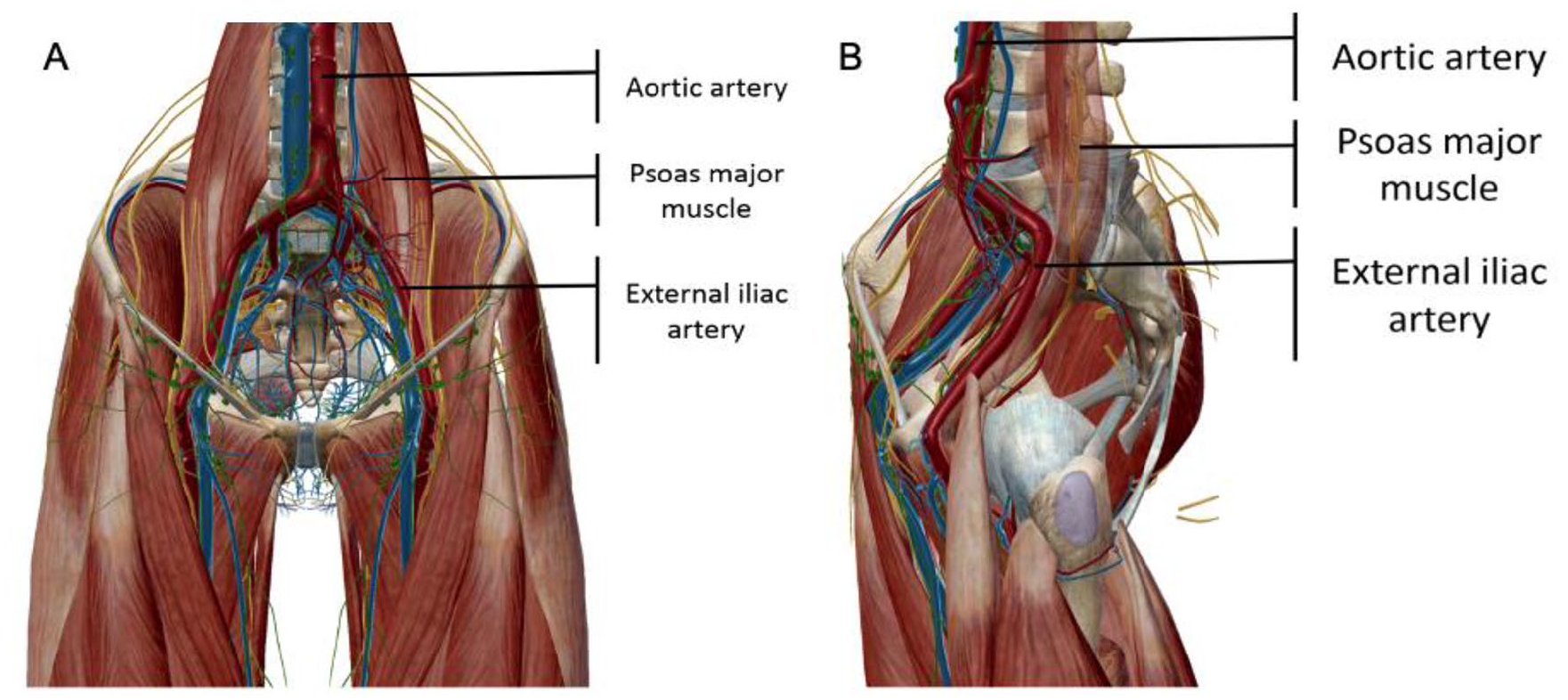
External iliac artery and psoas muscle anatomy: anterior (
EIAE occurs in high-level athletes due to the stress on the artery from hundreds of hours of high-intensity training, with continuous and repetitive flexion of the artery potentially causing damage and kinking. EIAE is hypothesized to be more common in cyclists due to the flexed posture of the hip, causing repetitive stretching and deformation of the iliac arteries 5 (Figure 2). Furthermore, EIAE may also be the result of longer than average iliac vessels. Such elongation makes the artery more tortuous (curvy) and likely to kink during hip flexion.
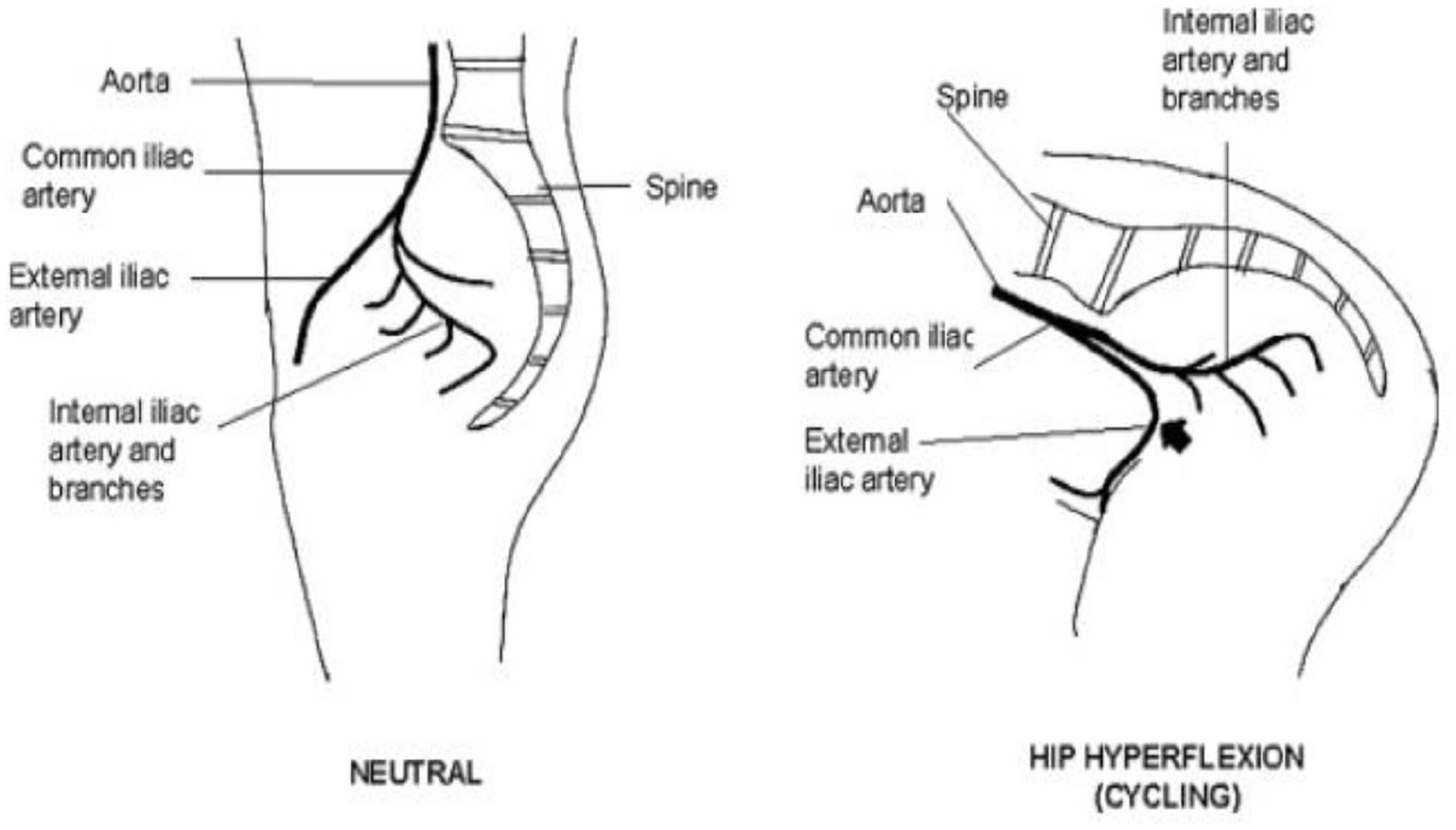
Hip hyperflexion: anatomical effect on the external iliac artery. Arrow demonstrates the acute angle of the external iliac artery during hip hyperflexion.
Additionally, the increased growth (hypertrophy) of the psoas muscles can worsen the kinking and mechanical stress on the external iliac artery since it increases the arterial repositioning when hyper-flexing the hip. Cyclists with EIAE have been found to have asymmetric thighs, with the larger thigh circumference on the side with symptoms, further explaining why symptoms are usually on one side. 1 Intensity of training has also been associated with EIAE. Cyclists with EIAE had cycled an average of 120,000 km prior to the onset of symptoms, with more than 14,500 km per year. 1
Recent research has also suggested vasospasms as a potential contributor in the development of symptoms of EIAE. 6 A vasospasm is a sudden contraction of the muscular wall of blood vessels. One of the hypotheses says that the repeated damage to the blood vessels from exercise makes the vessels unable to dilate – the normal exercise response – and, instead, they constrict, narrowing the passage for oxygenated blood, leading to the common EIAE symptoms. 6
How common is EIAE and who is at risk?
The true prevalence of the condition is not known since it is often undiagnosed or misdiagnosed. But from the data available, EIAE is more common in men, and the patients are usually younger than 40 years of age. 1 The prevalence of EIAE may be as high as 10–20% among elite-performing athletes. The gender discrepancy may be related to the greater number of men participating in these high-intensity endurance sports. 1
What are the symptoms of EIAE?
Symptoms vary, but leg cramping is the most common. Patients generally have no symptoms at rest, and the cramping is usually on one side and comes on during high-intensity exercise. Patients may also report swelling, numbness, weakness, and/or pain in the calf, thigh, or buttock. In some patients, a whooshing sound (‘bruit’) may be heard over the iliac or femoral vessels after exertion or hip flexion. A bruit is a sound heard with the stethoscope by a health care provider that indicates turbulent blood flow.
Since these symptoms are nonspecific and the physical exam is often normal at rest, long delays of 12–41 months may occur from symptom onset to diagnosis. 1 The diagnosis may also be delayed since many athletes experience muscle pain, cramps, and fatigue from the usual metabolic stress associated with high-intensity exercise. Additionally, since these healthy athletes are in peak physical form, vascular disease is not expected, so the symptoms are usually attributed to musculoskeletal and neurological causes. 1
In summary, the symptoms of EIAE include:
Cramping of one leg when exercising
Swelling
Numbness
Pain in calf, thigh, and/or buttock
No symptoms at rest.
How is EIAE diagnosed?
The initial testing for EIAE is the measurement of an ankle–brachial index (ABI) before and after exercise (within 5 minutes of maximal-intensity running/cycling). The ABI is performed by measuring the blood pressure in the arms and the ankles with ultrasound. 7 Then the ankle pressure is divided by the arm pressure. A normal ratio is 1.0, and anything below this indicates a decrease in blood flow to the legs. EIAE patients often have normal ABI values at rest, but the ABI in the affected leg typically drops after exercise.
Another test for the diagnosis of EIAE is an ultrasound of the arteries, called a Doppler ultrasound, which uses sound waves to visualize the blood vessels and determine the speed and direction of blood flow in those vessels (Figure 3). The peak systolic velocity (the speed of the blood in the artery when the heart squeezes) of the symptomatic leg in a patient with EIAE after exercise is significantly higher if a blockage (stenosis) is present. Additionally, a duplex ultrasound, which also shows grayscale ultrasound images of the arteries and tissues, may reveal endofibrosis and kinking of the artery. The benefit of duplex ultrasound is that it is relatively inexpensive, noninvasive, and widely available. 7
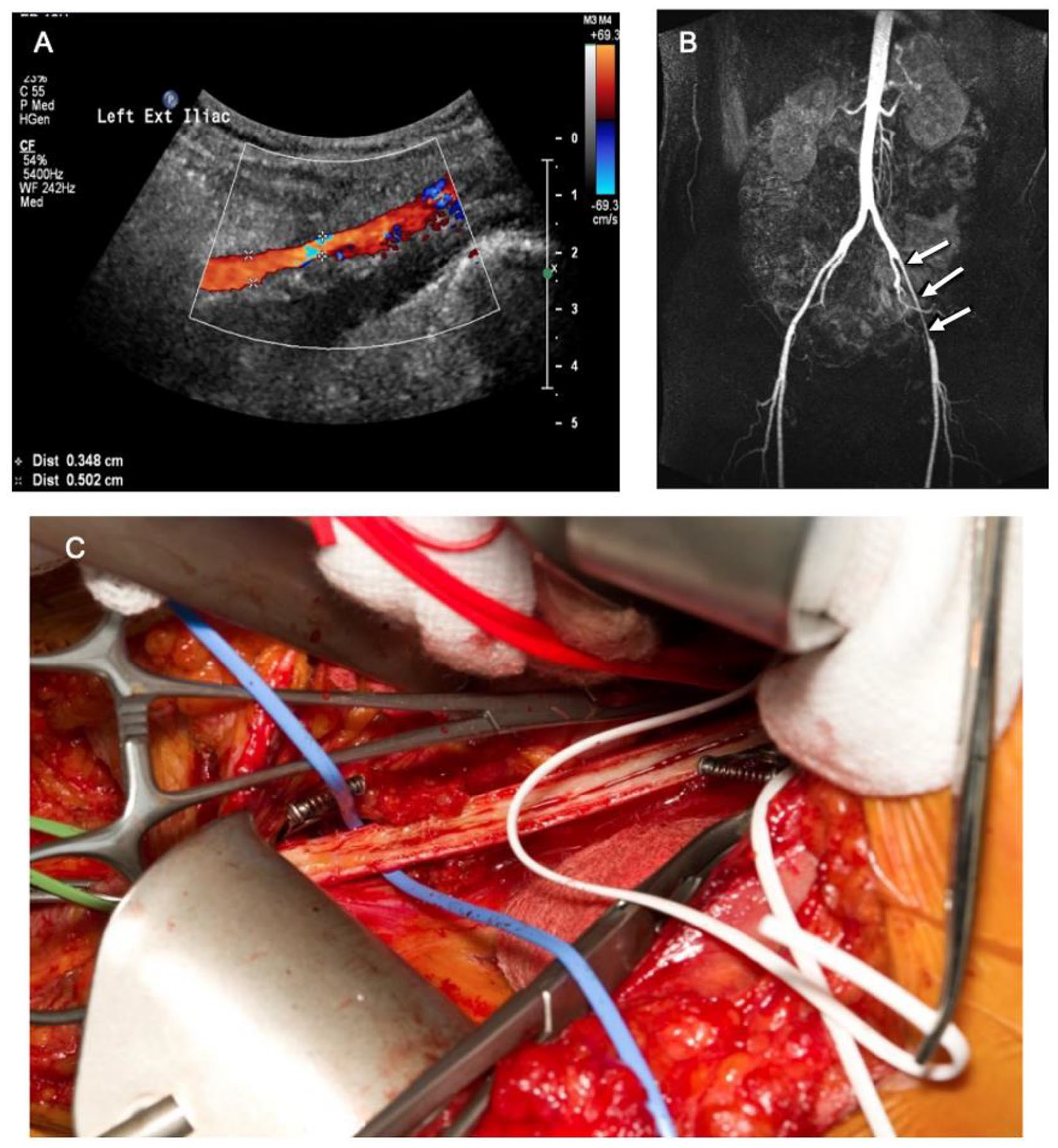
Duplex ultrasound (
Magnetic resonance angiography (MRA) and computed tomographic angiography (CTA) can also be used to assess the flow through the arteries. CTA and MRA are noninvasive imaging tests that use different techniques to create detailed images of the vessels. Both can be used to reconstruct the anatomy of the arteries and detect problems with blood flow (Figure 3). For more information, please see the Patient Information Page on these imaging tests. 8 These tests can also determine the length of the vessel and determine if surgery is needed. 1 However, these tests are more expensive, and the CTA exposes the patient to radiation.
To summarize, EIAD is diagnosed with the following tests:
ABI before and after exercise
Duplex ultrasound (grayscale and Doppler images)
MRA
CTA
How is EIAE treated?
Treatment depends on several factors. Conservative treatment should always be recommended before any major surgeries are considered. Such conservative treatments include changing the cycling body position, reducing exercise intensity, or occasionally switching sports. Recommended cycling position changes include raising handlebars, bringing the saddle forward to avoid hip hyperflexion, and avoiding pulling upwards on the pedals to prevent psoas muscle hypertrophy. 1
If the conservative approach does not work, open surgery is the current preferred treatment method. In general, less invasive treatments like stents and balloon angioplasties are not appropriate for EIAE.1,4,9 The surgical procedure depends on what is causing the patient’s symptoms. If the external iliac artery is kinked by its attachment to the psoas muscle, then the surgery would release the restrictive fibrous tissue and any tethering of the artery to the muscle. If the external iliac artery is longer than average, surgically shortening the artery may be necessary to relieve the symptoms. 1 Finally, if symptoms are caused by fibrosis of the vessel wall, then a procedure called an endarterectomy can be performed. This procedure surgically removes the fibrosis from the vessel wall, so the blood flow is no longer restricted (Figure 3). Some vascular surgeons have tried completely removing the narrowed portion of the artery and replacing it with a vein graft (a vein taken from another part of the body, usually the leg). 4 The recovery period and time before returning to sports depends on the surgery performed and complications, if any.
Summary
EIAE was originally described in the 1980s as a cause of leg pain in high-intensity cyclists. Symptoms of EIAE usually include leg and/or buttock cramping caused by a decrease in blood flow during intense physical activity. The decrease in blood flow can be caused by fibrosis of the wall of the artery, kinking of the artery, or an increase in the size of the pelvic muscle to which the artery attaches. Patients with EIAE are young and healthy athletes, so vascular disease is not suspected; thus, this condition often goes unrecognized or misdiagnosed. Tests to diagnose EIAE include exercise ABI, duplex ultrasound, MRA, and/or CTA. Conservative treatment involves changing the position during exercise, decreasing exercise intensity, or even stopping the current sport. If unsuccessful, the patient can undergo open surgery to correct the problem and restore the blood flow.
The ‘Vascular Disease Patient Information Page’ is a regular feature of Vascular Medicine. All articles in the collection are available for free online at http://journals.sagepub.com/vmjpatientpage. The Vascular Disease Patient Information Page is provided for educational purposes only and is not a substitute for medical advice.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.