
Abstract

Rasmussen aneurysm (RA), a false aneurysm arising from segmental pulmonary arteries, occurs secondary to infiltration of granulation tissue into the adventitia and media due to Mycobacterium tuberculosis (TB) 1 ; it has a prevalence of 5–8%.2,3 The most feared complication of RA is the thinning of the vessel wall, subsequent aneurysm formation, and rupture leading to massive hemoptysis; it has a mortality rate that ranges from 5% to 25%. 1
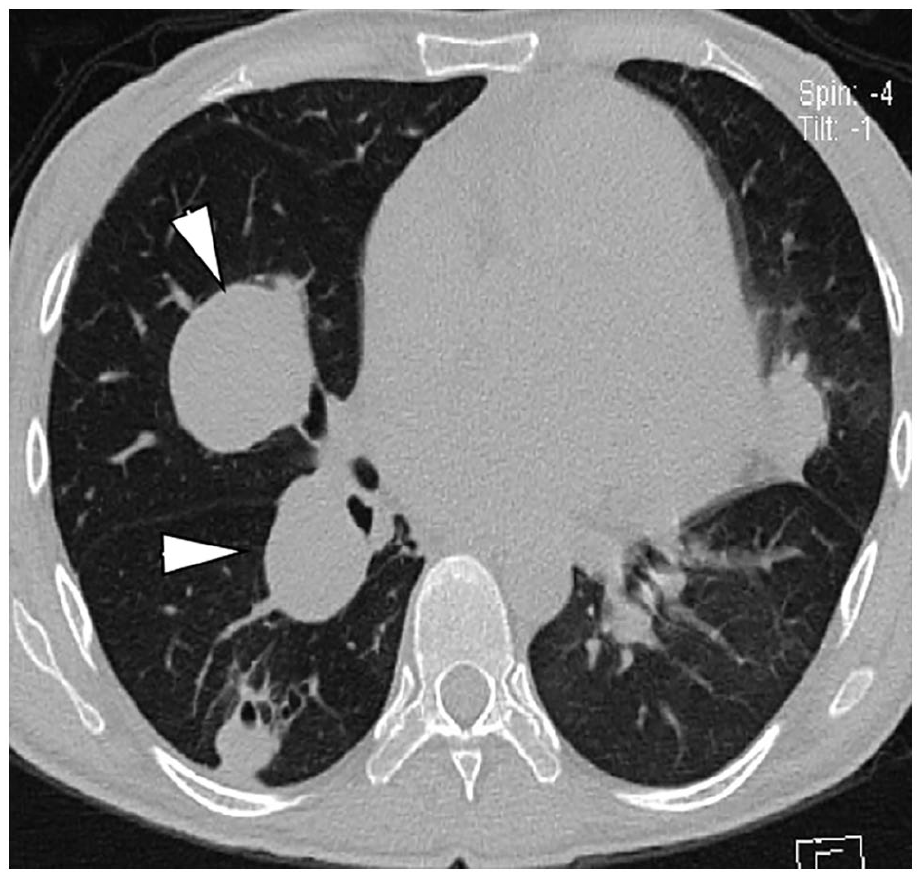
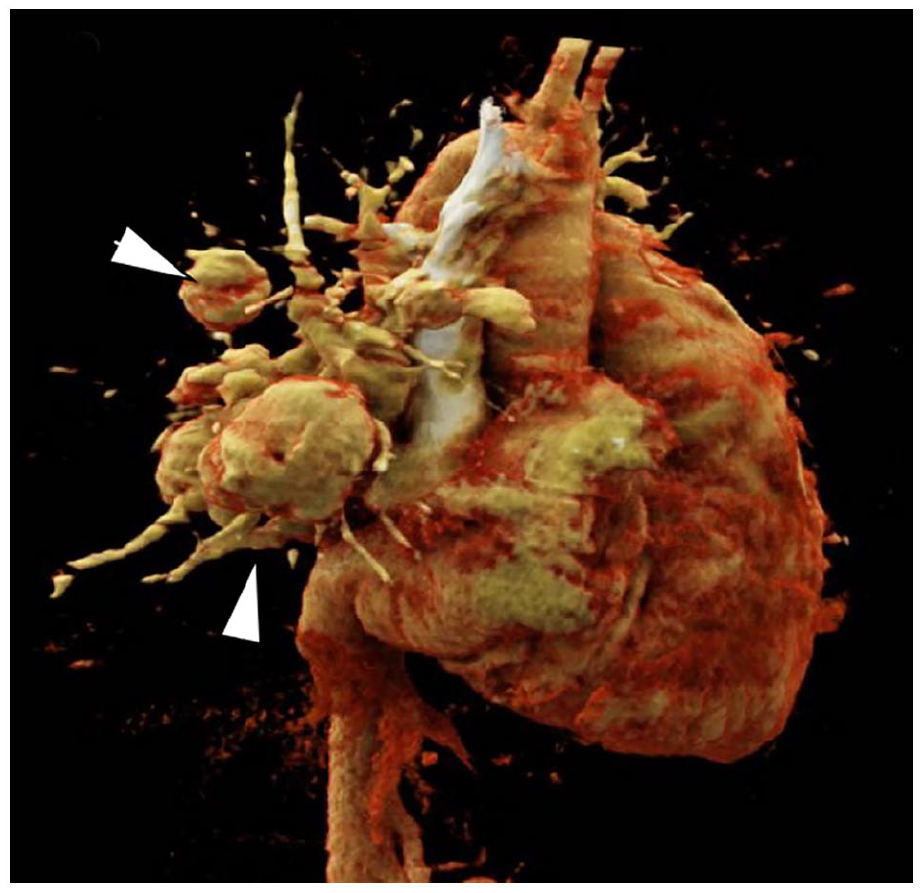
The presented images correspond to a 26-year-old female with no relevant history admitted for dyspnea and recurrent epistaxis. Physical examination showed decreased respiratory rate and bilateral crackles. The heart was in regular sinus rhythm, with a rate of 110 beats per minute. Chest x-ray showed a right rounded opacity. Axial CT using bone window depicted bilateral, pericardial RA (Panel A; arrowheads), with adjacent bronchiectasis and absence of lung cavitation. CT angiography with 3D reconstruction confirmed multiple rounded RA (Panel B; arrowheads).
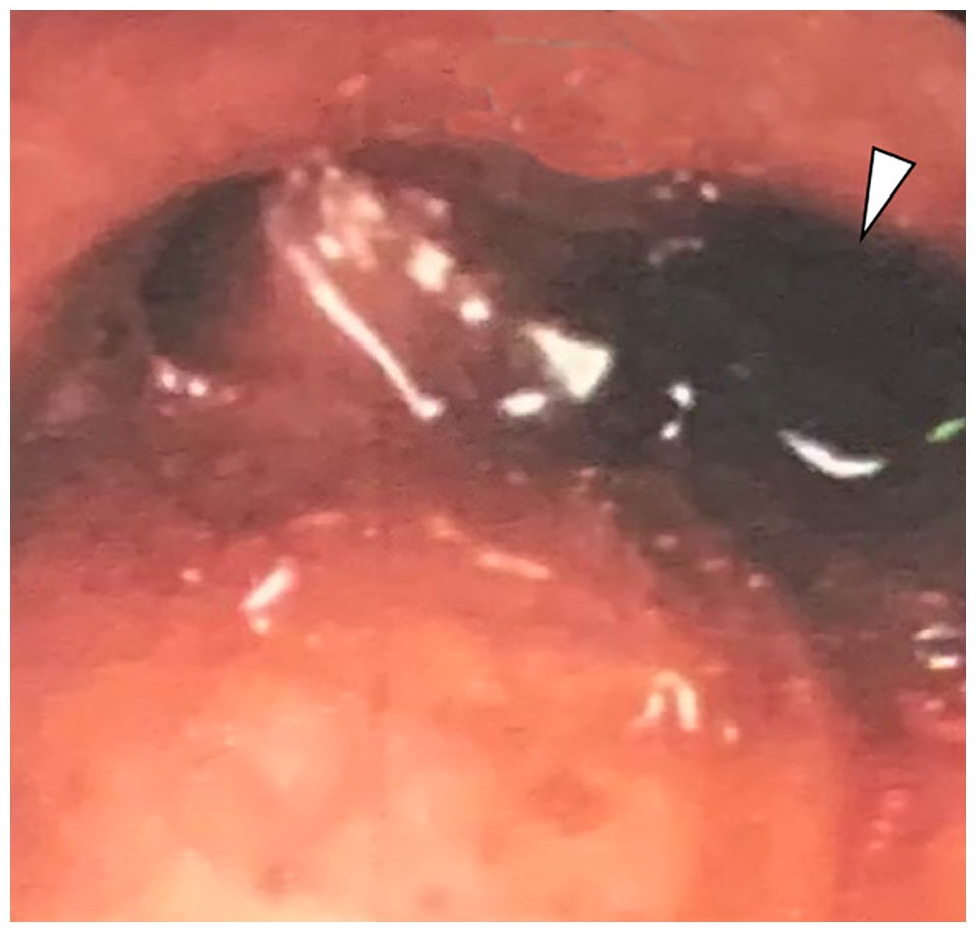
During her admission, hemoptysis quantified 900 mL/24 h, which led to bronchoalveolar lavage. Fiberoptic bronchoscopy showed a hemorrhagic clot in the left basal trunk (Panel C; arrowhead). GeneXpert was used for drug susceptibility testing for TB diagnosis and strain resistance level according to World Health Organization (WHO) recommendations 3 ; it detected TB and identified rifampin-resistant strains. The patient underwent pulmonary arteriography with right bronchial embolization; control arteriography showed corrected devascularization.
Clinicians should consider the occurrence of Rasmussen aneurysms in highly endemic TB settings. This case reminds us that hemoptysis can be an emergency in patients with tuberculosis, whether or not it is drug-resistant. 1 Helpful information for the diagnosis can be provided by 3D CT angiography evincing the aneurysm; it should be done before artery embolization so that pulmonary bleeding can be differentiated from systemic bronchial bleeding. 4 The management should be done by a multidisciplinary team (critical care medicine, pneumology, infectious diseases, radiology).
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.