
Abstract
In honor of Dr. Jay D. Coffman (1928–2006), distinguished internist and researcher of vascular medicine and clinical cardiology, SVM sponsors an annual award in vascular medicine and biology research. The top finalists make oral presentations during the Jay D. Coffman Young Investigator Presentation, which will be held on Saturday, September 11, at 9:15 am Eastern Time (ET). The winner of the Jay D. Coffman Young Investigator Award will be announced during the Awards Ceremony on Saturday, September 11, at 3:45 pm ET.
Authors will give poster presentations on Thursday, September 9, at 5:00 pm ET.
For more information about the meeting visit: https://vascularmed.confex.com/vascularmed/2021/prelim.cgi/Home/0.
Jay D. Coffman Young Investigator Award (YIA) Presentations
YIA 1215
Creatine chemical exchange saturation transfer MRI to evaluate calf muscle energetics in peripheral artery disease
1University of Virginia, Charlottesville, VA; 2Cone Health Medical Group, Greensboro, NC; 3Piedmont Healthcare, Atlanta, GA
Background: Diagnostic studies of peripheral artery disease (PAD) are frequently limited by inconsistency between hemodynamic parameters and functional capacity leading to the development of modalities focused on examining muscle energetics instead of blood flow. Creatine chemical exchange saturation transfer (CrCEST), a novel MRI technique, utilizes radiofrequency pulses to monitor creatine concentrations at high spatial resolution. The goal of this study is to utilize CrCEST kinetics to compare post-exercise creatine decay in patients with PAD to that of normal subjects.
Methods: 19 subjects with known PAD were compared with 15 healthy subjects. All subjects underwent an MRI on a 3T Siemens Prisma scanner. Baseline pre-exercise images were obtained, followed by plantarflexion ergometry using Ergospect (Innsbruck, AU) until calf exhaustion, at which point post-exercise images were obtained. CrCESTasym decay maps were obtained with a region of interest (ROI) drawn around the anterior tibialis, posterior tibialis, and gastrocnemius muscles. Creatinine decay times were compared using the Wilcoxon rank sum test.
Results: 19 subjects with confirmed PAD (mean ABI 0.69 ± 0.09) had prolonged median overall calf muscle creatine decay time of 276 seconds (s) (IQR 178 to 375 s) versus 148 s (IQR 108 to 189 s) in controls, p = 0.033. In addition, differences in the median creatine decay times for individual muscle groups were also observed. The gastrocnemius muscle demonstrated a creatinine decay time of 316 s in PAD (IQR 135 to 497 s) versus 178 s in controls (IQR 106 to 251, p = 0.03 and similarly, the posterior tibialis muscle, 186 s (IQR 18 to 354 s) versus 116 s (IQR 60 to 172), p = 0.03.
Conclusions: CrCEST can be utilized to distinguish creatine kinetics in PAD and normal subjects, as patients with PAD demonstrated a significant prolongation in overall creatine decay times post-exercise compared to healthy subjects. These differences in creatine kinetics are further demonstrated in individual muscle groups, illustrating the high spatial resolution of this technique. Future studies will compare this technique to phosphocreatine recovery kinetics by 31P spectroscopy and compare muscle energetics to perfusion.
YIA 1293
Tie2 activation protects against prothrombotic endothelial dysfunction in COVID-19
1Beth Israel Deaconess Medical Center, Boston, MA; 2Ragon Institute of MGH, MIT and Harvard, Boston, MA
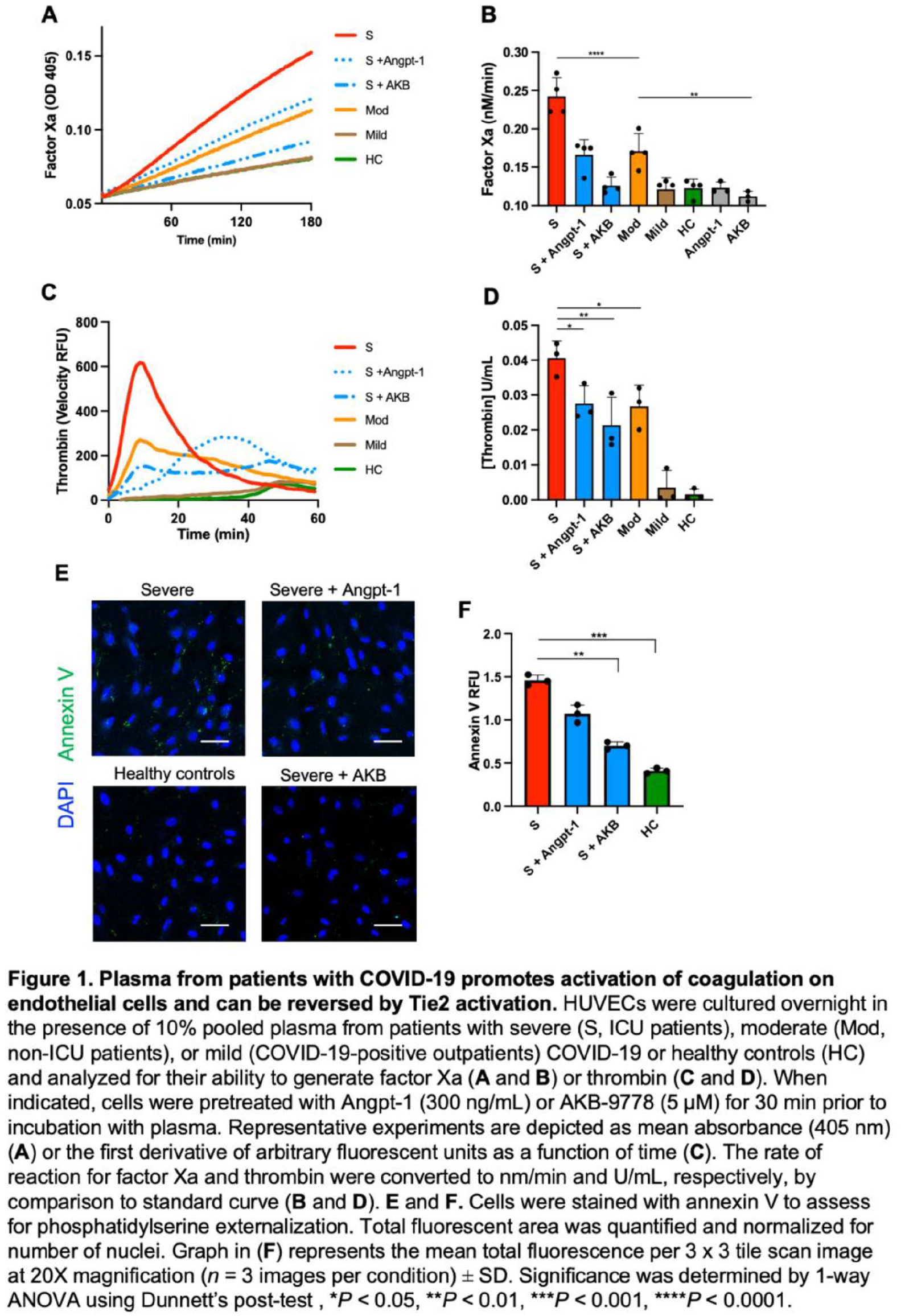
Background: We assessed whether severe COVID-19 is associated with procoagulant dysfunction of the endothelium and if activation of the Tie2 receptor can reverse this phenotypic change.
Methods: We treated primary human endothelial cells with plasma from patients with COVID-19 and analyzed for thromboinflammatory gene expression and activation of coagulation on the endothelial surface. We measured circulating endothelial markers in a cohort of 98 patients with COVID-19.
Results: Plasma from patients with severe COVID-19 resulted in a thromboinflammatory gene expression changes and promoted coagulation on the endothelial surface. Activation of Tie2 with the small molecule AKB-9778 reversed the endothelial procoagulant changes induced by COVID-19 plasma. On lung autopsy specimens, we found a prothrombotic endothelial signature as evidenced by increased von Willebrand Factor and loss of anticoagulant proteins. Assessment of circulating endothelial markers in a cohort of patients with COVID-19 revealed profound endothelial dysfunction indicative of a prothrombotic state. Angoppoietin-2 concentrations rose with increasing disease severity and highest levels were associated with worse survival. See Figure.
Conclusion: These data highlight the procoagulant changes in endothelial cells in severe COVID-19. Our findings provide novel rationale for current trials of Tie2 activating therapy with AKB-9778 in severe COVID-19.
YIA 1293 Figure.
YIA 1374
Efficient suppression of vascular smooth muscle cell proliferation and intimal hyperplasia by targeting phosphodiesterase 10A
1Department of Surgery, Stanford University, Stanford, CA; 2Aab Cardiovascular Research Institute, University of Rochester, Rochester, NY; 3Vascular Biology Center, Augusta University, Augusta, GA
Background: Accumulation of vascular smooth muscle cell (SMC)-like cells is a major contributor to intimal hyperplasia. Our preliminary screening for dysregulated cyclic nucleotide phosphodiesterases (PDEs) in proliferative vascular SMCs identified a significant change in PDE10A expression; hence, we aimed to reveal the potential function of PDE10A in SMC proliferation and neointimal formation.
Methods: Real-time RT-qPCR, immunoblotting, immunohistochemistry, and in situ proximity ligation assay were used to determine the PDE10A level in cultured SMCs and injured arteries. Cell counting, BrdU incorporation, and flow cytometry were performed on cultured SMCs to evaluate the effects of PDE10A deficiency on SMC growth. The involvement of the cGMP signaling pathway was examined by knocking down specific protein components. To determine the pathological function of PDE10A and the therapeutic value of its inhibition, the mouse femoral artery wire injury model was performed in wild type and PDE10A knockout mice, as well as in mice treated with vehicle or a PDE10A specific inhibitor, MP-10 (PF-2545920). Besides, MP-10 was also used in an ex vivo organ bath model of human saphenous vein (HSV) segments.
Results: We observed PDE10A mRNA and/or protein levels were largely up-regulated in cultured SMCs especially with growth stimuli and in the neointima of injured mouse arteries. PDE10A silencing by shRNAs and inhibition by MP-10 both induced G1/S cell cycle arrest in cultured SMCs with a decrease in the cyclin D1 protein level. Interestingly, the anti-mitotic effects of PDE10A inhibition were compromised by targeting cGMP-dependent protein kinase Iα (PKGIα), natriuretic peptide receptor 2 (NPR2), or natriuretic peptide precursor C. PDE10A depletion or MP-10 administration effectively attenuated intimal thickening in injured mouse femoral arteries. Moreover, PDE10A inhibition significantly suppressed cell proliferation and ex vivo remodeling of cultured HSV samples.
Conclusion: Our results suggest PDE10A promotes SMC proliferation and intimal hyperplasia through regulating NPR2/cGMP/PKGIα signaling; hence it can be a promising drug target for treating vascular occlusive disorders.
Poster Presentations
1223
The efficacy and safety of dual-pathway inhibition therapy among patients with peripheral artery disease: A meta-analysis
Philippine General Hospital, Manila, Philippines
Background: Peripheral artery disease (PAD) affects more than 200 million people worldwide and it is associated with an increased risk for cardiovascular morbidity and mortality. Current recommendations regarding the management of PAD have been controversial. Our meta-analysis investigated the efficacy of direct Xa inhibitor plus antiplatelet, also known as dual-pathway inhibition (DPI), on the individual components of major adverse cardiovascular events (stroke, myocardial infarction, and cardiovascular death) and major adverse limb events (amputation, restenosis, revascularization, and acute limb ischemia), the composite of MACE and MALE and its safety, in terms of bleeding, compared to antiplatelet therapy among patients with PAD.
Methods: We performed a random-effects meta-analysis among patients with PAD comparing DPI to antiplatelet therapy. PubMed, EMBASE, CENTRAL, and ClinicalTrials.gov were searched from their dates of inception to August 2020 for Randomized Controlled Trials. Three studies met the inclusion criteria for final analysis. The selected studies were assessed for risk of bias using the Cochrane RoB2 tool and the overall quality of evidence was assessed using the GRADE approach.
Results: Among patients with PAD, DPI significantly reduces the risk of adverse limb events excluding amputation (RR 0.69, 95% CI 0.57-0.83) and composite MACE and MALE (RR 0.80, 95% CI 0.69-0.93) but significantly increases risk of major bleeding (RR 1.43, 95% CI 1.06-1.93) compared to antiplatelet therapy alone. Overall, DPI did not reduce myocardial infarction, stroke, cardiovascular death, or amputation, or increase the risk of fatal bleeding.
Conclusions: Among patients with PAD, DPI is more effective than antiplatelet therapy alone in preventing adverse limb events excluding amputation with an increased risk of major bleeding. We recommend the use of DPI among patients with PAD who are at a low risk of bleeding.
1265
Characteristics and management of type A acute aortic syndromes at a single academic medical center: insights from the code aorta registry
1Brigham and Women’s Hospital, Boston, MA; 2Georgetown University School of Medicine, Washington DC; 3University of Santo Amaro, São Paulo, Brazil
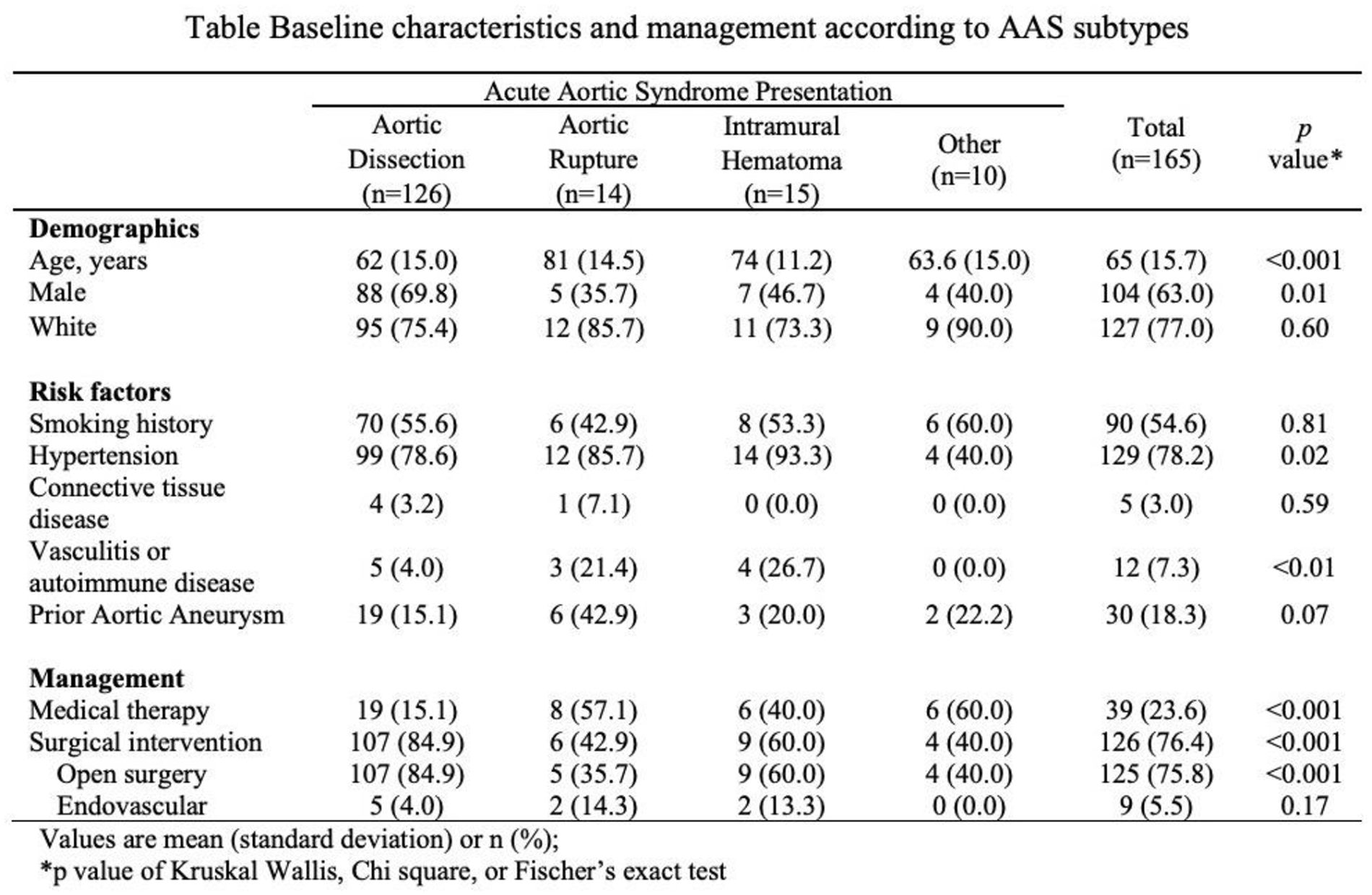
Background: Acute aortic syndromes (AAS) involving the ascending aorta (Stanford type A) are life-threatening emergencies. Management may vary between subtypes of type A AAS.
Methods: We conducted a retrospective analysis of all patients admitted to our tertiary medical center with type AAS between July 2012 and October 2020. Type A AAS presentations included aortic dissection, intramural hematoma (IMH), aortic rupture, and others (symptomatic aneurysm, penetrating aortic ulcer, and pseudoaneurysm).
Results: A total of 165 patients with type A AAS were admitted to the hospital and included in the analyses. Patients were predominantly male (63.0%) and white (77.0%), with a mean age of 65 years. The most frequent presentation of AAS was aortic dissection (76.7%), followed by IMH (9.2%), aortic rupture (8.6%), and others (5.5%). Demographic characteristics, risk factors, and management are reported in the Table. The majority of patients underwent surgical repair (76.4%), whereas the remaining were treated medically (23.6%). Patients with aortic rupture were more likely to undergo medical treatment compared with those with dissection (57.1% vs 15.1%, p < 0.001). The in-hospital mortality rate for the cohort was 20.3%.
Conclusion: Among patients with type A AAS, those with aortic rupture were more likely to be medically treated compared with those with dissection.
Poster 1265 Table.
1272
Do statins impact long-term mortality peripheral artery disease patients who have end stage renal disease?
University of Kansas Medical Center, Kansas City, KS
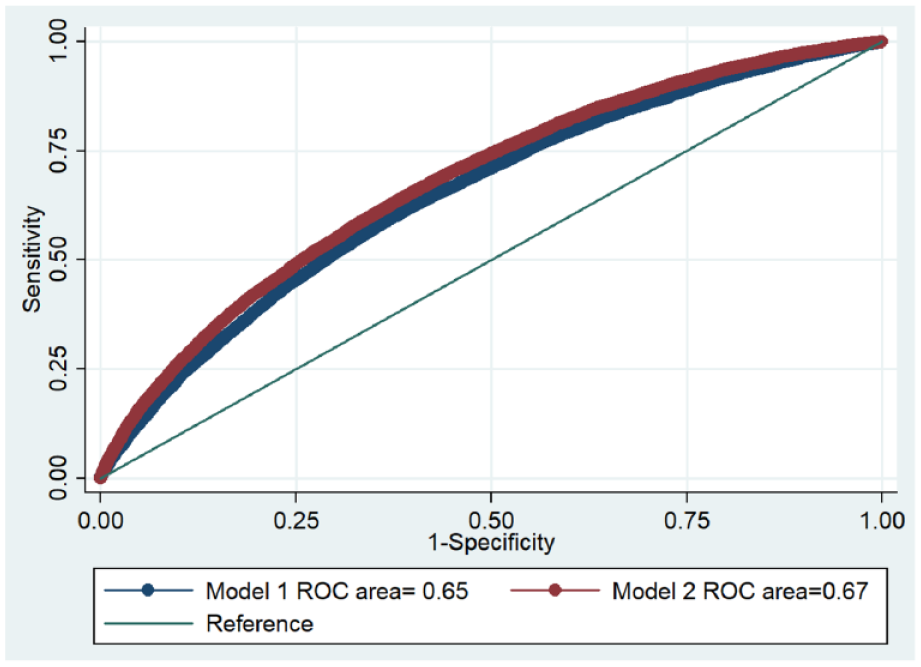
Background: Statins have shown mortality benefit in peripheral artery disease (PAD), their impact in end stage renal disease (ESRD) patients with PAD is not well studied.
Methods: We included ESRD Medicare beneficiaries from United states Renal Database (Jan 1st, 2006, to May 31st, 2017) with PAD within 6 months of incident dialysis. Medicare part D claims were used to determine STU during the follow up period. Fractional polynomial regression across varying % of STU was generated to predict 2-year mortality.
Results: Out of 45,424 ESRD patients with PAD, 62.3% received no statins while rest had at least some duration of STU. ST was bimodally distributed, with median utilization of 0% (IQR 0–90%). Mortality was 41.7% over a median follow up of 472 days. Univariate association of STU on mortality yielded odds ratio (OR) of 0.99 (95% CI = 0.992–0.993; p < 0.001). Model 1 including baseline demographics and comorbidities (age, sex, body mass index, hypertension, coronary artery disease, stroke, smoking, diabetes, and heart failure) an AUC 0.65. Addition of STU (Model 2) resulted in only minimal improvement in the AUC (0.65 vs 0.67; p < 0.01). See Figure.
Conclusion: Statin utilization in ESRD patients is associated with only borderline statistically significant reduction in mortality (≈ 0.1%) of unclear clinical implications.
Poster 1272 Figure.
1278
Exercise characteristics associated with improved walking performance in peripheral artery disease: the lite randomized clinical trial
1Northwestern University, Chicago, IL; 2Stanford University, Palo Alto, CA
Background: The LITE randomized trial reported that walking exercise that induced ischemic leg symptoms, but not walking exercise conducted at a comfortable pace, significantly improved walking performance in people with peripheral artery disease (PAD). Using data from the LITE trial, this report describes associations of greater exercise intensity and duration of walking exercise with improvement in six-minute walk distance (6MW) in people with PAD
Methods: In a multi-centered clinical trial, 305 participants with PAD were randomized (69±40 years, 181 (59%) black, 146 (48%) female) to low intensity walking exercise (conducted at a pace without ischemic leg symptoms), high intensity walking exercise (conducted at a pace eliciting moderate-severe leg symptoms), or an attention-control for 12-months. Both exercise interventions were home based. Participants were asked to walk for up to five days/week for up to 50 minutes/session at either a pace eliciting ischemic leg symptoms (high intensity) or at a pace without ischemic leg symptoms (low intensity). Participants in each exercise group were categorized into quartiles according to exercise minutes per week and exercise intensity, respectively (fourth quartile indicated greatest minutes or intensity).
Results: Within the low and high intensity exercise groups, greater walking exercise minutes/week were associated with greater 6MW improvement [(low intensity: -37, +6, +11, +18 meters across quartiles 1-4, P trend < 0.01), (high intensity: -13, -16, +10, +41 meters across quartiles 1-4; P trend < 0.01)]. Within the low intensity exercise group but not the high intensity group, greater exercise intensity was associated with greater 6MW improvement [(low intensity: -39, +2, +8, +41 meters across quartiles 1-4; P < 0.01), (high intensity: +18, +47, +72. +56 meters across quartiles 1-4; P = 0.141)].
Conclusion: Among people with PAD who exercise without ischemic leg symptoms, more minutes of exercise/week and greater exercise intensity were associated with greater 6MW improvement. Among patients with PAD who exercise at a pace inducing ischemic leg symptoms, greater exercise minutes per week, but not greater exercise intensity, improved 6MW.
1296
Association of polyvascular disease with adverse outcomes after percutaneous coronary intervention
1Dartmouth-Hitchcock Medical Center, Lebanon, NH; 2Maine Medical Center, Portland, ME; 3Catholic Medical Center, Manchester, NH; 4University of Vermont Medical Center, Burlington, VT; 5Eastern Maine Medical Center, Bangor, ME; 6Concord Hospital, Concord, NH
Background: The co-existence of coronary artery disease (CAD) and peripheral artery disease (PAD) or cerebrovascular disease (CVD), termed polyvascular disease, is associated with a higher risk of adverse outcomes than either condition alone. We examined the association of polyvascular disease with adverse outcomes in patients undergoing percutaneous coronary intervention (PCI).
Methods: Using the Northern New England Cardiovascular Disease Study Group database, patients undergoing PCI between 2005 and 2015 were stratified by CAD alone; CAD and PAD or CVD; and combination of CAD, PAD and CVD. Adjusted regression models and propensity matched cohorts were built to determine the association of polyvascular disease with adverse outcomes.
Results: Compared to CAD alone, patients with CAD and vascular disease were older, more likely to be female, with higher prevalence of comorbidities, and more extensive CAD. In multivariable analysis, polyvascular disease was independently associated with both 30-day and long-term all-cause mortality, with incremental increase in risk with more vascular beds involved. In propensity-matched cohort, polyvascular disease was associated with higher risk of bleeding complications, longer length of stay, and 30-day and long-term all-cause mortality.
Conclusion: Polyvascular disease is independently associated with higher risk of peri-procedural complications, as well as 30-day and long-term all-cause mortality. Aggressive secondary risk prevention measures (e.g., lipid lowering therapies in combination with high intensity statin, extended dual-antiplatelet therapy, or adjunctive low-dose rivaroxaban) should be more routinely considered for these patients.
1302
Hemodynamic changes according to the clinical stages of chronic venous disease
1Department of Ultrasound, Xijing Hospital, Xian, China; 2University of California, Davis, Vascular Center, Sacramento, CA
Background: Hemodynamic changes according to clinical stages of chronic venous disease (CVD) from the Eastern Hemisphere have not been extensively analyzed. We intend to compare clinical severity using CEAP-VCSS-HASTI and duplex ultrasound parameters.
Methods: From 2017 to 2020, consecutive CVD patients with primary venous reflux were categorized according to the CEAP classification. The vein diameter and reflux time were documented in the superficial, the deep and the calf perforator veins. VCSS and HASTI were assessed and analyzed. P < 0.05 was considered statistically significant.
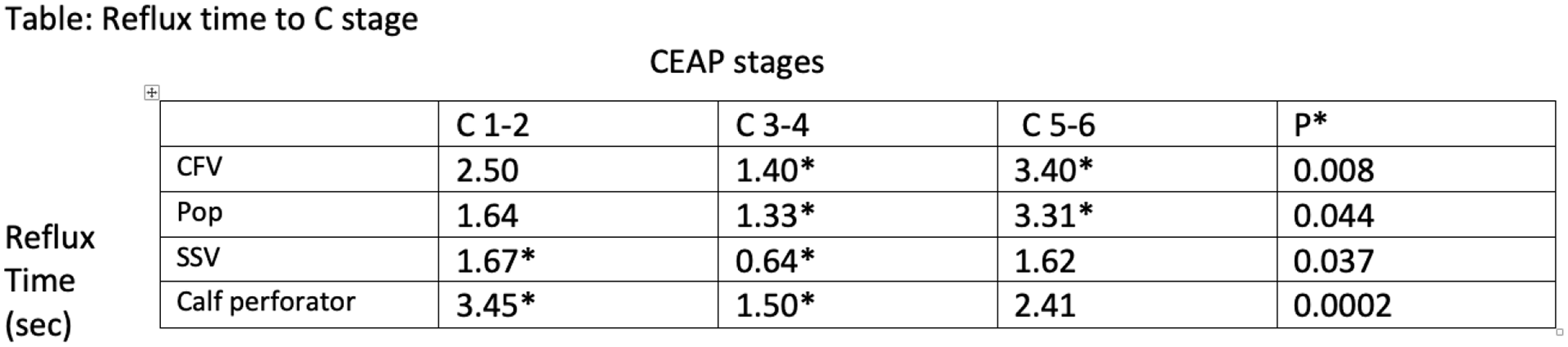
Results: 507 consecutive patients (243 female) with 521 limbs of primary venous reflex were studied. The mean age was 52.5 years. HASTI differed significantly between C1-2 and C3-4, but the power faded between C3-4 and C5-6. VCSS score was strongly discriminate from C1-C6. In combined superficial-deep reflux cases, longer reflux time (RT) in deep veins were observed in C5-6 compared to C3-4 (Table). In superficial-perforator reflux cases, the RT in small saphenous vein and calf perforator vein (CPV) were prolonged in C1-2 compared to C3-4 (Table) but a larger CPV diameter was observed in C3-4 (C1-2 CPV diameter = 3.80 mm, C3-4 CPV diameter = 4.74 mm; P = 0.034).
Conclusions: This analysis is one of the few epidemiological studies on CVD in China focusing on the relationship between duplex hemodynamics and clinical scores. HASTI was discriminative from C1-C4 while VCSS from C1-C6. Both scores increased when deep venous reflux present.
Poster 1302 Table.
1303
Association of clinical setting with sociodemographics and outcomes following endovascular femoropopliteal artery revascularization
1Division of Cardiology, Richard A. and Susan F. Smith Center for Outcomes Research in Cardiology, Department of Medicine, Beth Israel Deaconess Medical Center, Boston, MA; 2Harvard Medical School, Boston, MA
Background: Peripheral vascular intervention (PVI) has increasingly been performed in privately-owned office-based clinics after modification of reimbursement in 2008. It is not known how this shift influenced the care of patients of minority race and lower socioeconomic status (SES).
Methods: Medicare beneficiaries ⩾ 66 years undergoing femoropopliteal PVI between 4/1/15-12/31/17 in office-based clinics and hospital-based outpatient centers, and 10/1/15-12/31/17 in inpatient centers were identified. Sociodemographics, comorbidities and institutional characteristics were compared. Cox proportional hazard models were used to estimate unadjusted and adjusted associations between variables and outcomes. Outcomes included amputation-free survival (AFS) and death.
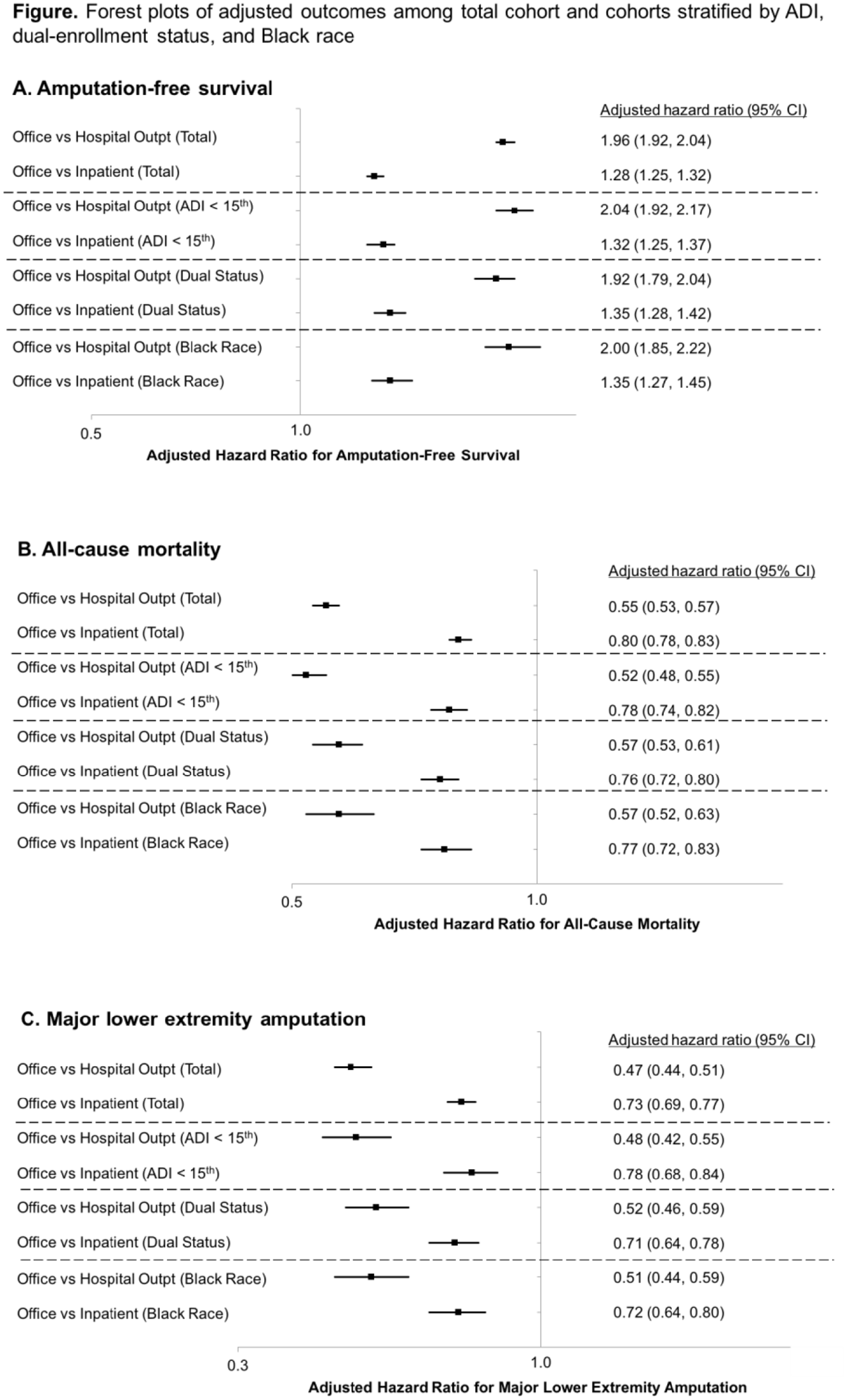
Results: Of 185,533 patients, 21% were treated in office-based clinics, 51% in hospital-based outpatient centers and 27% in inpatient centers. Mean age was 77 years, 45% were female and 80% were White. Patients treated in office clinics were more often Black, dually-enrolled and residing in lower resourced regions. After adjustment, patients treated in office-based clinics had higher AFS. These findings persisted after stratifying by race, dual enrollment, and regional SES. See Figure.
Conclusions: Office-based clinics performed PVI on a more socioeconomically disadvantaged population but have better outcomes. The marked differences in patient sociodemographics underscores the need to monitor quality and access to care.
Poster 1303 Figure.
1305 - withdrawn
1317
Outcomes of complete decongestive therapy in patients with lymphedema enrolled in the vascular and lymphedema center of the Makati Medical Center, Philippines
Makati Medical Center, Makati, Philippines
Background: Lymphedema is the abnormal accumulation of protein-rich fluid in soft tissues, results from a dysfunction of the lymphatic system. It is a prevalent and potentially debilitating disease that affects millions of people worldwide. This study aimed to determine the outcomes of patients undergoing Complete Decongestive Therapy (CDT) in the Vascular and Lymphedema Center (VLC) of Makati Medical Center (MMC), Philippines.
Methods: This was a retrospective study. This study included all patients with lymphedema undergoing CDT at the VLC of MMC from 2019 to December 2020. Patients more than 18 years old with diagnosis of either primary or secondary lymphedema were included in this study. Chart review was done from the patients’ chart provided by the unit. Limb volume excess (EV), percent volume excess (PEV), percent reduction in excess volume (PREV) for unilateral lymphedema, and percent reduction in absolute volume (PRAV) for bilateral lymphedema were calculated.
Results: A total of 54 patients were included in the study. Twenty four of the patients had unilateral UE lymphedema, while 30 patients had unilateral/bilateral LE lymphedema. More than half of the patients were more than 60 years old and mostly were females. Mean EV and PEV of the affected limbs on the UE after the CDT was significantly lower than before undergoing CDT (p = 0.0001 and p = 0.0001). There was a significant reduction of unilateral LE lymphedema in terms of EV and PEV before and after CDT (p = 0.0023 and 0.0035). There was also statistically significant reduction in limb volume of bilateral LE lymphedema (p < 0.001). Weight reduction and QOL of patients before and after CDT was statistically significant in both UE (p = 0.006 and 0.0001) and LE (p < 0.0001 and p < 0.0001). Univariable analysis showed no evidence to conclude significant association between demographic and clinical characteristics with lymphedema reduction.
Conclusions: CDT significantly reduce lymphedema volume and significantly improve QOL of patients suffering from any cause of lymphedema. Effect of CDT in terms of volume reduction is not affected or influenced by any demographic and clinical characteristics.
1320
Combination antithrombotic therapy and bleeding risk: comparing atrial fibrillation and venous thromboembolism
1University of Michigan, Ann Arbor, MI; 2Beaumont Hospital, Royal Oak, MI; 3Detroit Medical Center, Detroit, MI; 4Henry Ford Hospital, Detroit, MI
Background: Existing studies regarding combination anticoagulant-antiplatelet management have focused on patients with atrial fibrillation (AF). It is unknown if the combination of anticoagulant-antiplatelet therapy presents a comparable risk of bleeding for patients with venous thromboembolism (VTE).
Methods: Adult patients initiating warfarin at six anticoagulation clinics in Michigan from 2009 to 2020 were enrolled via a registry-based cohort study. Participants were stratified based on sole indication for anticoagulation: AF or VTE. Two propensity score-matched cohorts were generated based on demographics, comorbidities, antiplatelet use, and follow-up time. Survival analysis and Cox proportional hazards were used to examine adverse events.
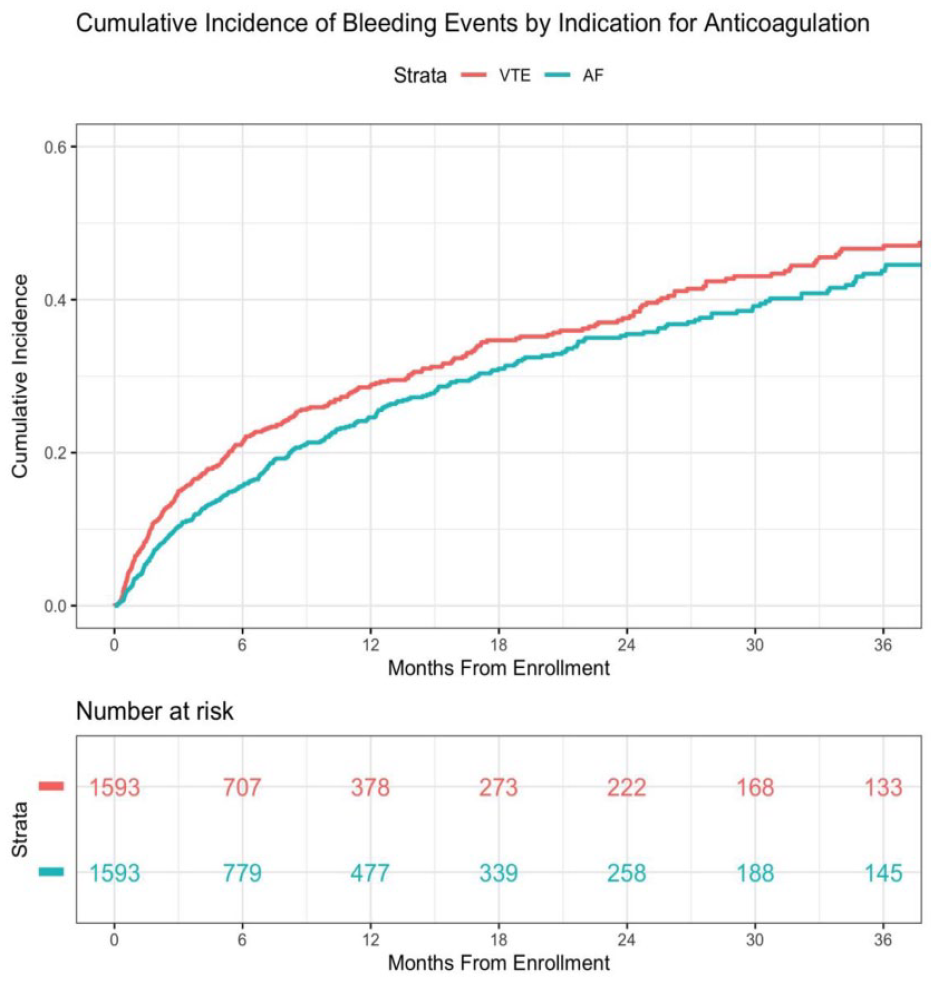
Results: Propensity score matching generated two well-balanced cohorts of 1593 patients each. Bleeding risk was significantly higher in patients treated for VTE compared to AF (see Fig.). After adjusting for the number of antiplatelet agents, being anticoagulated for VTE remained significantly associated with increased bleeding risk (hazard ratio: 1.23; 95% CI: 1.08-1.42).
Conclusion: Patients anticoagulated for VTE have a significantly higher bleeding risk compared to similarly matched patients with AF. As most guidelines regarding antithrombotic management have focused on patients with AF, further research is needed to tailor these recommendations to the unique VTE population.
Poster 1320 Figure.
1322
Knowledge, attitude, and practices of physicians on anticoagulation among patients admitted with COVID-19 in the Philippines
Jan Patrick Ng, Jasmin Melissa Bernardo
Makati Medical Center, Makati, Philippines
Background: Coronavirus disease-19 (COVID-19) is a global pandemic caused by SARS-CoV-2. One of the salient features of the disease is the propensity towards a hypercoagulable state. Incidence rate of venous thromboembolism (VTE) was as high as 69% in ICU patients with COVID-19. The Philippine Society of Vascular Medicine (PSVM) developed its interim guidelines in anticoagulant management of patients with COVID 19 last April 2020. This study aimed to assess the knowledge, attitude, and practices of local physicians in anticoagulant management of COVID 19 patients in Tertiary Hospitals in the Philippines.
Methods: This was a prospective study conducted in major Tertiary Hospital in the Philippines. Physicians who managed admitted confirmed COVID-19 patients were included in this study. Respondents were given a link via e-mail or an encrypted messenger platform which was directed to an encrypted site containing the questionnaire. Questions were categorized under the domain of knowledge, attitude, or practices.
Results: A total of 106 respondents participated in this study. Two of the respondents were excluded because they were not able to handle patients with COVID-19. The mean age of the respondents was 35.9 years old. Consultants (51.9%) comprised majority of the respondents. Most of the respondents (90.3%) were able to handle more than five patients with COVID-19 and 82 (78.8%) of them were able to handle patients with moderate to severe COVID-19 patients. Seventy-six respondents were able to encounter COVID-19 patients who developed VTE. Only 72 of the respondents are aware of the PSVM guidelines regarding anticoagulation treatment of patients with COVID-19. Majority of the respondents scored ⩾ 5 (97.1%) with mean score of 7.7 for the knowledge domain, ⩾ 4 (94.2%) with mean score of 4.7 for attitude domain, and ⩾ 5 (53.8%) with mean score of 4.7 for the practice domain.
Conclusion: Most of the respondents have good knowledge and attitude towards anticoagulation on patients with COVID-19; however, respondents scored fairly on practice domain. This was probably due to the lack of awareness and compliance to the locally made guidelines. Better awareness and compliance to the guideline could help aide in the management of patients with COVID-19.
1326
Autoantibodies stabilize neutrophil extracellular traps in COVID-19
1University of Michigan, Ann Arbor, MI; 2National Heart, Lung and Blood Institute, Bethesda, MD
Background: The release of neutrophil extracellular traps (
Methods: Utilizing a novel anti-NET ELISA, we measured global anti-NET activity in 171 individuals hospitalized with COVID-19 alongside 48 healthy controls. Beyond the ELISA platform, we also assessed anti-NET activity by immunofluorescence microscopy. The ability of purified anti-NET IgG to degrade NETs was also assessed.
Results: We found high anti-NET activity in the IgG and IgM fractions of approximately 40% and 50% of patients, respectively. There was a strong correlation between anti-NET IgG and anti-NET IgM, with high anti-NET antibody levels in general associating with circulating markers of NETs such as myeloperoxidase-DNA complexes and calprotectin. Clinically, anti-NET antibodies tracked with impaired oxygenation efficiency and elevated levels of circulating D-dimer. Furthermore, patients who required mechanical ventilation had higher levels of anti-NET antibodies than those who did not require oxygen supplementation. Mechanistically, anti-NET antibodies of the IgG isotype impaired the ability of DNases in healthy serum to degrade NETs.
Conclusion: In summary, these data reveal high levels of anti-NET antibodies in individuals hospitalized with COVID-19, where they likely impair NET clearance and thereby potentiate SARS-CoV-2 mediated thromboinflammation.
1335
Prognostic interaction between age and sex on early and late outcomes following carotid endarterectomy for asymptomatic and symptomatic de-novo carotid stenosis
University Hospital of Trieste, Trieste, Italy
Background: The aim of this study was to assess the prognostic interaction between age and sex on peri-operative and follow-up outcomes following elective carotid endarterectomy (CEA) for asymptomatic and symptomatic carotid stenosis.
Methods: A retrospective review of all patients admitted to a single vascular unit who underwent elective CEA between January 2015 and December 2019 was performed. The primary endpoints of the study were overall survival (from index operation) cumulative stroke rate at thirty days, and major adverse cardiovascular events (MACE) during follow-up.
Results: A total of 383 consecutive patients were included in this study; of these 254 (66.4%) were males. At baseline, males were younger (mean age 73.4 ± 11 vs 76.3 ± 10 years, p = 0.01) and with lower proportion of octogenarians (20.4% vs 28.7%, p = 0.05). The rate of stroke in symptomatic and asymptomatic patients (males vs females) were as follows: a) whole cohort 1.9% vs 2% (p = 1.00) and 2.7% vs 1.3% (p = 0.66), respectively; b) ⩾ 80 years old 3.7% vs 0% (p = 1.00) and 4% vs 5.9% (p = 1.00), respectively; c) < 80 years old 1.2% vs 3.3% (p = 0.47) and 2.5% vs 0% (p = 0.55), respectively. The 3-year survival estimates were significantly lower for males (84% vs 92%, p = 0.03). After stratification by age groups, males maintained inferior survival rates in the strata aged < 80 years (85% vs 97%, p = 0.005), while no differences were seen in the strata aged ⩾ 80 years (82% vs 79%, p = 0.92). Using multivariate Cox proportional hazards, age (HR 2.1, 95% CI 1.29-3.3, p = 0.002) and male sex (HR 2.5, 95% CI 1.16-5.5, p = 0.02) were associated with increased hazards of all-cause mortality. No significant differences were seen between males and females, in the whole cohort as well as after age stratification, in freedom from MACE at 3 years (males: 81% vs females 90%, p = 0.142).
Conclusions: In this study of elective CEA for asymptomatic and symptomatic carotid stenosis, similar peri-operative neurologic outcomes were found in both males and females irrespective of age. Despite being usually older, females have superior long-term survival rates.
1336
Pre-operative chronic kidney disease is associated with worse short-term and mid-term outcomes in patients undergoing fenestrated-branched endovascular repair for pararenal and thoracoabdominal aortic aneurysms
University of Uppsala, Uppsala, Sweden
Background: The purpose of this study was to review our experience with fenestrated-branched endovascular aortic repair (F-BEVAR) for pararenal/thoracoabdominal aortic aneurysms (PRAA/TAAA) and assess the association of pre-operative chronic kidney disease (CKD) with post-operative outcomes.
Methods: All consecutive patients undergoing (elective and non-elective) F-BEVAR at a single center (January 1, 2011 - July 1, 2019) were identified from a local database. Renal function was calculated as the estimated glomerular filtration rate (eGFR) using the Modification of Diet in Renal Disease formula. Accordingly, presence of CKD was defined as eGFR<60ml/min/1.73m2.
Results: Overall, 202 consecutive patients (mean age 72 ± 8 years; 25% females) underwent F-BEVAR for treatment of PRAA/TAAA during the study period. Of these, 51 had history of CKD (none on chronic hemodialysis). No significant differences were found in demographics and major comorbidities between patients with or without history of CKD. The overall perioperative mortality rate was 2%, without significant differences between study groups (p = 0.26). Patients with prior CKD had significantly higher rates of AKI (37% vs 12%, p < 0.001). At 3 years, overall survival was significantly lower in patients with history of CKD as compared to those without preoperative CKD (57% vs 82%, p = 0.01). Similarly, freedom from renal function decline at three years was significantly poorer in patients with prior history of CKD as compared to those without preoperative CKD (43% vs 80%, p = 0.02). In a multivariable analysis CKD was independently associated with higher odds of perioperative AKI (OR 2.8, 95% CI 1.9-5.8, p = 0.03), renal function decline (OR 4.9, 95% CI 1.7-9.2, p = 0.003), and all-cause mortality (HR 3.2, 95% CI 1.2-8.6, p = 0.02).
Conclusions: Despite low rates of peri-operative mortality that are comparable to patients with unimpaired renal function, occurrence of AKI was significantly higher in subjects with preexisting CKD. History of CKD was independently associated to renal function decline and poorer mid-term survival.
1337
Long-term survival after repair of ruptured abdominal aortic aneurysms is improving over time - Nationwide analysis during twenty-four years in Sweden (1994-2017)
University of Uppsala, Uppsala, Sweden
Background: Management of ruptured abdominal aortic aneurysms (rAAA) has seen significant changes in the past decades, with the shifting from open (OAR) to endovascular (EVAR) being the most striking, thereby enabling treatment of elderly patients with multiple comorbidities. We sought to investigate long-term survival after rAAA repair in Sweden during a 24-year period (1994-2017).
Methods: A registry-based nationwide cohort study was performed, and three 8-year periods (1994-2001, 2002-2009, 2010-2017) were compared for crude long-term survival with Kaplan-Meier and multivariable Cox proportional hazards analyses. Relative survival compared to matched general population referents was estimated.
Results: Overall, 8,928 rAAA repair subjects were identified (1994-2001 N = 3,368; 2002-2009 N = 3,405; 2010-2017 N = 2,155). The proportion of octogenarians (20.6%; 27.5%; 34.0%; p < 0.001), women (14.3%; 18.5%; 20.6%; p < 0.001), and EVAR procedures (1.5%; 14.9%; 35.5%; P < 0.001) increased over time. The overall rate of 90-day mortality for entire cohort was 40.7%, with a significant decrease over time (first period: 46.4%; second period: 38.3%; third period: 35.6%; p < 0.001). The crude 5-year survival was 36%; 44%; 43% (p < 0.0001). Multivariable Cox proportional hazard analysis displayed a decreasing mortality hazard ratio (HR) over time (1.00; 0.80; 0.72; p < 0.001). Use of EVAR was associated with reduced hazards of crude long-term mortality (HR 0.80, P < 0.001). Relative survival for patients surviving the perioperative period (i.e., 90 days) was lower than matched general population referents and was stable over time (relative 5-year survival: 86% vs 88%, vs 86%, p < 0.001). Causes of late death were analyzed in those surviving > 90 days after the index repair. Overall, cardiovascular diseases and cancer were identified as the most incident causes of late mortality accounting for 34% and 21% of all events, respectively.
Conclusions: Nationwide analysis of long-term outcomes after repair of rAAA in Sweden for a 24-year period (1994-2017) has revealed that, despite changes in the baseline population characteristics as well as in the treatment strategy, long-term survival improved over time.
1339 - withdrawn
1343
Mean platelet volume and mean platelet volume/platelet count ratio as predictor of major limb amputation and in-hospital mortality in patients with critical limb ischemia
Philippine Heart Center, Quezon, Philippines
Background: Critical limb ischemia (CLI) is the most advance form of peripheral artery disease that leads to major limb amputation and is associated with significant morbidity and mortality. Platelets play a pivotal role in the pathogenesis of occlusive arterial disease. This study aims to determine the accuracy of admission MPV and MPV/PC ratio in predicting major limb amputation and in-hospital mortality in patients with CLI.
Methods: A retrospective cohort of 62 patients with CLI was done from June 2014 to December 2016 admitted at the Philippine Heart Center. Demographic and clinical characteristics as well as hemogram parameters were taken. Cut-off values for MPV and MPV/PC ratio were computed and correlated with major limb amputation and in-hospital mortality.
Results: Major limb amputation and in-hospital mortality were 45.2% and 6.4%, respectively. The computed cut-off values for MPV were > 7.8 (sensitivity 60.71%, specificity 61.76%, PPV 56.7%, NPV 65.6%, AUC 0.546) for amputation and > 7.7 (sensitivity 100%, specificity 50%, PPV 12.1%, NPV 100%, AUC 0.582) for in-hospital mortality. The cut-off values for MPV/PC ratio were > 0.023 (sensitivity 28.57%, specificity 26.47%, PPV 24.24%, NPV 31.03%, AUC 0.763) and > 0.018 (sensitivity 100%, specificity 31.03%, PPV 9.1%, NPV 100%, AUC 0.554) for amputation and in-hospital mortality, respectively.
Conclusion: The MPV and MPV/PC ratio are readily available parameters that can be used as risk stratification tools in patients with critical limb ischemia. In this study, MPV is only moderately sensitive and specific in predicting major limb amputation and has a very low sensitivity and specificity in predicting in-hospital mortality. On the other hand, MPV/PC ratio showed good sensitivity with moderate specificity in predicting major limb amputation, and it also showed good sensitivity but low specificity in predicting in-hospital mortality.
1358
Long-term outcomes after superficial femoral artery revascularization in the elderly
1VA Boston Healthcare System, West Roxbury, MA; 2University of Pittsburgh, Pittsburgh, PA; 3Brigham and Women’s Hospital, Boston, MA; 4Central Maine Medical Center, Lewiston, ME; 5Medical University of South Carolina, Charleston, SC
Background: The risks of superficial femoral artery (SFA) endovascular revascularization for claudication or critical limb ischemia in elderly patients are uncertain. We assessed long-term outcomes in patients having SFA endovascular revascularization in 2 institutions to assess whether outcomes in the elderly were worse than younger patients.
Methods: All patients having SFA endovascular revascularization for lifestyle limiting claudication or critical limb ischemia by the Cardiovascular Divisions of the VA Boston Healthcare System and the Brigham and Women’s Hospital between 2003 and 2010 were followed by chart review for death, and adverse limb events of repeat revascularization and limb amputation. The national and VA death indices were also searched. Age was divided into three groups (65 years or less, > 65 years to 75 years, and over 75 years). The hazard ratio and 95% confidence interval (HR, 95%CI) of death and adverse limb events were assessed by characteristics at the index procedure by Cox proportional hazard models clustered by patient.
Results: 153 patients with index SFA endovascular interventions in 191 limbs were followed for a mean of 4.2 years. Revascularization for life-style limiting claudication occurred in 63 (88%) limbs in patients 65 years or less, 53 (85%) of limbs in patients > 65 to 75 years old, and 42 (74%) of limbs in patients over 75 years of age. There were 62 deaths over follow-up, which were not related to age (HR for age > 65 to 75 y = 1.7 [95% CI = 0.9, 3.4]; HR for > 75 y = 1.3 [95% CI 0.9, 1.8]). Repeat revascularization occurred in 49 limbs and was not related to age (HR for > 65 to 75 y = 0.5 [95%CI = 0.2, 1.0]; HR for >75 y = 0.9 [95% CI = 0.7, 1.3]). There were nine amputations, which were not related to age > 75 y (HR for > 65 to 75 y = 1.3 [95% CI = 0.3, 5.1]; HR for > 75 y = 0.6 [95% CI = 0.2, 1.8]). Multivariable models showed similar results.
Conclusion: Age and age over 75 years was unrelated to poorer survival or more adverse limb events over long-term follow-up. These support the practice of considering SFA endovascular intervention in older patients with life-style limiting claudication unresponsive to medical therapy or critical limb ischemia.
1359
Critical limb ischemia and long-term outcomes after superficial femoral artery revascularization
1VA Boston Healthcare System, West Roxbury, MA; 2Harvard Medical School, Boston, MA; 3Brigham and Women’s Hospital, Boston, MA; 4University of Pittsburgh, Pittsburgh, PA; 5Medical University of South Carolina, Charleston, SC; 6Central Maine Medical Center, Lewiston, ME
Background: Critical limb ischemia is related to poorer survival and adverse limb events in the first few years after superficial femoral artery (SFA) endovascular intervention. Whether these risks are attenuated over longer follow-up is uncertain. We assessed long-term outcomes in patients having SFA endovascular revascularization in 2 institutions.
Methods: All patients having SFA endovascular revascularization for lifestyle-limiting claudication or critical limb ischemia by the Cardiovascular Divisions of the VA Boston Healthcare System and the Brigham and Women’s Hospital between 2003 and 2010 were followed by chart review for death and the adverse limb events of repeat revascularization and limb amputation. The national and VA death indices were also searched. Procedures were classified as critical limb ischemia (rest pain or tissue loss) or claudication at the index procedure. Cox proportional hazard models clustered by patient were used to estimate the hazard ratio and 95% confidence interval (HR, 95%CI) of death and adverse limb events for critical limb ischemia versus claudication.
Results: 153 patients with index SFA endovascular interventions in 191 limbs were followed for a mean of 4.2 years and maximum of 13 years; 33 (17%) limb procedures were for critical limb ischemia. There were 62 deaths, 49 limbs requiring repeat revascularization, and 9 limb amputations over follow-up. The risk of death and adverse limb events kept increasing more than 5 years after the index procedure. At 5 years Kaplan-Meier event rates for critical limb ischemia versus claudication were 74% versus 30% for death, 59% versus 29% for repeat revascularization, and 45% versus 3% for amputation. Compared to claudication, critical limb ischemia had increased risks for death (HR = 4.3, 95% CI = 2.5, 7.5), repeat revascularization (HR = 2.2, 95%CI = 1.1, 4.7), and amputation (7/9 = 78% of amputations were in patients with critical limb ischemia).
Conclusion: Critical limb ischemia continues to have a major impact on death and adverse limb events many years after SFA revascularization. These patients warrant intensive medical therapy and vascular surveillance.
1362
Adverse limb related outcomes in end stage renal disease patients with peripheral artery disease: an analysis from USRDS database
University of Kansas Medical Center, Kansas City, KS
Background: The natural history of peripheral artery disease (PAD) in end stage renal disease (ESRD) patients is not well understood. The goal of this study was to assess the occurrence of adverse vascular outcomes and mortality in a large cohort of ESRD and patients with PAD.
Methods: Medicare beneficiaries diagnosed with PAD within 6 months of incident dialysis were identified from United States Renal Data System (USRDS) (Jan 1st, 2006 to May 31st, 2017). Patients who had renal transplants were excluded. We used in-hospital and outpatient claims to assess incident complications and outcomes of PAD up to three years.
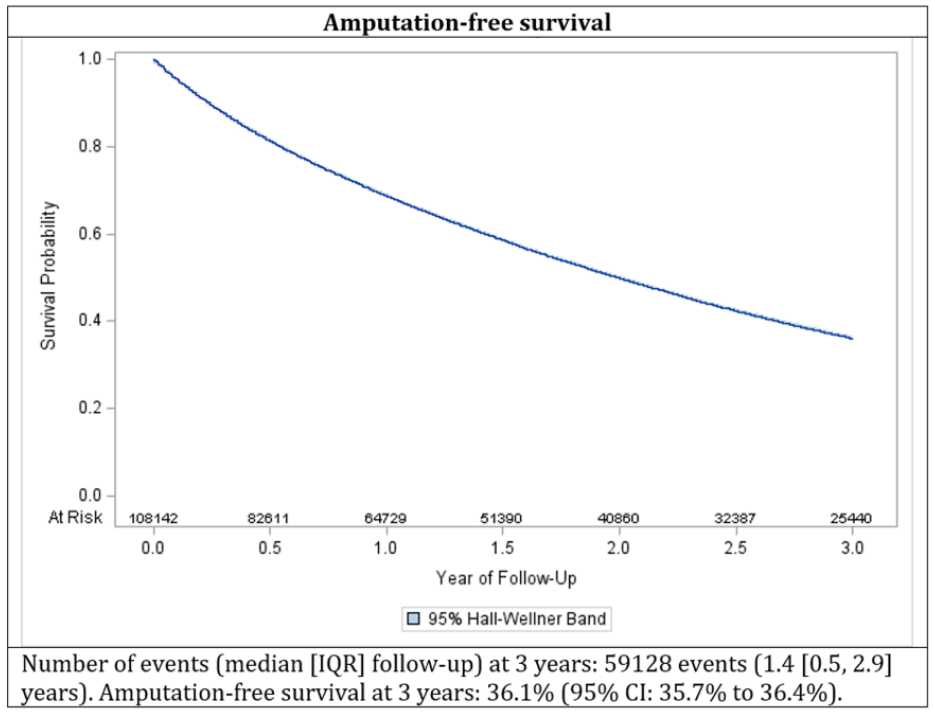
Results: We identified 108,142 study patients (mean age 71.5 years, female 41.1%) with a median follow up of 547 days (IQR, 215 - 1096 days). Most (95%) were on were on hemodialysis. Overall survival at 3 years was 39.0% (95% CI: 38.7% to 39.3%). New critical limb ischemia (CLI) occurred in 29.7% at 3 years with a median time to event of 423 days. The amputation-free survival at 3 years was 36.1% (95% CI: 35.7% to 36.4%) and continued to decline sharply (see Fig.). Overall revascularization rate was 25.7% (95% CI: 25.3% to 26.1%). Overall MALE (all revascularization, CLI, amputation) at 3 years was 42.0%.
Conclusion: ESRD patients with PAD are at an extremely high risk of death and incident adverse limb events with only one of three patients having an amputation free survival at three years. The poor prognosis noted in our study informs future studies planning interventions to improve outcomes in these cohort of patients.
Poster 1362 Figure.
1383
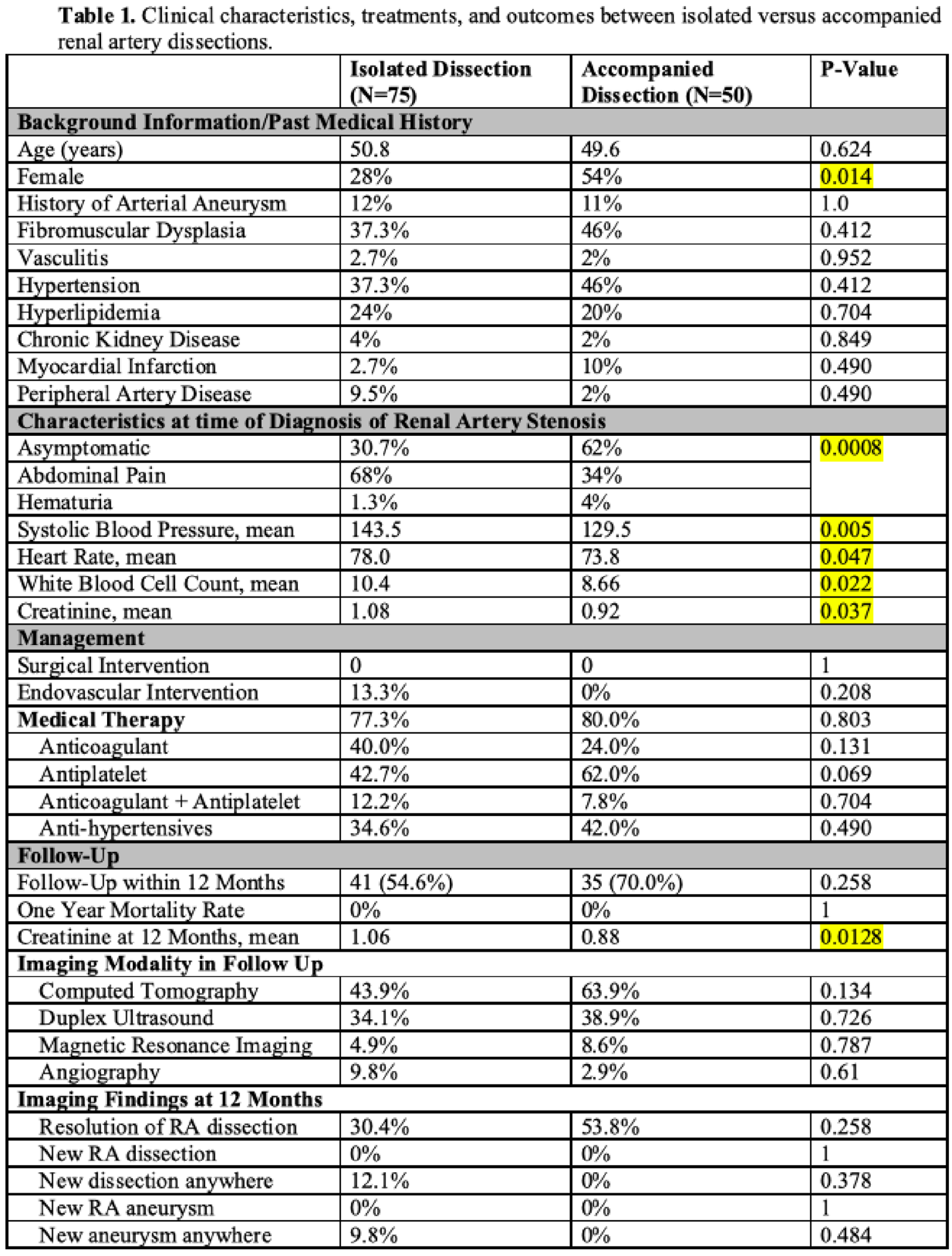
Clinical characteristics, treatment, and outcomes of patients with renal artery dissections
1Massachusetts General Hospital, Boston, MA; 2Weill Cornell Medicine-Qatar, Doha, Qatar
Background: Spontaneous renal artery (RA) dissections are poorly understood. Data are specifically limited concerning patients with an RA dissection and an accompanying arterial dissection elsewhere.
Methods: We used ICD-9/ICD-10 codes to identify patients with RA dissections at a tertiary medical center between 2001-2020. We compared clinical characteristics, treatment, and outcomes between patients with isolated versus accompanied renal artery dissections.
Results: 125 patients were diagnosed with RA dissections; 75 had an isolated dissection while 50 had concurrent arterial dissections (Table 1). When present, concurrent dissections occurred in a mean of 2.6 additional arteries, most commonly superior mesenteric (42.0%), celiac (28.0%), and iliac (28.0%). Patients with concurrent dissections were more likely female (54% vs. 28%) and asymptomatic (62% vs. 30.7%). Medical management only was most common (80% vs. 77.3%) and endovascular therapy was infrequent (13.3% vs. 0%). CTA (63.9% vs. 43.9%) and duplex ultrasound (38.9% vs. 34.1%) were utilized most often in follow-up. Over 12 months, additional dissections occurred nominally more often in patients with isolated dissection (12.1% vs. 0%) and renal function remained stable. There were no deaths in either group.
Conclusion: Patients with RA dissection, either in isolation or accompanied by other dissections, have a benign course in the first year after diagnosis as recurrent dissection rates are low and mortality is uncommon.
Poster 1383 Table.
1385
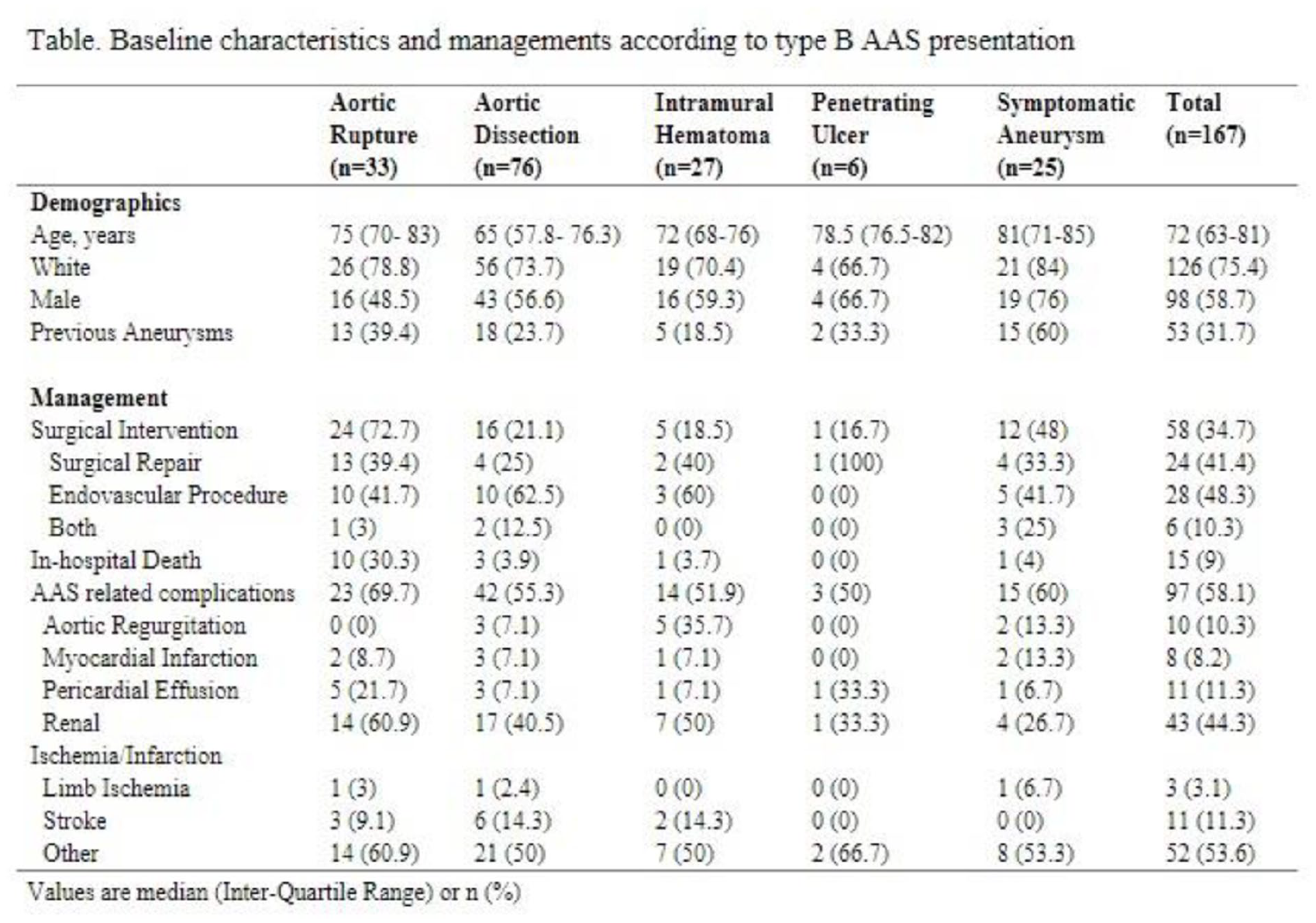
Management of type B acute aortic syndromes at a single academic medical center: insights from the code aorta registry
1Brigham and Women’s Hospital, Boston, MA; 2Georgetown University School of Medicine, Washington DC; 3University of Santo Amaro, São Paulo, Brazil
Background: Acute aortic syndromes (AAS) involving the descending aorta (Stanford type B) are life-threatening emergencies that require prompt evaluation and complex multidisciplinary management. We report the initial experience of our AAS program in the management of patients with type B AAS.
Methods: We performed a retrospective analysis of all patients admitted to our center with type B AAS between July 2012 and October 2020. Type B AAS presentations included aortic dissection, aortic rupture, intramural hematoma (IMH), penetrating atherosclerotic ulcer, and symptomatic aneurysm.
Results: 167 patients with type B AAS were admitted to the hospital and included in the analyses. Patients were most often white (75.4%) and male (58.7%). 76 (45.5%) patients presented with aortic dissection, 33 (19.8%) with aortic rupture, 27 (16.2%) with IMH, 25 (15%) with symptomatic aneurysm, and 6 (3.6%) with penetrating ulcer. 109 (65.3%) patients were medically treated, whereas 58 (34.7%) underwent surgical intervention. Of these, 28 (48.3%) had an endovascular procedure, 24 (41.4%) had a surgical repair. AAS-related complications occurred in 97 (58.1%) patients. There were 15 (9%) in-hospital deaths. Aortic rupture had the highest rate of in-hospital mortality (30.3%) (see Table).
Conclusion: Our experience offers insight into the different presentations of AAS. Despite the varying levels of mortality among AAS subtypes, we found a high percentage of AAS-related complications across all subtypes.
Poster 1385 Table.
1387
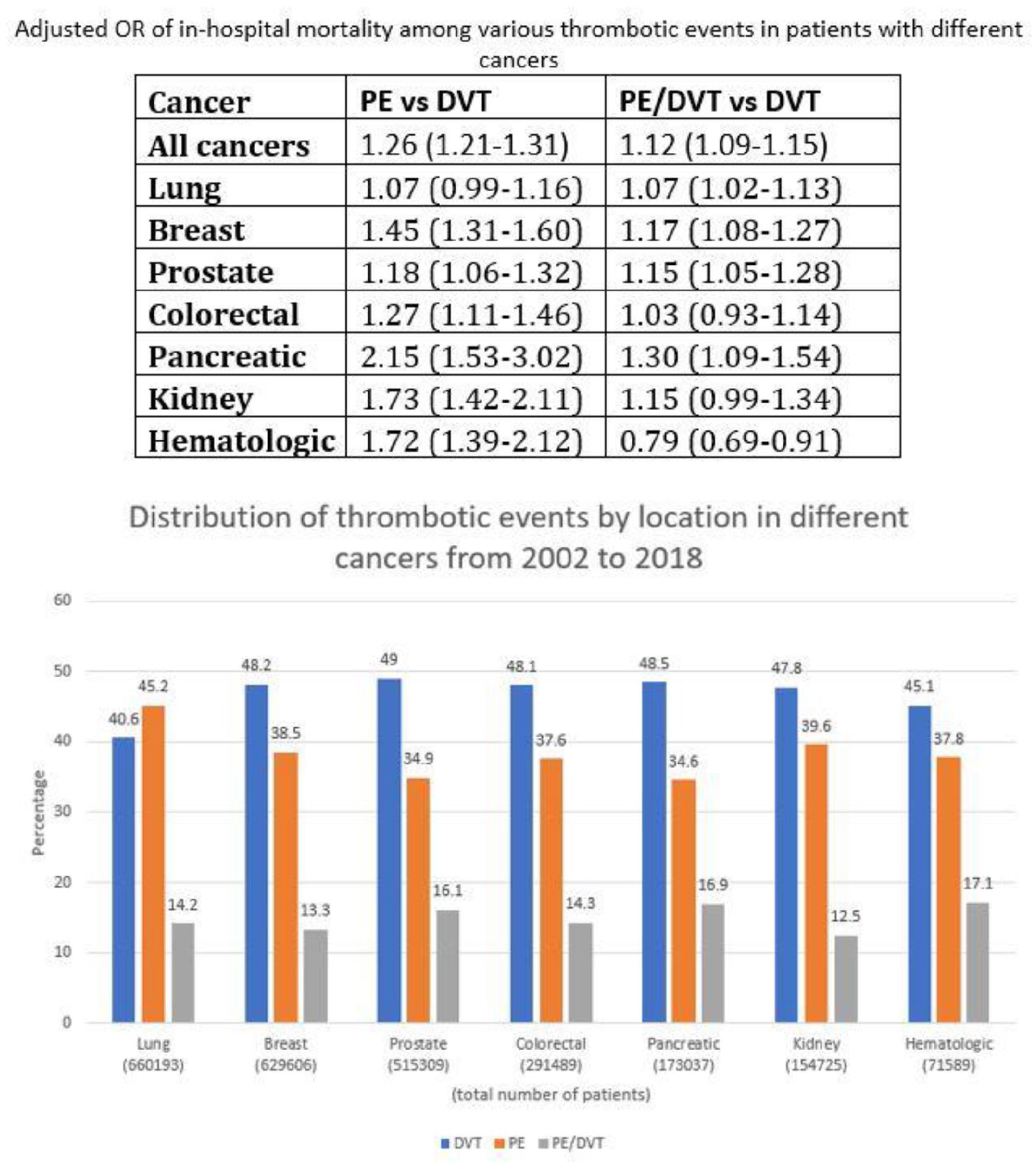
Embolic propensity and in-hospital mortality following venous thrombosis among major cancer types
1Mayo Clinic, Rochester, MN; 2Abington Jefferson Health, Philadelphia, PA; 3Thomas Jefferson Hospital, Philadelphia, PA
Background: The impact of venous thrombus location and burden on in-hospital mortality rates among specific cancer types has not been previously explored. The aim of this study was to test the hypothesis that cancer type influences both the propensity for embolic disease and adversely impacts in-hospital mortality rates.
Methods: National (Nationwide) Inpatient Sample (NIS) was searched for hospitalizations for cancer associated venous thromboembolism (2002-2018), parsed by major cancer type and thrombus location: pulmonary embolism (PE), deep venous thrombosis (DVT), or both PE plus DVT. Categorical variables were compared using binary regression model to obtain adjusted odds ratio (aOR) for in-hospital mortality rates.
Results: Of 3,260,535 cancer-associated VTE hospitalizations, the seven most common cancer types were lung (20.2%), breast (19.3%), prostate (15.8%), colorectal (8.9%), pancreatic (5.3%), kidney (4.74%) and hematologic (2.19%). DVT was more common presentation among all cancer types except for lung cancer which had more PE than DVT (45.2%vs 40.6%) (see Fig.). PE was associated with increased in-hospital mortality rates among all cancer types except for lung cancer (Table). DVT was associated with prolonged length of stay with higher hospital costs compared to PE.
Conclusion: In this large inpatient sample, cancer type influenced both embolic propensity and in-hospital mortality particularly among those patients with PE.
Poster 1387 Figure.
1395
Diagnostic evaluation of arterial foot flow using plantar acceleration time
Philippine Heart Center, Quezon City, Philippines
Background: Ankle brachial index (ABI) is the most commonly requested diagnostic test to determine the presence and / or severity of peripheral artery disease (PAD). However, limitations in ABI exist precluding evaluation of arterial flow in the feet such as medial arterial calcification, wound, and unbearable pain. Because of these restrictions, we investigated a novel noninvasive diagnostic technique to evaluate plantar foot flow called plantar acceleration time (PAT).
Methods: This is a prospective cohort study, which included 71 patients with ABI and PAT using non-invasive vascular ultrasound. All patients with age of 19 years old and above suspected or diagnosed PAD, with or without non-healing wound and /or gangrene with ABI were included. Patients with severe pain unable to undergo the test, with prior lower extremity revascularization procedures and / or amputation, and with acute limb ischemia were excluded. Convenient sampling was done. Clinical class, ABI and PAT were obtained using standard vascular protocols.
Results: A total of 142 limbs were classified to compressible and non-compressible arteries. There was a high correlation of PAT and ABI in compressible arteries (r -0.71, p < 0.001). PAT also showed significant correlation (p-value < 0.001) in all clinical classes of PAD with compressible arteries. In non-compressible limbs, PAT has negligible correlation to ABI (r -0.05, p < 0.816), but with significant correlation to clinical classes (p-value < 0.001).
Conclusion: In the Philippines, this study is the first to demonstrate the use of PAT as a reliable non-invasive tool to evaluate lower extremity arterial disease or PAD. PAT correlates well with different ABI groups and clinical classes in patients with compressible arteries. PAT also correlates well with clinical class in patients with non-compressible arteries. Clinically, PAT can be used as an alternative or complementary tool in evaluating the presence and severity of PAD, especially in patients with falsely elevated ABI, presence of wound, and occurrence of intolerable pain that deters measurement of ABI.
1408
Effectiveness and safety of combined direct oral anticoagulant and antiplatelet therapy among high-risk peripheral artery disease patients -a meta-analysis
Manila Doctors Hospital, Metro Manila, Philippines
Background: Peripheral artery disease (PAD) is a common manifestation of systemic atherosclerosis which strongly correlates to cardiovascular morbidity and mortality and increased risk of limb loss, and despite the wide use of guideline-based antiplatelet therapy, patients remain at high risk for cardiovascular and limb events. There has been increasing interest in novel anticoagulants to improve prevention of complications secondary to PAD, and this study aims to determine the effectiveness and safety of combined direct oral anticoagulant plus antiplatelet in reducing MACE, MALE, and all-cause mortality among patients with PAD.
Methods: Randomized controlled trials with outcomes on major adverse cardiac events (MACE), major adverse limb events (MALE), all-cause mortality and bleeding were searched through PubMed, Cochrane, and EBSCOHost.
Results: Pooled analysis of studies on patients PAD showed that anticoagulant combined with antiplatelet have significant benefits compared with antiplatelet alone in reducing major adverse limb events (RR 0.72, 95% CI 0.62 to 0.83) and stroke (RR 0.74, 95% CI 0.57 to 0.97) but had inconclusive results in reducing myocardial infarction (RR 0.85, 95% CI 0.70 to 1.03).There was no significant benefit in reducing cardiovascular death (RR 1.04, 95% CI 0.88 to 1.23) and all-cause mortality (RR 1.02, 95% CI 0.90 to 1.16). Likewise, there was increased risk of bleeding (RR 1.46, 95% CI of 1.18 to 1.80) compared with antiplatelet alone.
Conclusion: Anticoagulant (Rivaroxaban) combined with antiplatelet (aspirin) as alternative to traditional antiplatelet (aspirin) therapy significantly reduced major adverse limb events and stroke. However, there was a higher incidence of bleeding for the combined cohort. Therefore, it is deemed necessary to identify patients with high-risk PAD with low risk of bleeding who can benefit the most with the combined intervention.
1414
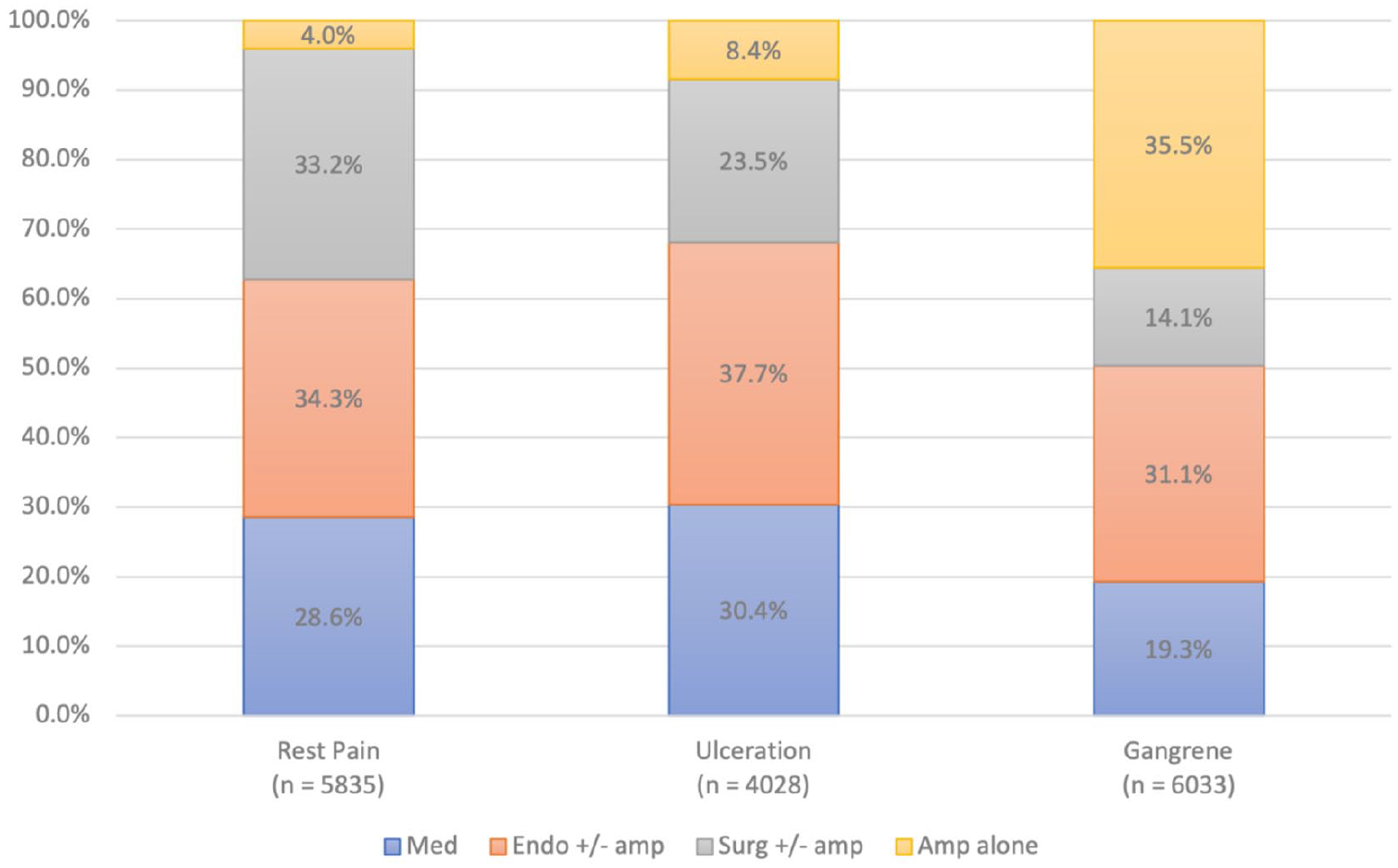
Critical limb ischemia treatment variability in the us: an analysis of the 2016-2018 nationwide inpatient sample
1Brown University, Providence, RI; 2Independent Statistical Consultant, Kansas City, MO; 3Beth Israel Deaconess Medical Center, Boston, MA; 4Dartmouth, Lebanon, NH; 5Case Western Reserve University, Cleveland, OH; 6University of Texas Southwestern, Dallas, TX
Background: Prior data from select healthcare systems suggest that treatments employed for critical limb ischemia (CLI) vary significantly across hospitals. Little is known about CLI treatment variability in the broader US population.
Methods: All patients aged ⩾ 18 years admitted with a CLI primary diagnosis to non-federal US hospitals that offer non-invasive [med], endovascular [endo], bypass [surg], and amputation [amp]), were extracted from the 2016-2018 Nationwide Inpatient Sample. Treatment variability was characterized using the median odds ratio (MOR), adjusted for patient and hospital characteristics; values > 1.2 (i.e., > 20%) suggest high institutional variability in practice.
Results: Among 15,896 patients with mean age 70 years; 41% women, 68% Caucasian, 20% diabetic, and 33% smokers. Med, endo +/- amp, surg +/- amp and amp alone were employed in 4,057 (25%), 5,390 (34%), 3,733 (24%) and 2,716 (17%) patients, respectively; treatments employed by clinical presentation (rest pain, ulceration, gangrene) appear in the
Conclusions: Significant CLI treatment variability exists across US hospitals, which is not fully explained by patient or hospital characteristics. Variability is greatest for endovascular and surgical revascularization.
Poster 1414 Figure.
1419
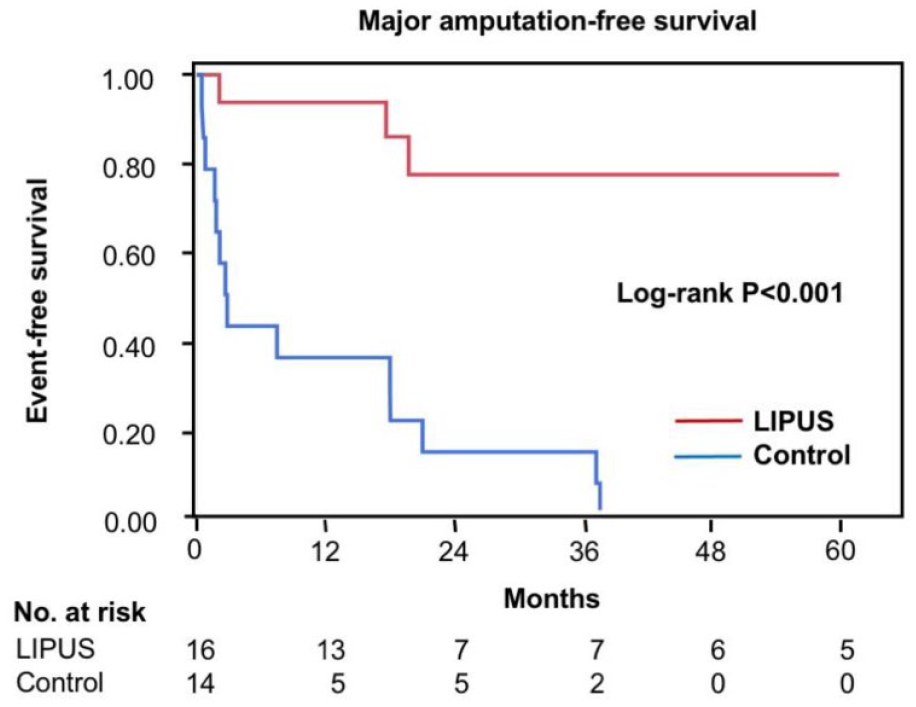
Low-intensity pulsed ultrasound decreases major amputation in patients with critical limb ischemia: 5-year follow-up study
Hiroshima University, Hiroshima, Japan
Background: Various therapeutic strategies for angiogenesis are performed to improve symptoms in patients with critical limb ischemia (CLI). Pre-clinical studies have shown that low-intensity pulsed ultrasound (LIPUS) exposure induces angiogenesis.
Methods: The purpose of this study was to evaluate clinical outcomes in patients with CLI who were treated with LIPUS at 5-year follow-up periods. 14 patients with CLI, who were not candidates for angioplasty or surgical revascularization, were enrolled in this study. Historical control data were obtained from the Hiroshima University PAD database. The primary endpoints were major amputation and death.
Results: Clinical outcomes were compared in 16 lower limbs of the 14 patients with CLI who were treated with LIPUS and in 14 lower limbs of 14 patients with CLI as historical controls. The mean duration of LIPUS exposure in the LIPUS group was 381± 282.6 days. The overall amputation-free survival rate was significantly higher in patients who were treated with LIPUS than in historical controls (see Fig.). There was no significant difference between overall mortality-free survival rates in the LIPUS group and historical control group.
Conclusion: LIPUS is a noninvasive option for therapeutic angiogenesis with the potential to reduce the incidence of major amputations in patients with CLI.
Poster 1419 Figure.
1425
Quality of care and outcomes of lower extremity peripheral artery disease (PAD) on adult diabetic patients admitted in a tertiary hospital in the Philippines
University of the Philippines, Philippine General Hospital, Manila, Philippines
Background: Peripheral artery disease (PAD) causes significant disability, morbidity, and mortality. For quality of care (QOC) improvement measures to be set in place, there is a need to describe the current pattern of care to identify key areas of improvement. We aim to describe the QOC of diabetic patients with PAD in a tertiary government hospital in terms of compliance to the 2016 ACC/AHA PAD guidelines using key quality indicators.
Methods: This study was conducted in our center by interview of patients and review of medical records which were prospectively collected. Adult diabetic patients diagnosed with PAD admitted from April 1 to November 30, 2019 who were referred to the cardiovascular medicine service were included. Parameters to measure QOC and time intervals were calculated. To determine compliance with the ACC/AHA guidelines, quality indicator (QI) for key Class I and Class IIa recommendations were computed (those with appropriate intervention divided by those eligible). Compliance was defined as QI > 75%.
Results: Seventy-two patients were included, majority are males (75%), overweight (BMI 23.19 kg/m2) and smokers (50%). The mean age was 58 years. Major adverse limb events (MALE) were seen in 50 (69.44%). Twenty-one (29.17%) had at least one major adverse cardiovascular event (MACE), 15 of whom died (20.83% mortality rate). Those who experienced MACE were overweight (p 0.01) and have heart failure (p <0.0001). Quality care was observed in terms of the comprehensive review of medical history (100%), lower extremity inspection and palpation (100%), performance of ABI (93.06%), prescription of statins (90.27%) and anti-hypertensives (100%). Suboptimal quality was seen in terms of femoral bruit auscultation, performance of duplex ultrasonography (13.23%), use of antiplatelet (52.77%) and ACE inhibitors or ARBs (62.5%).
Conclusion: We described the typical profile of an adult diabetic Filipino diagnosed with PAD. Delays in seeking of medical consult, performance of diagnostic imaging and definitive surgical procedure contributed to adverse limb events. Establishment of a “PAD Pathway” could possibly improve compliance to guidelines and reduce both major adverse limb and cardiac events and mortality.
1430
Clinical profile of patients with peripheral artery disease treated with high-pressure intermittent pneumatic compression in St. Luke’s Medical Center-Quezon City: a 6-year retrospective cohort study
St. Luke’s Medical Center - Quezon City, Quezon City, Philippines
Background: High-pressure intermittent pneumatic compression (HPIPC) has been proposed as an alternative intervention to supervised exercise to improve intermittent claudication in patients with peripheral artery disease (PAD). This intervention has already been introduced in the Philippines. However, no local data has been published regarding the clinical profile of patients with PAD treated with HPIPC. This study aims to determine the clinical profile of patients with PAD treated with HPIPC in St. Luke’s Medical Center – Quezon City (SLMC-QC) from March 2015 to March 2021.
Methods: A total of eighty-three (N = 83) adult patients aged ⩾ 19 years with confirmed diagnosis of PAD and symptoms of intermittent claudication who received at least 12 sessions of HPIPC in the Department of Vascular Medicine of SLMC-QC from March 2015 to March 2021 were included in this retrospective cohort study. The primary outcome was identification of the clinical profile of the study population. Descriptive statistics were generated for all variables. Continuous variables were presented as mean standard deviation (SD). Nominal data were reported as frequencies and percentages. All data were analyzed using Statistical Package for the Social Sciences (SPSS) v27 software.
Results: The mean (SD) age of the study population was 75 (14) years. Approximately 76% of them were aged ⩾ 65 years (n = 63). Overall, there were more males (57%) than females (43%) in the study. Majority of the study population never smoked (70%), had hypertension (89%), diabetes (81%), dyslipidemia (78%) and abnormal ankle-brachial index (ABI, 80%). The mean (SD) ABI of the study population was 0.92 (0.5). Hemodynamically significant stenosis in the distal and proximal arterial segments of the lower extremities were 92% and 62% respectively.
Conclusion: Age ⩾ 65 years, male sex, never-smoker, hypertension, diabetes, and dyslipidemia define the clinical profile of patients with PAD treated with HPIPC in SLMC-QC from March 2015 to March 2021. Further studies are recommended to test the association of these risk factors to PAD and to determine the efficacy of HPIPC in the treatment of PAD.
Clinical Case Abstracts
1180
A young Filipino male with clinical catastrophic antiphospholipid syndrome and probable systemic lupus erythematosus presenting as cerebral venous thrombosis: a case report
Makati Medical Center, Makati City, Philippines
Background: Catastrophic antiphospholipid syndrome (CAPS) is a rare form of antiphospholipid syndrome (APS) and often a life-threatening autoimmune disease characterized by microvascular thrombotic complications usually affecting multiple organs. Cerebral venous thrombosis (CVT) is a sporadic condition with an accrued annual incidence from 0.22 to 1.57 per 100,000 with a female to male ratio of 3:1.
Methods: We report a young-adult Filipino male patient with clinical CAPS with probable systemic lupus erythematosus.
Results: A 43-year-old right-handed non-hypertensive, non-diabetic male presented in our institution because of jerking and stiffening of extremities. Cranial MRI showed a subacute infarct. Venous duplex scan showed a subacute DVT, partially occluding the left proximal to mid popliteal vein, a chronic DVT, partially occluding the left distal popliteal vein, and chronic calf vein thrombosis, partially occluding the left soleal vein. In the interim, he neurologically deteriorated prompting intubation. Repeat MRI showed hemorrhagic conversion of subacute infarct in the right frontoparietal lobe and an intraparenchymal hemorrhage in the left parietal lobe. He underwent decompressive hemicraniectomy and evacuation of hematoma. Intraoperative findings revealed significant cerebral edema, thrombosis of left vein of Trolard with venous congestion of small cortical veins. Further work up showed an elevated lupus anticoagulant LA1 and LA2, anticardiolipin and B2 glycoprotein IgG and IgM. Anti-nuclear antibody was positive with 1:640 titer, nucleolar pattern but a negative lupus panel. Nailfold capillaroscopy showed the presence of several non-specific anomalies and hemorrhages. He remained in deep stupor to mild coma with no eye-opening for the next 9 days. Signs of improvement were seen on the 10th POD with further improvement. Over time, he remained seizure-free with improving left-sided hemiplegia. He was eventually discharged significantly improved with advice of close follow up, religious compliance to medications and physical therapy.
Conclusion: The importance of a multidisciplinary approach in both the diagnosis and management of CAPS could not be over emphasized.
1183
A young Filipino male with clinical catastrophic antiphospholipid syndrome, hereditary thrombophilia and hyperthyroidism presenting as cortical vein thrombosis: a case report
Makati Medical Center, Makati City, Philippines
Background: Catastrophic antiphospholipid syndrome (CAPS) is a rare form of antiphospholipid syndrome (APS) and often a life-threatening autoimmune disease characterized by microvascular thrombotic complications usually affecting multiple organs. Cerebral venous thrombosis (CVT) is a sporadic condition with an accrued annual incidence from 0.22 to 1.57 per 100,000 with a female to male ratio of 3:1.
Methods: Reporting a young-adult Filipino male patient with clinical CAPS with concomitant hereditary thrombophilia and hyperthyroidism with sinus and cortical vein thrombosis.
Results: A 38-year-old male with no co-morbid conditions presented at our institution because of left-sided weakness. In the interim, the patient had recurrent unilateral headache and recurrent motor tonic seizures with associated urinary incontinence. He had left hemineglect and was inconsistent in following commands. He had multiple, hyperpigmented, circumscribed lesions over both lower legs. Cranial imaging showed minimal subarachnoid hemorrhages identified along the left high parietal, bilateral mesial frontal and right central sulci and right Sylvian fissure with the superior sagittal and right transverse sinuses as well as the entire right vein of Trolard, proximal left vein of Trolard and the bilateral frontal cortical veins appearing hyperdense. Diagnostics showed normal C3 and C4 levels, an increased ESR, a positive ANA at 1:40 dilution. Lupus anticoagulant LA1 and LA2 were elevated, anticardiolipin and B2 glycoprotein IgG and IgM were negative. Fibrinogen was increased; Factor V, Proteins C and Protein S were decreased; antithrombin III, PTT and PT were normal. TSH was low and FT3 and FT4 were elevated. Nailfold capillaroscopy showed an absent subpapillary venous plexus, abnormal distribution and frequent irregularity in shape of capillary loops with frequent ramification and crisscrossing with some areas of hemorrhages. On the 7th hospital day, the patient remained seizure-free with only mild drift of the LUE. He was eventually discharged improved.
Conclusion: Due to high mortality rates of CAPS, the importance of a multidisciplinary approach in both the diagnosis and management is paramount.
1184
One HIT After Another: A Case of PE with HIT
Boston Medical Center, Boston, MA
Background: Heparin induced thrombocytopenia (HIT) is a rare but serious immune system-mediated complication of heparin therapy. Pulmonary embolus (PE) is a known complication that highlights many therapeutic dilemmas and requires a multidisciplinary approach.
Methods: A 44-year-old female with no know prior medical history presented to the hospital with right lower quadrant pain. A pelvic ultrasound was performed that showed a right adnexal cyst measuring 14 x 8.7 x 13.7 cm. The patient was referred for MRI that showed features highly concerning for malignancy. She underwent an open salpingo-oophorectomy and hysterectomy with frozen pathology exhibiting mucinous carcinoma. She was transferred to the floor and over the next 3 days, the platelet count declined from 343 to 45 while on low molecular weight heparin for DVT prophylaxis. Due to the concern for HIT, all heparin products were stopped. Hematology was consulted and argatroban was recommended. Subsequently, the patient developed acute dizziness, shortness of breath, and hypotension. An emergent CTPA showed a large saddle PE. Transthoracic echocardiogram exhibited right ventricular dysfunction and McConnell’s sign. Laboratory workup was notable for troponin of 0.231 ng/uL and BNP of 60 pg/mL. The pulmonary embolism response team (PERT) was activated.
Results: The patient was found to have a massive PE with signs of obstructive shock. The etiology of her embolus was her hypercoagulable state given her likely HIT diagnosis based on a high 4T score. Lytic therapy was contraindicated given her severe thrombocytopenia and recent surgery. In a multidisciplinary manner with cardiology, critical care, and hematology, the decision was made to proceed with argatroban therapy solely. Lab workup later confirmed the diagnosis of HIT. The patient responded well with improvement in her clinical status and was eventually transitioned to an oral anticoagulant. She has been stable in outpatient follow up.
Conclusion: This case exhibits a case of HIT causing a massive PE in the setting of a recent surgery. It highlights the importance of a PERT system and a multidisciplinary approach in patients with complex systemic diseases.
1186
Dual basilic vein access for catheter directed thrombolytic therapy in acute pulmonary embolism: a single-center experience
University of Cincinnati College of Medicine, Cincinnati, OH
Background: Catheter directed thrombolysis (CDT) offers comparable outcomes to systemic thrombolysis with better risk profile and lower thrombolytic dose in select intermediate to high risk patients with acute pulmonary embolism (PE). The EkoSonic Endovascular System (Ekos) uses combined ultrasound and CDT to enhance the lysis of acute thrombi. This study aimed to assess safety of dual basilic vein (BV) cannulation for bilateral CDT.
Methods: This is a single-center, case series of consecutive patients presenting with acute intermediate-high risk submassive PE, that underwent CDT with EKOS via dual right BV cannulation between June 2019 and December 2020. Safety outcomes were recorded both during the index hospitalization and at 2-week clinic follow up. The outcomes of interest were major bleeding, major adverse cardiovascular events (MACE), access site complications, infusion catheter malfunction and persistent upper-extremity neurological symptoms.
Results: There were 13 patients who received CDT via the BV during the study period; age, 36 ± 11 years; male, 4 [30.8%]. All 13 patients had elevated troponin levels and right ventricular dilatation with >0.9 right ventricle to left ventricle ratio, mean pulmonary embolism severity index score (PESI) score of 87.7 ± 26.7 and median B-type natriuretic peptide (BNP) level of 451 pg/mL. The entire study population had successful dual cannulation of the right BV with placement of bilateral pulmonary EKOS catheter. No complications were reported during the hospital stay or at outpatient follow up.
Conclusions: Dual cannulation of BV offers a safe alternative approach for CDT with EKOS with major ergonomic advantage. This technique could be advantageous particularly for patients with inability to lie supine or with high risk of access site complications with deep vein cannulation.
1224
Roadcut complete internal carotid artery occlusion presenting as stroke in the young: a case report
Desiree Afaga
Manila Doctors Hospital, Manila, Philippines
Background: Complete occlusion of the internal carotid artery (ICA) is rare (6 per 100,000) among young adults with ischemic stroke. This case was presented to show challenges in the diagnosis and management of this patient. This aimed to help clinicians understand the importance of a thorough investigation to ascertain the stroke etiology and direct the management.
Method/Case Presentation: A 38-year-old hypertensive, obese male presented with left-sided weakness. Stroke etiology (atherothrombotic, cardioembolic, hypercoagulable state, embolic stroke of undetermined source) was investigated. Complete occlusion of the right ICA was confirmed with transfemoral cerebral angiogram. An atherothrombotic source was primarily considered. Hypercoagulable workups were unremarkable except for a falsely elevated dilute Russell viper venom time related with anticoagulation. This is essential in establishing antiphospholipid antibody syndrome since it necessitates anticoagulation. He was discharged improved with direct oral anticoagulant and antiplatelet.
Results: Chronic total occlusion (CTO) of the internal carotid artery (ICA) entails understanding of its natural history depending on the established source. CTO portends a good prognosis but may increase the risk for ischemic events if contributing factors are not addressed.
Conclusion: CTO of the ICA presenting as stroke in the young entail thorough investigation leading to carefully selected treatment options.
1231
Osteophytic iliac venous compression: A rare case of bony May-Thurner syndrome
Boston Medical Center, Boston, MA
Background: Classic May-Thurner Syndrome (MTS) is defined as extrinsic compression of the left common iliac vein (LCIV) by the right common iliac artery (RCIA) causing venous stasis that can lead to deep vein thrombosis (DVT). We report a rare case of MTS variant in which a vertebral osteophyte compresses the LCIV.
Methods: A 71-year-old male presented with left lower extremity (LE) pain/edema. He underwent LE US that showed chronic thrombus in the left proximal to distal femoral vein and acute thrombus in the left popliteal vein. He was also diagnosed with paroxysmal atrial fibrillation (PAF) with palpitations and was started on anticoagulation (AC). He underwent pulmonary vein isolation for PAF, during which it was noted that his LCIV was subtotally occluded. Repeat LE US showed resolving DVT in the mid to distal femoral and popliteal vein and chronic venous disease of the proximal to mid femoral vein. He then underwent CT venogram (see Fig.) to assess for MTS which showed bony variant of MTS with lumbosacral osteophytic compression of the LCIV.
Results: Given mild symptoms and need for chronic AC (on apixaban for PAF), multidisciplinary decision was made to manage conservatively with AC and compression stockings for mild LE edema.
Conclusion: This is a case of bony MTS with osteophytic compression of LCIV. Although rare, this diagnosis should be considered in older patients with LE DVT especially with iliofemoral distribution. Treatment depends on severity of symptoms and includes AC, thrombectomy, and stenting/venoplasty.
Case Report 1231 Figure.
1239
Hybrid superior mesenteric artery and celiac artery bypass grafting from the right external iliac artery after aorto- bilateral common iliac artery endovascular repair in an 84-year-old Filipino with chronic mesenteric ischemia and extensive vasculopathy
St. Luke’s Medical Center - Global City, Taguig, Metro Manila, Philippines
Background: Chronic mesenteric ischemia is a reduction in intestinal blood flow that is commonly caused by atherosclerotic disease. It is a rare occurrence and frequently diagnosed at its late stage due to nonspecific symptoms.
Methods: This is a case of an 84-year-old, male, known coronary and carotid artery disease. The patient has been experiencing intermittent abdominal pain for four years. He underwent repeated gastrointestinal work up: esophagogastroduodenoscopy and colonoscopy with the consistent finding of erosive gastritis. Medical management was maximized with proton pump inhibitor and mucosal protectant. Abdominal pain was eventually noted to be aggravated with meals with eventual weight loss and constipation.
Results: Abdominal duplex scan showed significant stenosis in right common iliac, celiac artery and infra-renal, distal aortic segments, left common iliac artery. Selective celiac angiogram demonstrated (see Fig.) significant stenosis in celiac artery and superior mesenteric artery. Endovascular intervention on the iliac artery was done and completion open bypass surgery on the superior mesenteric artery and celiac artery.
Conclusion: Chronic mesenteric ischemia diagnosis calls for a high index of suspicion when an elderly with extensive vasculopathy presents with recurrent abdominal pain. Early diagnosis and prompt management with revascularization will provide resolution of symptoms, improvement in quality of life and prevention of complications and mortality.
Case Report 1239 Figure.
1274
The Deadly Quad - Polycythemia vera (PV) and Atherosclerosis in a 43-year-old Diabetic Smoker presenting with Chronic Limb Threatening Ischemia (CLTI)
St. Luke’s Medical Center Quezon City, Quezon City, Philippines
Background: Inflammation is a common denominator in the cardiovascular risks brought about by polycythemia vera, atherosclerosis, diabetes mellitus and heavy smoking. The management of this deadly quad in a patient with CLTI with atherothrombosis pivots on minimizing the systemic effects of inflammation. This is a case of a 43-year-old male, diabetic, smoker with PV presenting with CLTI WIFi 2-2-0, Glass III who improved after a few months of medical treatment (see Fig.).
Results: To address inflammation and decrease shearing forces, our patient underwent phlebotomy, cytoreductive therapy, and was given metformin, statin, and aspirin. He was advised smoking cessation, high pressure intermittent pneumatic compression therapy, and rehabilitation.
Conclusion: Among patients with PV who develop CLTI, addressing the inflammation is key to a successful treatment plan. This, combined with a guidelines-based, holistic management of other risk factors for thrombosis and atherosclerosis should be provided to decrease risk of developing further thrombotic events.
Case Report 1274 Figure.
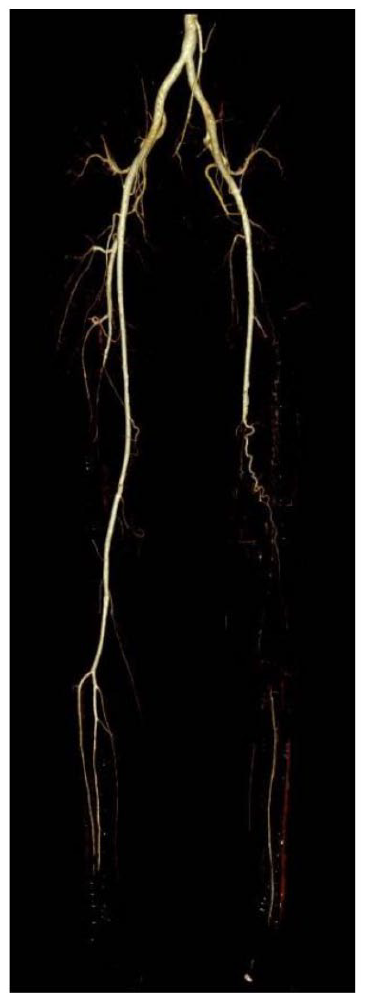
1284
Case Series: Internal jugular (IJ) vein catheter-related thrombosis in patients with severe COVID-19
St. Luke’s Medical Center Quezon City, Quezon City, Philippines
Background: There are a number of thrombotic complications from SARS-CoV-2 infection which may be from the activation of the coagulation pathway by inflammatory cytokines. Most patients with severe SARS-CoV-2 infection would require an IJ catheter insertion for different purposes; and this, compounded by the increased state of inflammation puts the patient at risk for catheter-related thrombosis.
Methods: In a tertiary hospital, seven patients with severe SARS-CoV-2 infection have presented with acute catheter-related IJ thrombosis (see Fig.). Most of them have high levels of D dimer, Ferritin, and acute phase inflammatory markers.
Results: These patients were initially on prophylactic dose of Enoxaparin, which was uptitrated to treatment doses for a minimum of 5 days. Repeat duplex scan was done on follow-up to reassess thrombus status prior to removal of the IJ catheter.
Conclusion: To date, there is a lack of recommendations for managing catheter-related thrombosis among patients with COVID-19. This is, however, an important issue to address as both the presence of a catheter and the systemic inflammation brought about by SARS-CoV-2 infection predisposes a patient to thrombus formation.
Case Report 1284 Figure.
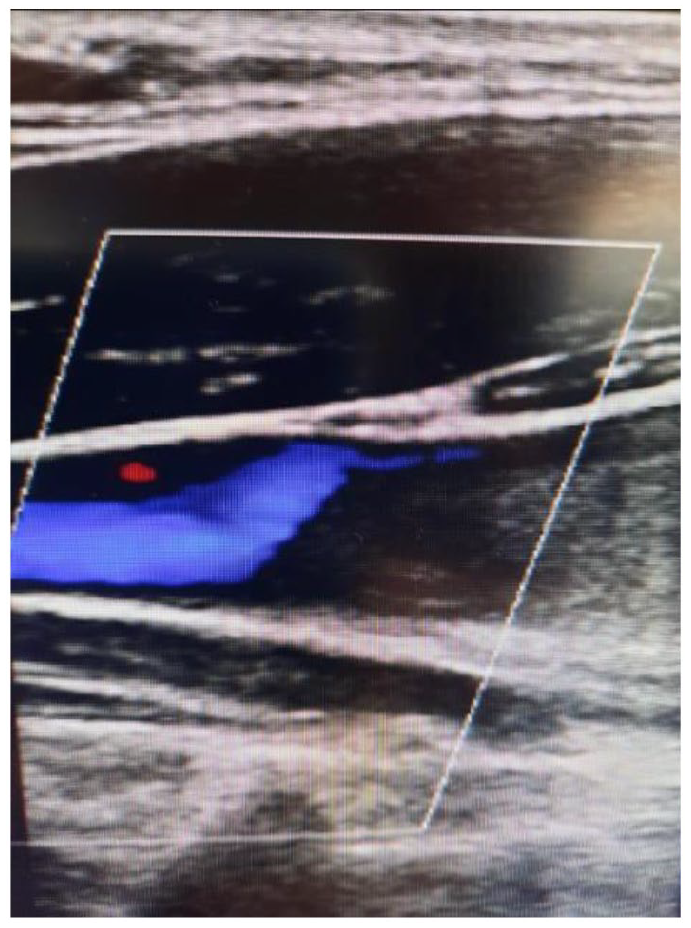
1285
Recurrent acute limb ischemia in a patient with known allergy to contrast material: a case report
Makati Medical Center, Makati, Philippines
Background: Acute limb ischemia (ALI) is defined as a sudden limb-threatening decrease in arterial perfusion of less than 14 days’ duration. It is a vascular emergency that requires rapid recognition and treatment to prevent limb loss and morbidity. As such, numerous guidelines were formulated in order to aid clinicians on how to go about its diagnosis and management.
Methods: Electronic medical records of a patient with recurrent ALI with known allergy to contrast material were reviewed. Moreover, search for available literatures related to topic was done for a relevant literature review.
Results: A 69-year-old female, hypertensive with known allergy to contrast material, previously went into cardiopulmonary arrest after receiving contrast dye, presented with unilateral left leg pain. She had duplex ultrasound (DUS) showing a totally occluding acute thrombus in the left distal superficial femoral artery (SFA), for which she underwent thrombectomy. Heparin drip was instituted. Completion imaging by means of computed tomography angiography was requested, however, deferred due to allergy. DUS with pedal acceleration time (PAT) was utilized instead. Repeat imaging showed a totally occluding acute thrombus in the left distal SFA with slightly abnormal PAT, for which she underwent a repeat thrombectomy. Due to labile partial thromboplastin time, heparin drip was shifted to Enoxaparin and patient was referred to Hematology service for possible hypercoagulopathy. Work up on hypercoagulable state or possible cryptogenic ALI (CALI) was held during the acute phase to avoid false results. After the second thrombectomy, DUS again showed an acute thrombus in the left distal SFA. Patient underwent another thromboembolectomy with vein patch angioplasty and was eventually discharged. Intraoperative DUS followed by repeat PAT showed an open popliteal artery and improved PAT.
Conclusion: ALI remains a potentially fatal condition. Prompt recognition and rapid restoration of arterial perfusion remains the cornerstone of therapy. Guidelines are in place to help clinicians manage these patients; however, each patient is unique and should be managed tailored to their needs. CALI should also be actively worked up.
1294
Multiple intra-cardiac thrombi associated with acute pulmonary embolism
Dartmouth-Hitchcock Medical Center, Lebanon, NH
Background: Right heart thrombi and thrombi in transit across a patent foramen ovale (PFO) are uncommonly seen in patients with pulmonary embolism (PE) and are associated with high risk of adverse outcomes. We present a case of bi-atrial thrombi and thrombus in transit in a patient with acute submassive PE.
Methods/Case Description/Results: A 31-year-old male with no significant past medical history presented with 8 days of dyspnea on exertion and pleuritic chest pain. Computed tomography angiography showed large volume of bilateral PE with right ventricular (RV) strain and right atrial (RA) thrombus. He was hemodynamically stable. Cardiac biomarkers were elevated. COVID testing was negative. Pulmonary embolism response team (PERT) was activated. Transthoracic echocardiogram revealed severely dilated RV with severely reduced function. A mobile mass was seen in the RA, possibly anchored to the interatrial septum. An emergent transesophageal echocardiogram showed mobile thrombus within both atria and thrombus in transit through a PFO. After multidisciplinary PERT discussion, involving the patient and his family, decision was made to proceed with a surgical approach, including pulmonary artery and bi-atrial embolectomy, and PFO closure. Post-surgical recovery was uneventful, and he was discharged on aspirin and apixaban on post-operative day 6. Follow up TTE 4 weeks after discharge showed recovered RV size and function. The patient is back to normal functional status.
Conclusion: Combined biatrial thrombi and thrombi in transit are rare in patients with PE. Multidisciplinary approach to such patients, taking into account risks and benefits of each treatment approach, and patient preferences, is of paramount importance to achieve optimal patient outcome.
1308
Using multi-modality with 3d imaging to guide right atrial thrombus extraction via Flowtriever
Lahey Hospital and Medical Center, Burlington, MA
Background: A 79 year-old man with cardiomyopathy EF 30-35%, sick sinus syndrome and atrial fibrillation with dual chamber ICD, presented to the hospital with deep vein thrombosis, pulmonary embolism and was thrombus in-transit in the right atrium (RA) attached to the pacer lead. Despite 3 weeks of anticoagulation therapy, there was no improvement in the RA thrombus size.
Methods: A 24 French Flowtriever device was used to extract the right atrial thrombus using Fluoroscopic guidance as well as transesophageal echocardiogram.
Results: After multiple attempts, we were able to utilize 3D imaging to guide the device placement and successful extraction of the fibrinous thrombus. No residual thrombus was visualized via TEE at the end of the procedure. See Figure.
Conclusion: This case is an example of an innovative use of a device in a very rare clinical scenario. The clinical success in this case makes potential use of this device for a more diverse set of clinical situations.
Case Report 1308 Figure.
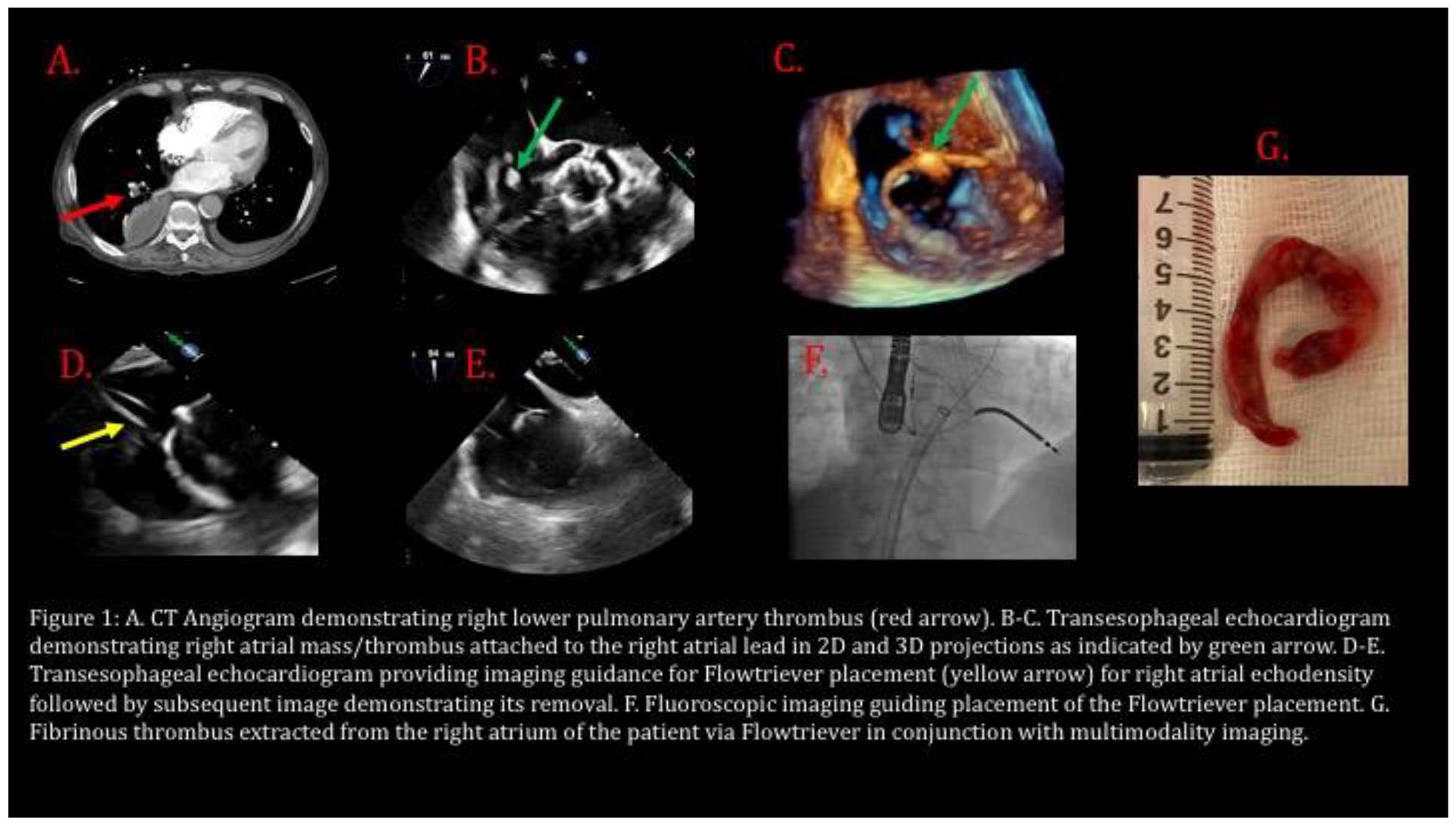
1321
Novel approach in imaging and quantifying microperfusion in non-healing ulcers using contrast enhanced ultrasound: initial case report
Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Manhasset, NY
Background: Contrast-enhanced ultrasound (CEUS) is an evolving diagnostic alternative to contrast-enhanced CT, MRI, and fluorescence angiography for the evaluation of vascular diseases. Microbubble contrast allows for imaging of blood flow in microvasculature beyond the resolution of standard imaging techniques and demonstrates potential for the evaluation of tissue perfusion. Several authors have investigated the application of CEUS in the evaluation of myocardial or skeletal muscle perfusion and tumor characterization. However, this technique has yet to be applied in the evaluation of tissue reperfusion in the setting of wound healing. We report a case of a patient who underwent CEUS evaluation of perfusion in the setting of a non-healing right posterior ankle ulcer pre- and post-revascularization.
Methods: Sonography of the ulcer was performed two weeks before and three days after superficial femoral artery stenting. Imaging was performed using a linear array transducer during intravenous administration of a total of 5 cc of sulfur hexafluoride lipid-type A microspheres (Lumason, Bracco Diagnostics). Perfusion was assessed quantitatively as the amount of contrast present in the subcutaneous tissue over a span of up to six minutes after a total of 5 cc of microbubbles were administered. This data was plotted as a time-intensity curve (TIC), which depicts the average intensity in a predefined region of interest (ROI) as a function of time,showing the transit of microbubbles in a given area. From the TIC, the area under the curve (AUC) and time to peak (TTP) were obtained and used to quantify blood flow and volume in the ROI. The ROI was standardized as a 0.3 by 0.3 cm area within the subcutaneous tissue directly underlying the ulcer on both pre- and post-intervention imaging.
Results: CEUS demonstrated diminished perfusion as evidenced by AUC of 5.7 and TTP of 38 sec. prior to revascularization and increased perfusion with AUC of 50.7 and TTP of 19 sec. after intervention.
Conclusion: CEUS is an important diagnostic modality to qualitatively and quantitatively assess soft tissue perfusion of non-healing ulcers before and after surgical intervention.
1324
Incidental finding of a painless Stanford b aortic dissection in a 60-year-old female admitted for ischemic stroke
Neil Wayne Salces1, Florge Francis Sy2
1Philippine Heart Center, Quezon, Philippines; 2Chong Hua Hospital, Cebu, Philippines
Background: Type B acute aortic dissection (TBAAD) commonly presents with severe, ripping or tearing chest, back, or abdominal pain. Painless TBAAD are relatively rare (3.7%), which can lead to a delay in diagnosis and treatment. Neurologic manifestation such as stroke may be an initial presentation in painless aortic dissection, but these are more common in Type A acute aortic dissection.
Methods: This paper presents an interesting case of a painless TBAAD in a 60-year-old Filipino female who initially presented with acute right-sided weakness and numbness.
Results: A 60-year-old Filipino female with hypertension and diabetes from Sogod (Cebu, Philippines) was admitted for right-sided weakness and numbness. Cranial CT scan showed an acute left thalamic infarct. Dual anti-platelet and statin treatment were started, and permissive hypertension was allowed. Chest radiograph showed a suspicious left upper lobe density. To work up for the chest finding, a contrast-enhanced chest CT scan was done showing a slightly lobulated non-calcified nodule, which may represent a small granuloma in the left lung apex suggestive of pulmonary tuberculosis. However, an incidental finding of an aortic dissection from the distal arch down to the level of the renal arteries was noted. Upon diagnosis of TBAAD, anti-platelet therapy was discontinued, and aggressive blood pressure control was done. TBAAD is managed medically unless there is evidence of end-organ damage. There were no episodes of any chest, back or abdominal pain during the course of admission. There was also no deterioration of neurologic status. A CT aortogram was done a week later showing an aortic dissection extending from the distal aortic arch down to the distal abdominal aorta. There was no evidence of organ malperfusion. The patient was also treated with anti-TB medications and was eventually discharged improved with target BP achieved.
Conclusion: Painless TBAAD is rare and there has not been a report in the literature that it may present with neurologic symptoms such as stroke. The incidental diagnosis of TBAAD in this case was done for work up of an unrelated medical problem. This is truly a rare case that prevented a potentially life-threatening condition.
1325
Aortic tumor and a lower extremity undifferentiated pleomorphic sarcoma
St. Luke’s Medical Center - Quezon City, Quezon City, Philippines
Background: Undifferentiated pleomorphic sarcoma (UPS) is part of a rare heterogenous group of malignant tumors, most of which arising from soft tissues. Primary malignancy or metastasis to the aorta are both rare, with symptoms being similar to nonmalignant vascular diseases, making the diagnosis difficult and management complex. This case report describes a 62-year-old female presenting with a left thigh mass, with concomitant chest and back pain.
Results: The patient underwent contrast tomography aortogram revealing a lobulated mass in the descending aorta with possible transmural extension (see Fig.). Biopsy of the left thigh mass was done revealing undifferentiated pleomorphic sarcoma. Chemotherapy was contemplated but risk of aortic dissection or rupture was considered. Endovascular aortic repair (EVAR) with graft placement was offered for aortic protection prior to chemotherapy, but patient consent was not given and palliation was pursued.
Conclusion: Aortic undifferentiated pleomorphic sarcoma is rare. Chemotherapy is the recommended management for UPS. EVAR with graft placement can provide protection from aortic dissection or rupture.
Case Report 1325 Figure.
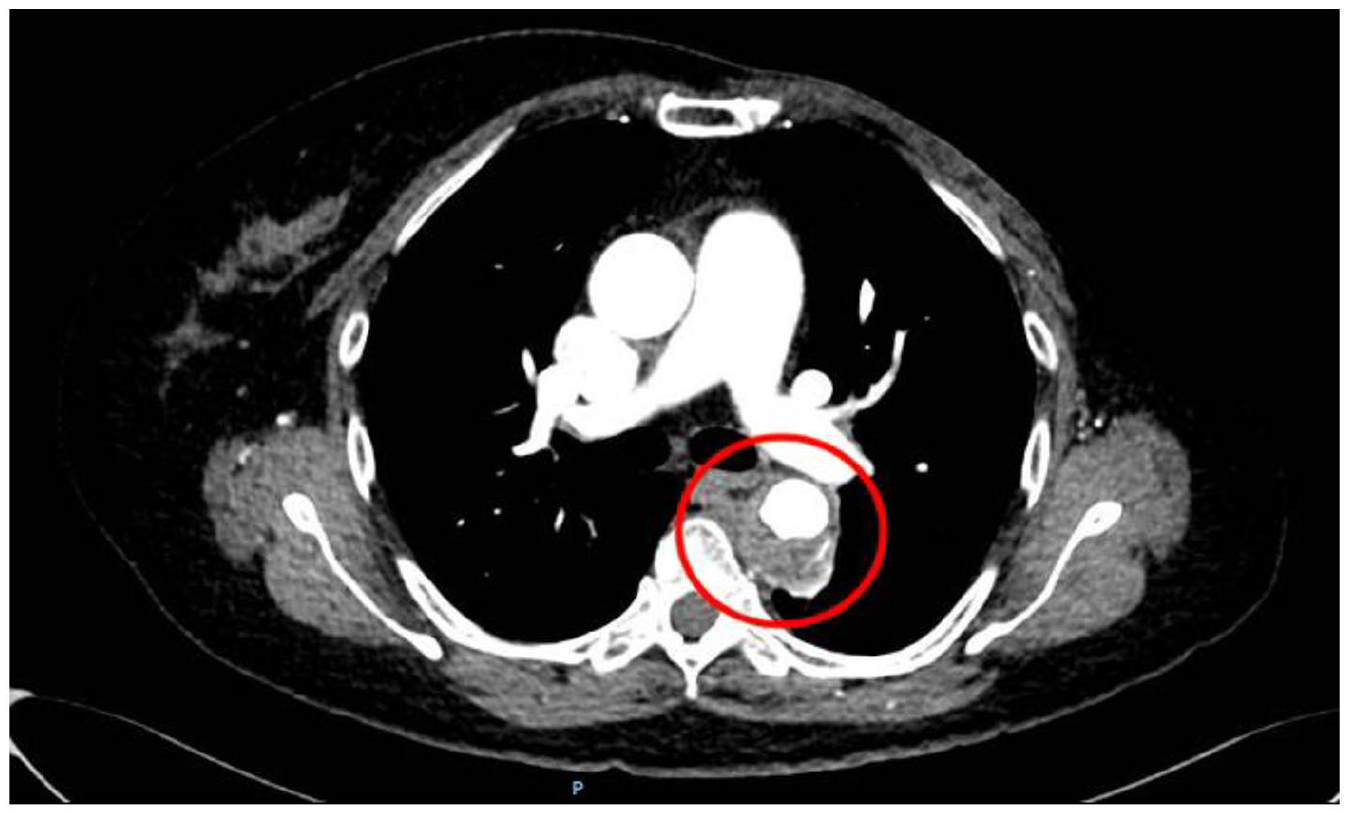
1328
Palliative subclavian stenting in a patient with a highly vascular metastatic histiocytic sarcoma with arterial invasion
1University of Arizona/Banner Health, Phoenix, AZ; 2University of Texas, Houston, TX; 3Yale University, New Haven, CT
Background: Subclavian artery stenting has been indicated in patients with subclavian steal syndrome secondary to chronic occlusions, acute limb ischemia, trauma, and iatrogenic perforations. We hereby present an unusual scenario of subclavian artery stenting in a patient with recurrent infiltrative and highly vascular tumor.
Methods: A 52-year-old male, receiving palliative chemotherapy for histiocytic sarcoma, presented to the hospital for newly noticed left shoulder mass. A non-contrast computed tomography showed a large heterogenous soft tissue mass superior to the left clavicle with erosion of the clavicle measuring 11 x 0.1 x 8.4 cm. A contrast computed tomography of head and neck showed multifocal lymphadenopathy above the diaphragm and large necrotic left supraclavicular lymph nodes with probable invasion into left subclavian artery.
Results: Considering the overall poor prognosis and patient not being a surgical candidate, we planned for subclavian covered stent placement for two major reasons 1. To avoid invasion of the left subclavian artery by the highly infiltrative sarcoma 2. To cut off the feeding vessels to the tumor so as to help reduce tumor size as a palliative attempt. An aortic arch angiogram was done, and the vertebral artery and IMA were found to be patent. There was no evidence of subclavian artery invasion but there was extensive vascularity to the tumor. intravascular ultrasound revealed luminal diameter of 7 mm. An 8 x 150 mm Viabahn (Gore Medical) covered stent was delivered and was post dilated with a 10 x 80 mm Mustang balloon (Boston Scientific Corporation). Post procedural angiogram showed well deployed subclavian stent with patent vertebral artery flow. He was discharged home on dual anti platelet therapy and had one month follow up with Oncology in clinic for further evaluation for chemotherapy.
Conclusion: In our patient, subclavian stenting was not performed for a guideline defined indication. This is a unique scenario with a goal of avoiding compression/invasion of the subclavian artery and also to reduce vascularity to the tumor. To our knowledge, this is the first case report of palliative subclavian artery stenting in a patient with recurrent infiltrative tumor.
1341
Venous purple toe syndrome: a variant of acrocyanosis
Providence Heart Institute, Portland, OR
Background: Acrocyanosis is commonly described as a painless condition characterized by discoloration of different shades of blue in the distal parts of the body that is marked by symmetry and persistence of color changes aggravated by cold exposure. The venous variety is often mischaracterized as blue toe syndrome, Raynaud’s phenomenon or pernio. This is first report of this variant.
Case: Retired female presents for 2nd opinion in regard to purple discoloration of toes. First noticed in past Winter with feet exposed to cold floors. Has been improving with warmer temperature in weeks of Spring. Patient with normal pulse examination. Toe discoloration resolves with elevation. See Figure.
Discussion: During COVID-19 pandemic more people are spending time indoors without shoes and often socks and as a result more frequently identify toe and foot discoloration. Patients can present for concern only about discoloration, but there can be foot pain and ulceration when noted in cooler months. A subclassification of acrocyanosis has venous congestion component. On presentation toes and sometimes entire foot have deep purple coloration. This can be distinguished from other arterial and vasospastic disorders in that this resolves with leg elevation and massage in cephalad direction. See picture for typical presentation.
Conclusion: Discoloration improves with compression which is hallmark. When present because of foot deformity that is not correctable warming measures can be helpful as well as potentially bioflavonoids.
Case Report 1341 Figure.

1350
Pulmonary leukostasis: an important differential of pulmonary embolism
Alta Vista Regional - Burrel School of Medicine, Las Vegas, NM
Background: Acute respiratory failure in the absence of infection requires a thorough assessment of the patient’s medical history in search for alternative diagnoses. A 60-year-old male with a not so distant history of cerebrovascular accident presented to the ER with a 1-week history of progressive respiratory failure. The patient was uncomfortable with tachypnea and tachycardia. He required 2 liters via nasal cannula to maintain good oxygen saturations.
Methods: His initial hemoglobin was 5.7 g/dL for he received two pRBC units; no source of bleeding was found. All other labs deemed to be processed incorrectly were repeated. Despite blood transfusions, hypoxia did not improve. Repeat labs confirmed what once thought to be an error: WBC count was 366 x 103/uL. Peripheral smear showed blast, promyelocyte, and myelocyte predominance (10, 50, and 31, respectively.) CT lung with contrast was not performed due to renal failure (creatinine 3mg/dL.) Review of the literature shows that mismatched perfusion defects in a ventilation/perfusion scan (V/Q scan) do not aid with the differential diagnosis. Like pulmonary embolism, infiltration of leukemic cells and hyperleukocytosis can mimic emboli effect.
Results: As a result, we initiated the patient on treatment for pulmonary leukostasis with hydroxyurea 1g PO. A repeat WBC showed a 25% decreased count (WBC 280 x 103/uL) following clinical improvement and complete oxygen independence within 3 hours of initiating therapy.
Conclusion: This case underscores the importance of identification of the cause of disease and prompt initiation of therapy without hesitation or waiting for confirmatory imaging that may eventually render no specific findings. It also highlights the significance of vascular medicine beyond red blood cells, platelets, and coagulation.
1356
The infectious tale of Aerococcal aortic endocarditis: cardiac pacing in acute aortic insufficiency with complete heart block as a bridge to aortic valve replacement
1Arnot Ogden Medical Center, Elmira, NY; 2Allegheny Health Network, Pittsburgh, PA
Background: We describe a rare case of Aerococcus endocarditis causing aortic insufficiency (AI) and paravalvular abscess presenting as complete heart block (CHB) and shock.
Case: A 76-year-old man with diabetes mellitus presented to the emergency department with fever and dyspnea. Vital signs were temperature of 102.4 F, heart rate (HR) 59 beats per minute (bpm), blood pressure 105/44 mmHg, 98% on 6L oxygen. Examination revealed a 2/6 diastolic murmur and diminished lung sounds at the bases. Lab data showed leukocytosis 19.65 k/mcL, acute kidney injury BUN 72 mg/dL and creatinine of 2.92 mg/dL, lactic acid 3.1 mmol/L, pro-BNP 15,342 pg/ml, high sensitivity troponin 136 ng/L, AST 129 U/L and ALT 115 U/L. Electrocardiogram showed CHB (Fig. 1A). Transthoracic echocardiogram showed normal biventricular function, AI and hypokinetic mid-distal anteroseptal segments. Transvenous pacemaker was placed and set at 100 bpm. Blood cultures grew Aerococcus urinae. Transesophageal echocardiogram showed an aortic root abscess and severe AI (Fig. 1B). Ventricular pacing was used to optimize computed tomography with gating to view the coronary arteries (Fig. 1C). His aortic valve was replaced (Fig. 1D) and a pacemaker was planned.
Discussion: Aortic valve Aerococcus endocarditis is rare and can lead to CHB and AI. Cardiac pacing improves hemodynamics by increasing HR, decreasing left ventricular end-diastolic pressure, pulmonary arterial wedged pressure and increasing cardiac index by decreasing diastolic time.
Case Report 1356 Figure.
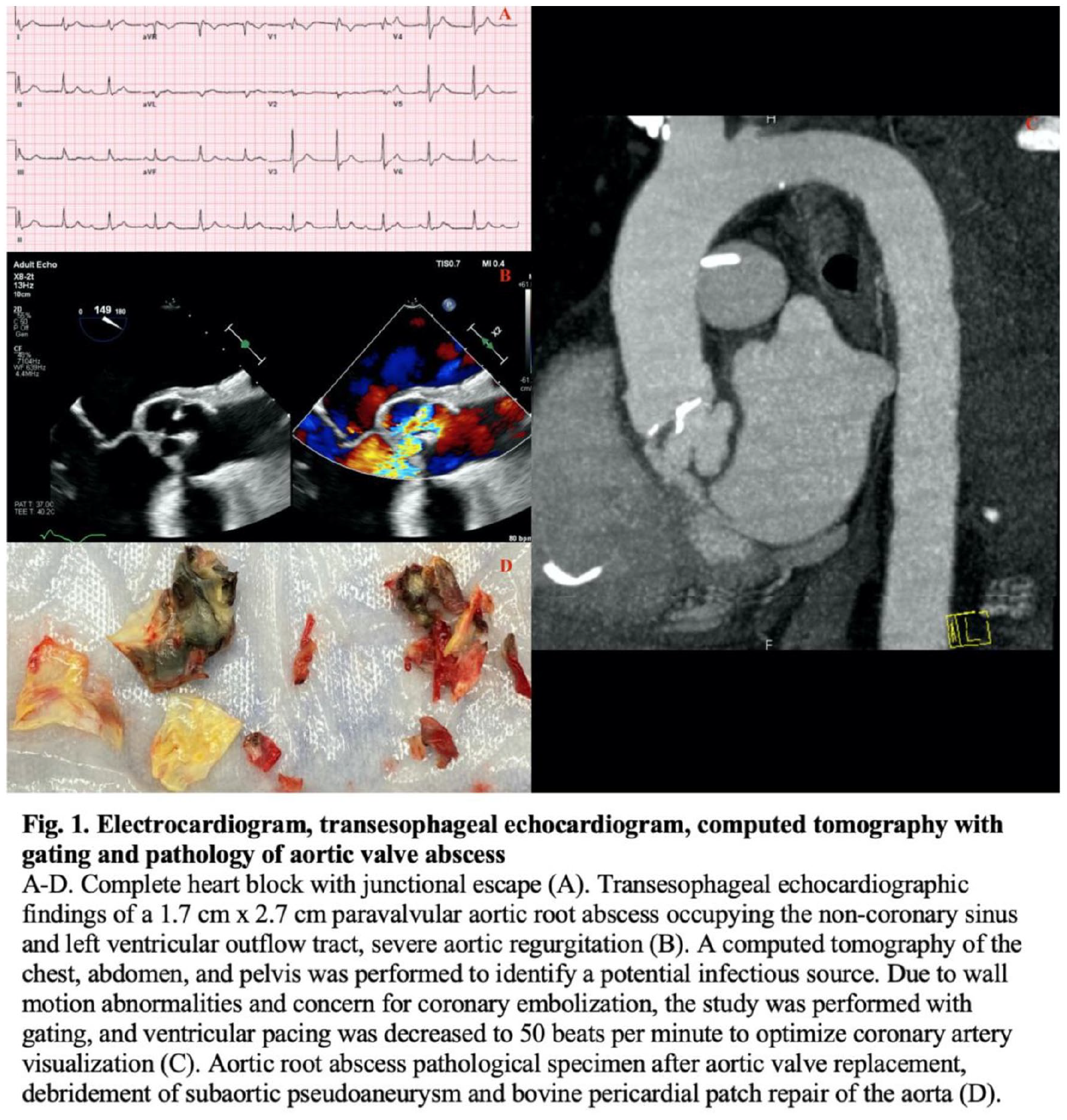
1364
Chronic type B aortic dissection in a pregnant patient: a case report
Philippine Heart Center, Quezon City, Philippines
Background: Chronic aortic dissection in a pregnant patient is not widely reported. Together with its rarity is the high risk of mortality it carries to both the mother and the fetus.
Methods: We report a case of a 33-year-old female with a four-year history of Stanford B DeBakey III aortic dissection. She had a normal aortic Z score and satisfied only two systemic criteria of the Ghent nosology. She had been asymptomatic and with stable aortic diameters. However, she was found to be pregnant at 5 weeks age of gestation, gravida 3 para 2.
Results: Patient continued her prenatal check-ups and was maintained on antihypertensive medications. She was admitted at 37 weeks age of gestation and delivered a healthy baby via cesarean section without complications.
Conclusion: The strategy of optimizing antihypertensive therapy and delivery via cesarean section proved to be successful in this case. But we cannot overemphasize the importance of multidisciplinary management and individualized treatment to provide survival opportunities for both the mother and the fetus.
1403
A case report on hybrid procedure in the treatment of a 75-year-old male with thoracoabdominal aneurysm
Marrah Angela Comia, Precious Samonte
Philippine Heart Center, Quezon City, Philippines
Thoracoabdominal aortic aneurysm commonly occurs in the elderly population with comorbidities. The author presents a case of successful TAAA repair in a 75 year-old male, hypertensive, with COPD and coronary artery disease with 3 vessel involvement, using the hybrid approach. During the first stage, the abdominal segment of the aortic aneurysm was repaired using a bifurcated graft. This was followed by TEVAR during the second stage. Completion angiogram showed no endoleak. No neurologic deficit was noted postoperatively.
1410
An atypical presentation of aortic dissection and rupture involving coronary grafts
Arnot Ogden Medical Center, Elmira, NY
Background: Acute aortic Dissection (AAD) is a catastrophic disorder; diagnosis can be difficult and delayed due to an atypical presentation.
Case Presentation: The patient is a 68-year-old male with a history of coronary artery bypass (CABG) four years prior who presented to the emergency department with syncope, no chest or abdominal pain reported. His temperature was 97.5 F, heart rate 40 beats per minute, blood pressure 72/50 mmHg in both arms, and SPO2 98%. On the physical exam he was alert, oriented and pain free, the rest of the exam was unremarkable. Electrocardiogram showed normal sinus rhythm with no acute ischemic changes (Fig. 1A). Labs showed creatinine 1.2 mg/dL, lactic acid 9.1 mmol/L, and high sensitivity troponin 69 pg/mL. He was placed on vasopressor support. Computed tomography angiogram showed a Type A AAD (Fig. 1B-D). Transesophageal echocardiogram showed aortic insufficiency from a prolapsing flap into the non-dissected root. He underwent aortic repair with re-implantation of vein grafts. A contained rupture was seen in the posterior part of the ascending aorta with blood around the right atrium that was drained.
Conclusion: Type A AAD is associated with a mortality rate of 1-2% per hour and timely diagnosis is imperative for definitive surgical management. This case illustrates that atypical presentation can delay the diagnosis even with such an extensive complicated dissection.
Case Report 1410 Figure.
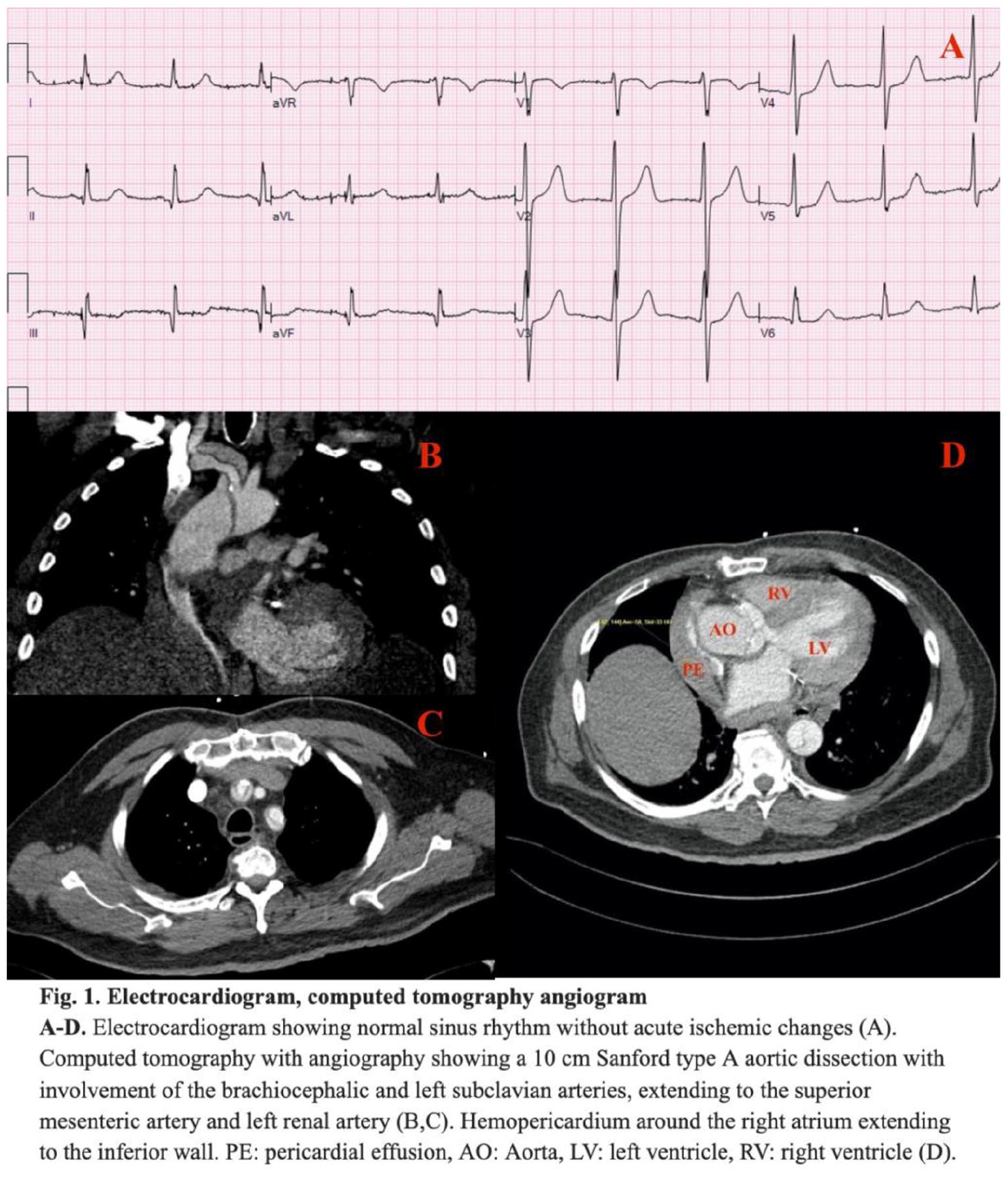
1411
Antiphospholipid antibody induction after infliximab treatment for inflammatory bowel disease
Cleveland Clinic, Cleveland, OH
Background: Tumor necrosis factor (TNF) antagonists are used in the treatment of broad classes of autoimmune disorders, including rheumatoid arthritis and inflammatory bowel disease (IBD). TNF antagonists are associated with the induction of antiphospholipid antibodies. As use of TNF antagonists increases, patients with autoimmune disorders may be falsely identified as having concomitant antiphospholipid syndrome (APLS). We review the case of an IBD patient previously treated with infliximab, who presented with GI bleeding and a history positive for antiphospholipid antibodies.
Case: A 55-year-old female with a history of Crohn’s disease and APLS presented with abdominal pain, GI bleed and small bowel obstruction. Vascular medicine was consulted for possible mesenteric ischemia secondary to APLS. Review of the patient’s history revealed APLS testing was done as part of autoimmune work up after a brain MRI in 2014 for headache revealed findings consistent with multiple sclerosis. The patient was being treated with infliximab at the time of testing. Testing was done six months apart and notable for markedly elevated Beta 2 Glycoprotein IgM >120 SMU and equivocally elevated Cardiolipin IgM with normal screen and mixing studies.
Treatment/Outcome: Vascular medicine consultation determined the patient did not have APLS, did not recommend anticoagulation, and recommended further IBD optimization. Upper and lower endoscopy revealed only non-bleeding esophagitis. MRA of the abdomen showed no stenoses, dissections or thromboses within the bowel vasculature. The patient underwent adhesion lysis with resolution of symptoms and was discharged without anticoagulation after the diagnosis of APLS was removed from her chart.
Conclusion: Antiphospholipid antibodies can be induced by treatment with TNF antagonists. These antibodies are not necessarily thrombogenic; however, their presence can lead to false diagnoses of antiphospholiplid syndrome and confound treatment plans. Awareness of antiphospholipid antibody induction by TNF antagonists can reduce misdiagnoses and avoid unnecessary anticoagulation in patients with inflammatory bowel disease, who already have elevated bleeding risk.
1412
Flying blind in a turkey shoot: a case of bow hunter’s syndrome
1Vanderbilt University School of Medicine, Nashville, TN; 2Department of Neurological Surgery, Vanderbilt University Medical Center, Nashville, TN; 3Division of Cardiovascular Medicine, Department of Medicine, Vanderbilt University Medical Center, Nashville, TN
Background: Bow Hunter’s Syndrome (BHS), or positional vertebrobasilar insufficiency, is a rare vascular syndrome in which vertebral arteries (VA) are occluded in a position dependent manner.
Methods: A 58-year-old man with history of T2/N2 squamous cell nasopharyngeal carcinoma treated via TPF (docetaxel, cisplatin, 5-FU) and radiotherapy presented with dizziness upon lifting or turning his head to the right. Turkey hunting resulted in syncope that significantly affected quality of life. There was no history of cervical trauma.
Results: CTA of the head and neck showed no fixed arterial occlusive disease. Cardiac monitoring was negative for arrhythmia. Tilt table testing was normal. Left VA velocities tripled with right head turn during carotid duplex. Transcranial doppler showed decreased basilar velocities in the same position. Dynamic catheter-based angiogram showed irregularities of the right VA felt secondary to prior radiation which worsened with neck flexion or rightward rotation. The left VA occluded with the same movements (Fig 1a) due to ponticulus posticus anomaly (Fig 1b). The patient underwent C1 decompression of the left VA resulting in significant improvement.
Conclusion: Impingement at the V1 segment secondary to bony spicule is unique as most reported cases occur in the V3-4 segments as a result of trauma or hypoplastic VA. This case highlights the importance of clinical suspicion, multimodality imaging and multidisciplinary care for patients with suspected BHS.
Case Report 1412 Figure.
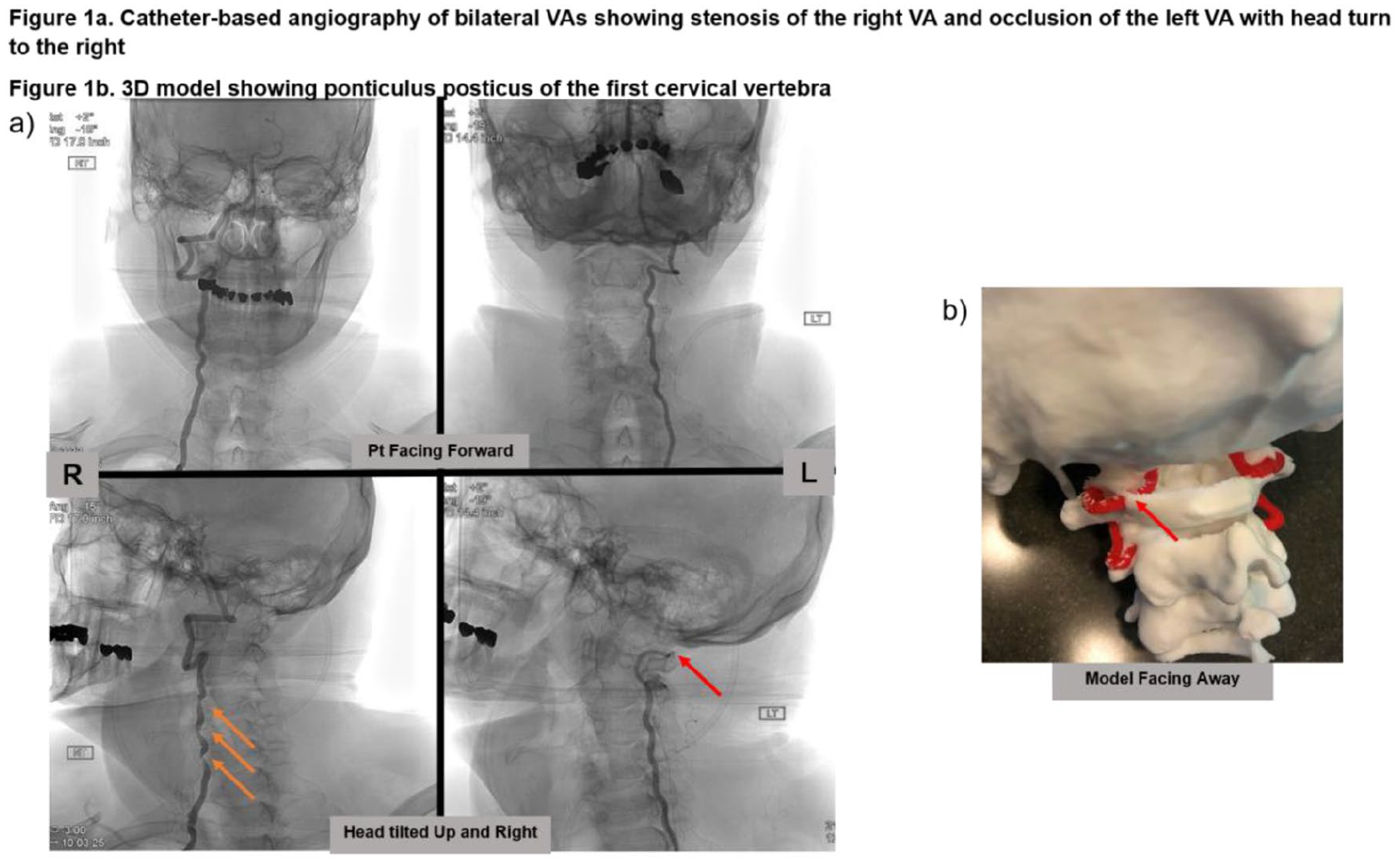
1421
Conservatively treated complicated penetrating atherosclerotic ulcer of the infrarenal aorta and left common iliac artery in a 79-year-old patient with advanced atherosclerosis of the coronary and peripheral arteries - a case report
St. Luke’s Medical Center - Quezon City, Quezon City, Philippines
Background: Penetrating atherosclerotic ulcer (PAU) is a rare condition which occurs in 2-7% of acute aortic syndromes. The natural history remains unclear, and treatment remains controversial.
Methods: We report a case of a 79-year-old male, hypertensive, dyslipidemic, diagnosed case of peripheral artery disease (PAD) of the bilateral lower extremities, severe two vessel coronary artery disease (CAD) of the mid left anterior descending artery (LAD) and late mid segment of the obtuse marginal artery (OM), with incidental finding of saccular aneurysm in the infrarenal aorta and in the left common iliac artery originating from a penetrating atherosclerotic ulcer.
Results: Although surgical management is advocated in patients with complicated PAU such as saccular aneurysm formation in case reports and small case series-due to the presence of significant comorbidities and high surgical risk, a conservative approach was opted for the patient with radiologic surveillance and antihypertensives using beta blocker (BB) and calcium channel blocker (CCB).
Conclusion: Because patients with PAU often suffer from significant comorbidities, conservative management may be suitable so that consideration of these factors should therefore play an important role in the management decisions.
1423
Spinal dural AVF-a rare differential for claudication
Department of Radiology, Creighton University School of Medicine, Omaha, NE
Background: Spinal dural arteriovenous fistula (dAVF), a rare cause of neurogenic claudication, is an important differential consideration with the possibility of permanent physical disability. Here, we present a case of a 62-year-old female with history of severe obesity and knee and back pain, who had a relapsing remitting pattern of symptoms found to have spinal dAVF.
Methods: Spinal MRI (see Fig.) showed increased T2 signal within the cord from T5 through the conus with adjacent increased flow voids suspicious for spinal dAVF. A spinal angiogram localized a dAVF arising from right L1 lumbar artery with increased venous congestion at the mid-lower thoracic spine with subsequent surgical resection of the L1 dAVF.
Results: The patient had an uneventful postoperative course with discharge on postoperative day 3 with outpatient therapy. She was slowly gaining strength with ambulation using a walker with progress complicated by comorbidities.
Conclusion: Spinal dAVF is a rare cause of neurogenic claudication that can lead to permanent impairment. Spinal MRI is the gold standard for initial diagnosis. Angiographic localization precedes surgical or endovascular treatment that can be successful in up to 98% and 75% of cases, respectively.
Case Report 1423 Figure.

1426
It’s Alive: Biologically Active Thrombus and Implications for Vascular Remodeling
1University of Rochester, Rochester, NY; 2Cleveland Clinic, Cleveland, OH
Background: The decision to supplement anticoagulation with catheter-directed therapy (CDT) to treat patients with venous thromboembolism (VTE) remains controversial. In addition, the absence of mechanistic data and unclear patient selection criteria make universal use of CDT challenging to justify. Our goal was to determine the cellular content and biochemical activities of thrombus extracted during CDT to gain additional insight into pathological vascular remodeling.
Methods: Thrombus extracted by catheter in 27 patients with VTE consisting of deep vein thrombosis (DVT, n = 5), pulmonary embolism (PE, n = 9) and acute thrombotic stroke (AT, n = 13) was evaluated by 2-dimensional electrophoresis (2DE) and by immunoblotting (IB) for marker of platelets (CD42), white blood cells (WBC, CD45), and red blood cells (RBC, CD235A). Matrix metalloproteinase (MMP) isoforms were determined by reverse transcriptase quantitative polymerase chain reaction (RT-qPCR) and confirmed by IB. MMP isoform activity was determined by in-gel zymography and validated for isoform catalytic activity using a chromogenic enzymatic substrate.
Results: Protein content in 7-mg extracted thrombus was greater in patients with VTE vs. AT (p = 0,046). CD42 was similar in VTE vs. AT thrombus while CD45 (p = 0.047) and CD235A (P = 0.001) were greater in VTE. Only CD235A was greater in PE vs. DVT thrombus (P = 0.002). Gel zymography identified enzymatic activity of many MMP isoforms in VTE and AT. Of the 10 MMP isoforms assessed, only the following were identified in both VTE and AT: MMP 1, 2, 8, 9, 10, 14. Protein content was greater in VTE vs. AT by IB for: MMP1 0.79 ± 0.13 vs. 0.43 ± 0.12, p = 0.02, MMP2 (0.30 ± 0.08 vs. 0.17 ± 0.03, p = 0.05), and MMP9 (1.3 ± 0.38 vs. 0.26 ± 0.06, p = 0.009). MMP9 activity was far greater in thrombus from patients with VTE vs. AT (12477 U ± 1618 vs. 4846 U ± 1119 per mg/mL protein, p = 0.0008).
Conclusion: These data provide mechanistic insight regarding the biochemical susceptibility of thrombus to tissue plasminogen activator and potential for thrombus to irreversibly remodel blood vessels. Thrombus-derived biomarkers with respect to therapy initiated should be prospectively evaluated in patients with VTE and stroke.
1427
Tumor thrombosis of the internal jugular vein in a patient with follicular thyroid carcinoma
Cleveland Clinic, Cleveland, OH
Background: Tumor extension into the vascular lumen is known as tumor thrombus. Duplex venous ultrasound plays a significant role in the diagnosis of tumor thrombus of the head and neck.
Case presentation: A 53yo woman presented with right neck swelling, with history of follicular thyroid carcinoma (FTC) status post total thyroidectomy in 2014. Physical examination revealed exophthalmos, well healed surgical scar, visibly full right neck, painless fixed lymphadenopathy. Contrast CT of the neck showed FTC recurrence and right internal jugular vein occlusion. She was referred to Vascular Medicine clinic and Non-Invasive Vascular Laboratory.
Results: Right upper extremity Duplex venous ultrasound was performed using a Phillips Epic ultrasound system with a 3-12 MHz linear probe. Tumor thrombosis extended segmentally from the thyroid carcinoma into the mid to distal right internal jugular vein (Fig 1A). There was characteristic pulsatile tumor enhancement on color power angio (Fig 1B), and arterialized flow on pulsed wave and color Doppler (Fig 1C).
Conclusion: FTC invasion of the internal jugular vein is rare and is associated with worse prognosis. Duplex venous ultrasound can help differentiate between deep vein thrombosis and tumor thrombosis. Tumor debulking and thrombectomy is first line treatment in tumor thrombosis and anticoagulation is not indicated. Our patient is scheduled for surgical debulking of the tumor by ENT/Endocrine Surgery in collaboration with Vascular Surgery for thrombectomy.
Case Report 1427 Figure.
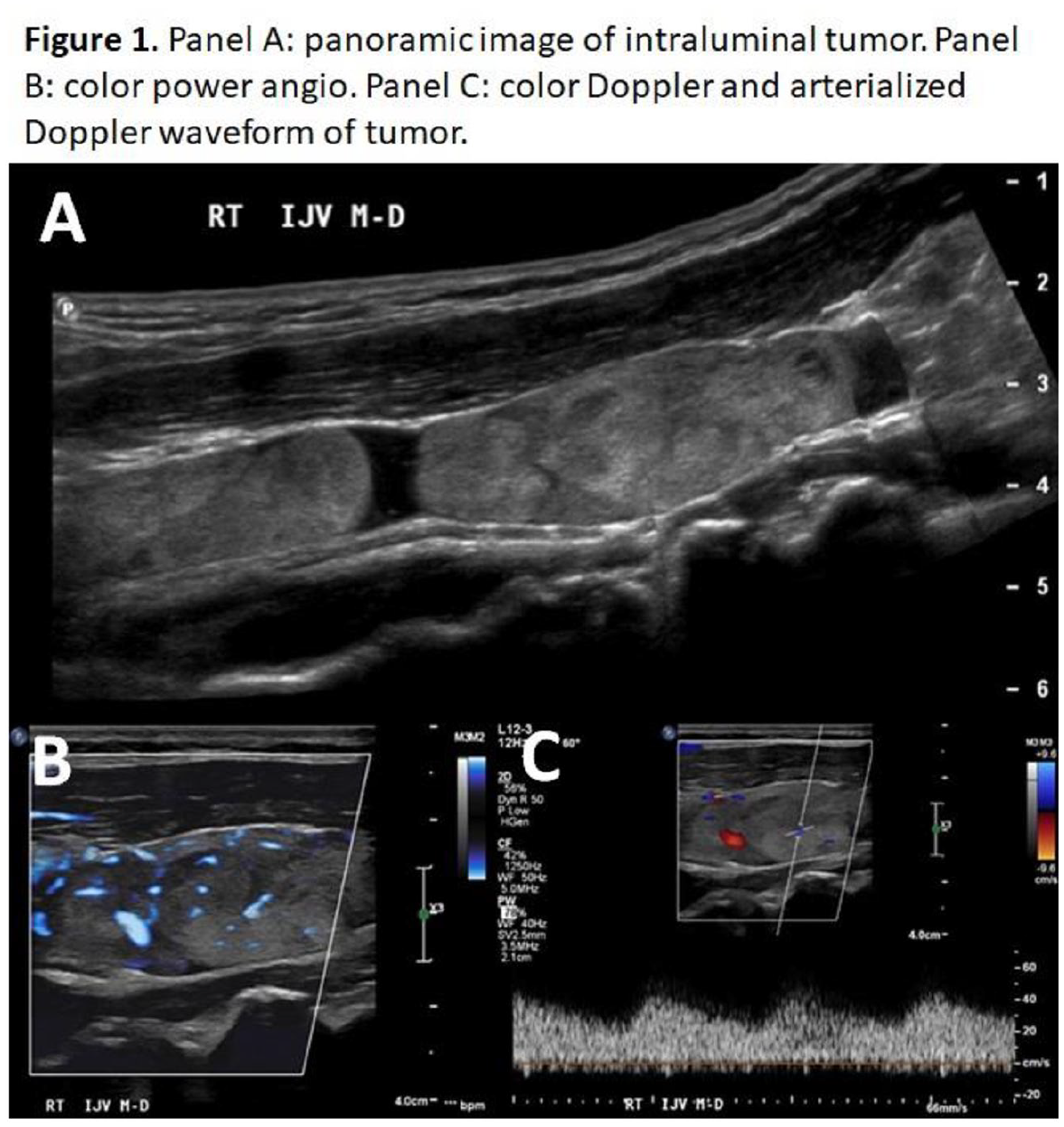
1429
Biopsy-proven diagnosis and treatment of non-uremic calciphylaxis
1OhioHealth Doctors Hospital, Columbus, OH; 2OhioHealth Riverside Methodist Hospital, Columbus, OH
Calciphylaxis is a rare condition characterized by vascular medial calcification of small arterioles that can have different clinical presentations depending on the organ system involved but commonly affects the skin. This is a disease characterized by small vessel calcification leading to dermal ischemia, and the skin changes ultimately lead to non-healing necrotic tissue. Calciphylaxis is usually associated with end-stage kidney disease (ESKD), but even in this cohort, it is rare and occurs around 1% of the time. When patients without renal impairment develop necrotic tissue consistent with calciphylaxis, it is termed non-uremic calciphylaxis (NUC). Cutaneous biopsy is diagnostic of this disease (see Fig.). Management is usually wound debridement, control of infection and risk factor modification. We present a case of a 65-year-old male with lower limb NUC which responded to daily wound care with complete ulcer healing.
Case Report 1429 Figure.
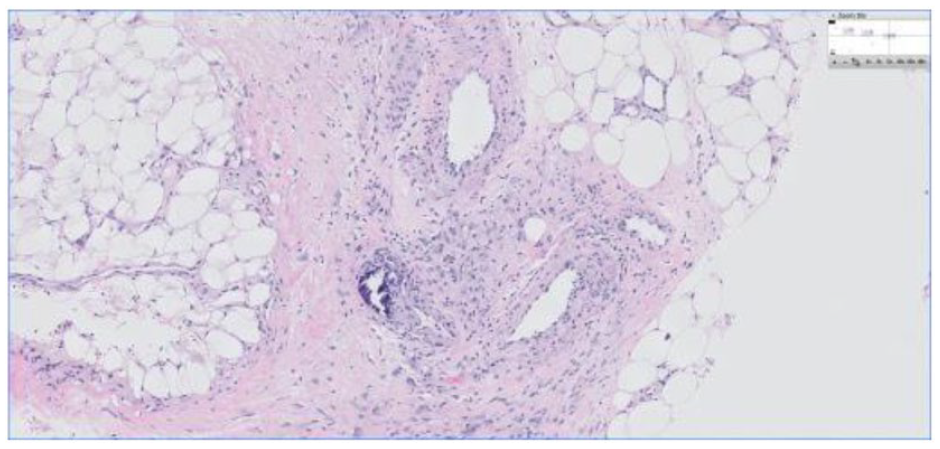
1434
Unique presentations of aortic graft infection-small bowel obstruction and gastrointestinal bleeding
Department of Radiology, Creighton University School of Medicine, Omaha, NE
Background: Vascular graft infections represent an uncommon life- and limb-threatening complication after surgical graft and endograft placement. The prototypical presentation is fever, pain/swelling over the graft site, and sepsis. We present two unique cases of aortic graft infection: a 70-year-old man with bowel obstruction from ventral hernia, and a 73-year-old man presenting with rectal bleeding, mild anemia, and leukocytosis.
Methods: Retrospective chart review was performed for both patients. The patients’ CT imaging was reviewed including multiplanar reformations and volume-rendered reconstructions. Literature review of vascular graft infection was performed.
Results: Both patients were imaged with intravenous contrast-enhanced CT of the abdomen and pelvis. The first patient’s imaging demonstrated a gas-containing fluid collection across the aortoiliac endograft, with secondary mass effect that may have contributed to a ventral hernia with associated bowel obstruction. The second patient’s imaging demonstrated bowel gas from sigmoid diverticulitis communicating with an internal iliac aneurysm at the margin of an aortoiliac graft. Surgical treatment found graft infections in both patients relating to communication with the colon, both requiring colon resections with colostomy and cadaveric graft placement. The first patient initially improved after surgery, but subsequently developed graft thrombosis and succumbed to his disease during the hospital stay. The second patient recovered and was discharged on antibiotics.
Conclusion: Aortic graft infections are severe complications of vascular surgery with the potential for atypical clinical presentations. Even with prompt surgical treatment, mortality from this condition is high and outcomes may depend on patient comorbidities.
1436
The x factor- using chromogenic factor x to monitor oral anticoagulation therapy in patients with thrombotic anti-phospholipid syndrome
University of Oklahoma Health Sciences Center, Oklahoma City, OK
Background: Patients with thrombotic anti-phospholipid syndrome (APLS) need appropriate life-long anticoagulation with warfarin. Patients with positive lupus anticoagulant can have falsely high Internal Normalized Ratio (INR) values. Chromogenic Factor X (CFX) is a laboratory test that remains unaffected by the many variables that seem to alter INR. Studies have shown that it can be used reliably to monitor patients on oral anticoagulation therapy with warfarin since it is a phospholipid-independent test.
Methods: We present a case of triple positive APLS who had artifactual INR values on each clinic visit. His oral anticoagulation therapy was successfully monitored by assessing their factor X levels using a chromogenic substrate. On his visit to a different facility, his INR was reversed under the impression that the high levels were secondary to warfarin toxicity. This unfortunately led to his demise.
Results: Chromogenic Factor X is a phospholipid independent test which can be used safely to monitor OAT in patients with artifactual INR. In general, there appears to be an inverse correlation between CFX and INR. However, we do not have defined therapeutic protocols established for using CFX to monitor oral anti-coagulation therapy. Individuals, such as our patient would ideally be anti-coagulated to a goal INR of 2-3 but given lack of clear guidelines, we managed to anti-coagulate him based on rough estimated outlines of CFX therapeutic ranges (40-23%).
Conclusion: Patients with dysfibrinogenemia, or on direct thrombin inhibitors can have unreliable INR values which can lead to inaccurate dosage adjustments of oral anti-coagulation therapy. It is of vital importance to identify these individuals and find alternate methods to reliably monitor oral anti-coagulation therapy in these individuals.
1439
Portal vein anastomotic stent thrombosis in a polycythemia vera patient after liver transplant
Cleveland Clinic, Cleveland, OH
Background: Polycythemia vera (PCV) and essential thrombocytosis (ET) are associated with JAK2 mutation and portal vein thrombosis (PVT). Few studies exist to guide anticoagulant selection in patients with portal vein stents and thrombophilias.
Case: A 42-year-old female with a history of PCV/ET, prothrombin mutation, PVT, and liver transplant complicated by portal vein anastomotic site stenosis requiring stenting presented with new abdominal pain and ascites. Imaging demonstrated totally occlusive portal vein stent thrombosis and persistent portosystemic shunts (see Fig.). Patient was adherent with aspirin and warfarin prior to presenting.
Treatment/Outcome: The patient was treated with IV heparin but did not improve. Balloon venoplasty and mechanical thrombectomy were unsuccessful. The patient received successful TIPS and repeat thrombectomy. The patient continued daily aspirin and was bridged back to warfarin.
Conclusion: Portal venous stents in hypercoagulable patients are at risk for thrombosis. Selection of the appropriate antiplatelet and anticoagulant, as well as adherence monitoring, are critically important to prevent stent thrombosis. In the setting of portosystemic shunts from previous portal hypertension, direct lysis or thrombectomy for completely thrombosed stents may be more effective than systemic anticoagulation.
Case Report 1436 Figure.
