
Abstract

Over the past two decades, the primary treatment paradigm for chronic mesenteric ischemia (CMI), most frequently caused by superior mesenteric artery (SMA) occlusive disease, has shifted from open surgical towards endovascular therapies. However, endovascular therapies are associated with up to 50% lower primary patency rates largely due to in-stent restenosis (ISR). 1 The 2020 Society for Vascular Surgery Clinical Practice Guidelines recommend post-stenting surveillance using duplex ultrasound (DUS). 2 However, there are no consensus duplex criteria for SMA ISR.
Previous studies have demonstrated that DUS velocity criteria for stenosis of the native, or unstented, SMA overestimate SMA ISR, potentially resulting in unnecessary diagnostic testing. 3 Despite the efforts of prior studies with modest sample sizes,4–7 there are no consensus DUS velocity criteria for predicting SMA ISR. Furthermore, most of these studies compared DUS to digital subtraction angiography (DSA) studies, the traditional gold standard for duplex velocity validation. However, in real-world practice, computed tomography angiography (CTA) is frequently utilized to assess recurrent restenosis.2,8 Thus, the goal of this study was to identify optimal DUS velocity criteria for SMA ISR using both DSA and CTA.
We performed a retrospective cohort study of patients who underwent SMA stenting in the Division of Vascular Surgery at Northwestern Memorial Hospital (Chicago, IL) between 2014 and 2020. The study protocol was approved by the Northwestern University Institutional Review Board. Postoperative CTA or DSA performed within 3 months of DUS were selected for inclusion as a ‘paired’ study. All DUS were performed by a Registered Vascular Technologist credentialed by the American Registry for Diagnostic Medical Sonography in a vascular lab accredited by the Intersocietal Accreditation Commission.
Angiographic SMA ISR was quantified by two independent reviewers using electronic calipers from CTA and DSA studies. In the case of CTA studies, the minimum diameter from axial, sagittal, and coronal planes was used (online Supplemental Figure 1). A third independent reviewer was used to adjudicate disagreements between the other reviewers. Percentage stenosis was averaged across all reviewers. Maximum peak systolic velocity (PSV) and end diastolic velocity (EDV) in the stented SMA were recorded from each paired DUS study. Receiver operator characteristic (ROC) curves were constructed to determine optimal PSV and EDV thresholds for detecting ⩾ 70% angiographic ISR using the closest top-left method.
During the study period, 116 patients underwent SMA stenting. Among these, a total of 48 paired DUS and angiographic studies in 25 patients (mean age 68 years, 72% female) were eligible for analysis. Eleven patients had one paired study and 14 patients had two or more paired studies. DSA was used in 22 of the paired studies (46%) and CTA in 26 of the paired studies (54%). There was ⩾ 70% angiographic ISR in 12 paired studies (25%) from nine patients. PSV (556 vs 331 cm/s, p < 0.001) and EDV (155 vs 76 cm/s, p < 0.001) were both significantly higher in paired studies with ⩾ 70% ISR than those with < 70% ISR.
Using ROC analysis, the optimal DUS criteria for predicting ⩾ 70% SMA ISR were PSV ⩾ 457 cm/s (sensitivity = 100%, specificity = 97.2%) (Figure 1A) and EDV ⩾ 81.6 cm/s (sensitivity = 91.7%, specificity = 74.3%) (Figure 1B). PSV was a modestly better predictor of ⩾ 70% SMA ISR than EDV (AUC: 0.975 vs 0.848, p = 0.047). Sensitivity, specificity, and positive and negative predictive values were calculated across a range of thresholds for PSV and EDV (Table 1). Based on these criteria, there was one false positive study and no false negative studies.
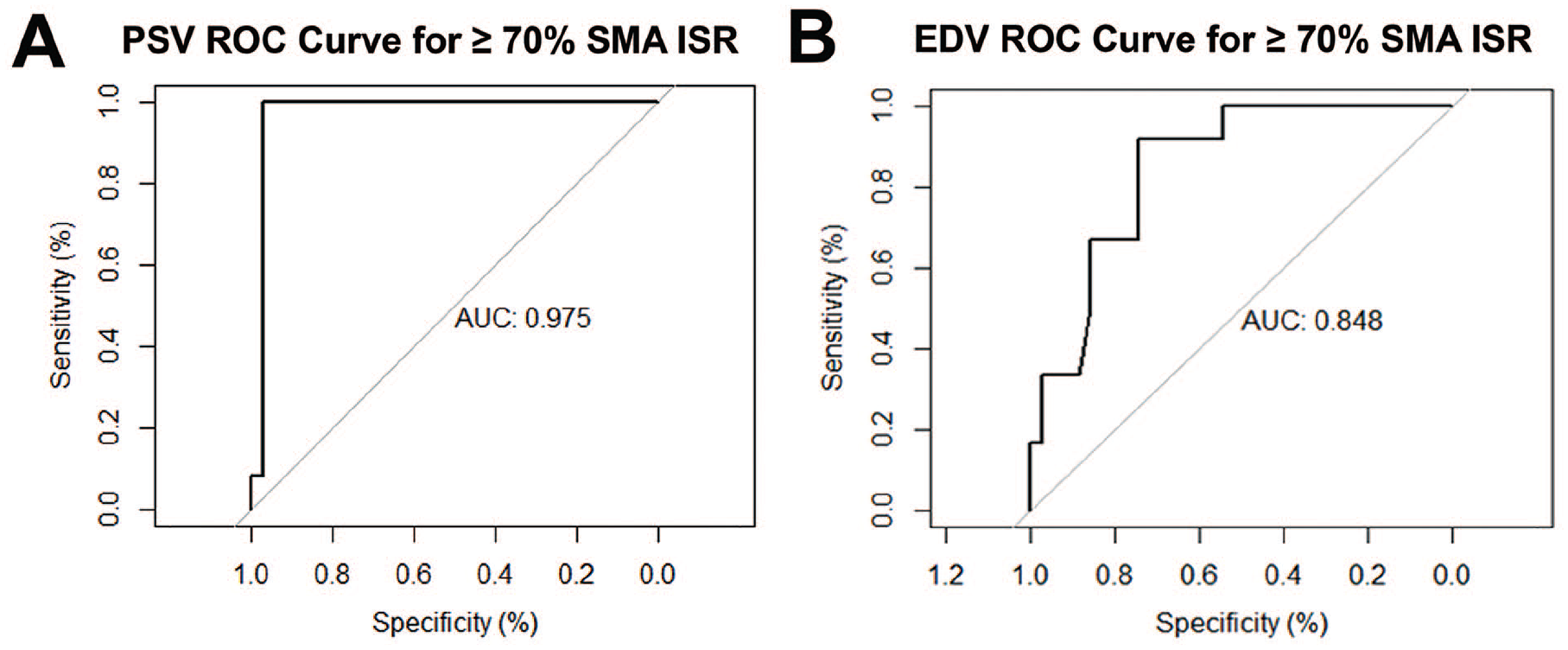
Determination of optimal duplex ultrasound criteria for superior mesenteric artery in-stent restenosis. Receiver operator characteristic curve for ⩾ 70% angiographic stenosis for peak systolic velocity
Peak systolic velocity and end diastolic velocity thresholds for ⩾ 70% superior mesenteric artery in-stent restenosis.
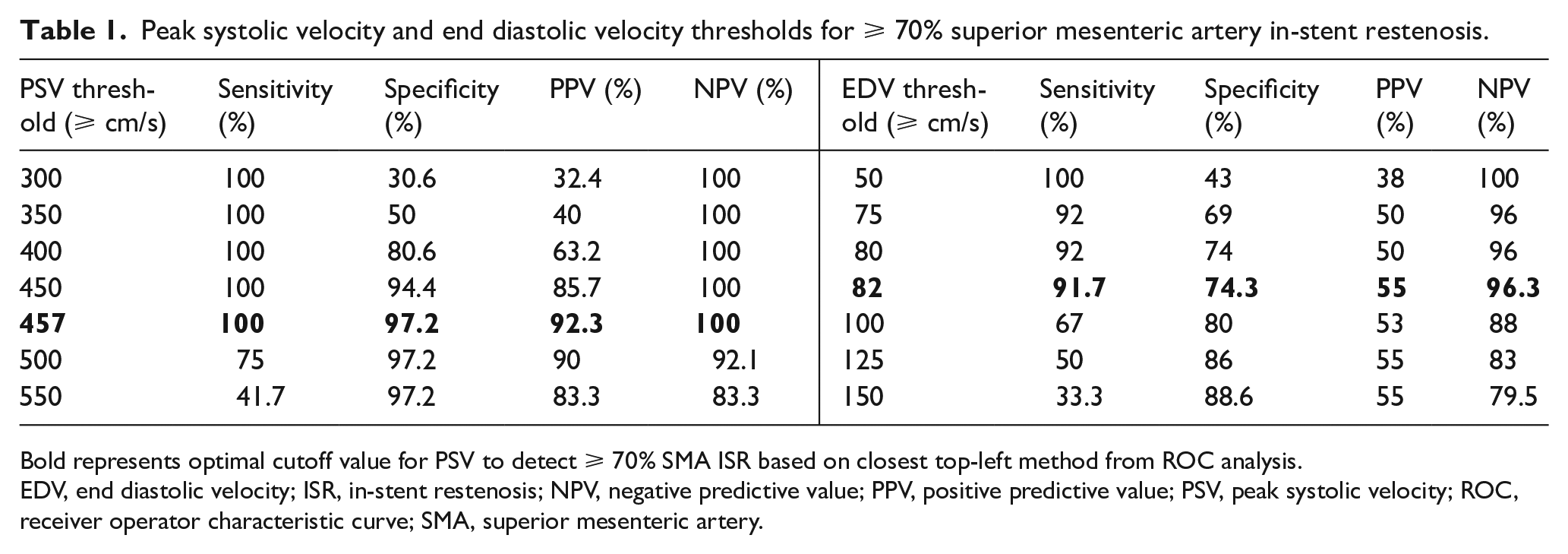
Bold represents optimal cutoff value for PSV to detect ⩾ 70% SMA ISR based on closest top-left method from ROC analysis.
EDV, end diastolic velocity; ISR, in-stent restenosis; NPV, negative predictive value; PPV, positive predictive value; PSV, peak systolic velocity; ROC, receiver operator characteristic curve; SMA, superior mesenteric artery.
In concordance with prior studies,4–7 our study indicates that DUS velocity criteria of PSV ⩾ 275 cm/s 9 corresponding to ⩾ 70% native SMA stenosis overestimates SMA ISR. Furthermore, we found that PSV is a modestly better predictor of ⩾ 70% SMA ISR than EDV (p = 0.047), with a threshold PSV ⩾ 457 cm/s providing a sensitivity of 100% and specificity of 97.2%. Study characteristics and DUS velocity criteria comparing the present study to prior studies4–7 are presented in online Supplemental Table 1. Notably, our study had a lower percentage of paired studies with ⩾ 70% ISR (n = 12/48, 25%) compared to the other studies. A likely explanation is the inclusion of CTA in our study: patients undergoing DSA have a higher a priori probability of high-grade SMA ISR than those undergoing CTA given that DSA is often used in cases where clinical factors justify probable endovascular re-intervention.
With the increased use of stents as a primary treatment modality for CMI, it is of practical value to establish validated DUS velocity criteria for SMA ISR. Our study is limited by its retrospective single-center nature and modest sample size. Future larger research studies utilizing CTA in addition to DSA, prospective multicenter study design, longitudinal comparisons with post-stent DUS data, and multivariable modeling to incorporate patient and clinical factors will help delineate guidelines for management of SMA ISR on postoperative surveillance imaging.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X211025615 – Supplemental material for Use of computed tomographic and digital subtraction angiography to determine optimal duplex ultrasound criteria for predicting superior mesenteric artery in-stent restenosis
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X211025615 for Use of computed tomographic and digital subtraction angiography to determine optimal duplex ultrasound criteria for predicting superior mesenteric artery in-stent restenosis by Vivek Pamulapati, Joan R Guitart, Irene B Helenowski, Scott Resnick and Karen J Ho in Vascular Medicine
Supplemental Material
sj-pdf-2-vmj-10.1177_1358863X211025615 – Supplemental material for Use of computed tomographic and digital subtraction angiography to determine optimal duplex ultrasound criteria for predicting superior mesenteric artery in-stent restenosis
Supplemental material, sj-pdf-2-vmj-10.1177_1358863X211025615 for Use of computed tomographic and digital subtraction angiography to determine optimal duplex ultrasound criteria for predicting superior mesenteric artery in-stent restenosis by Vivek Pamulapati, Joan R Guitart, Irene B Helenowski, Scott Resnick and Karen J Ho in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Research reported in this publication was supported in part by the National Heart, Lung, and Blood Institute of the National Institutes of Health under Award Number T32HL094293 to VP. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. In addition, JG was supported by the William H Pearce, MD, Vascular Surgery Student Research Award, Feinberg School of Medicine, Northwestern University.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.