
Abstract
Introduction
Concurrent stenting of complex iliac lesions during infrainguinal bypasses can increase the complexity of a case and impact outcomes.
Objective
Our aim was to evaluate the effect of inflow stenting of TASC-II C, D iliac lesions on femoropopliteal bypass patency.
Methods
A retrospective observational cohort study of patients who underwent femoropopliteal bypass with TASC-II C, D iliac artery stenting (hybrid group) or without inflow lesions (non-hybrid group) was conducted. After propensity score matching, 120 patients were included in the non-hybrid group and 60 patients in the hybrid one. The median follow-up was 432 (193; 1313) days in the hybrid group and 472 (196; 1376) days in the non-hybrid group (p = 0.94).
Results
No significant differences were found between the groups in 30-day morbidity and serious adverse events. At 3 years, primary and secondary bypass patency for the hybrid group and non-hybrid group were 62.2% versus 59.9% (p = 0.36) and 63.7% versus 64.3% (p = 0.077), respectively. The primary patency of the iliac stents in patients of the hybrid group was 95% at 3 years. The estimated hazard ratio for primary patency for hybrid versus non-hybrid was 0.77, with 90% CI: 0.50–1.21; the noninferiority upper bound being 1.31, which corresponds to a 10% additive noninferiority margin for probabilities. The 3 years of freedom from amputation in patients with chronic limb-threatening ischemia was 94.1% and 75.0% in the hybrid and non-hybrid groups, respectively (p = 0.09).
Conclusion
The outcomes of the femoropopliteal bypass in hybrid surgery supplemented with stenting of TASC-II C, D iliac lesions was similar to femoropopliteal bypass with intact inflow arteries.
Keywords
Introduction
The patency of the inflow arteries is a key aspect of the long-term patency of the infrainguinal bypass and improvement of the limb ischemia. Therefore, bypass surgery should be combined with repair of the inflow in patients with multilevel lesions. An option to treat multilevel disease is a hybrid procedure – concurrent iliac artery stenting and femoropopliteal artery bypass.1–6
Iliac artery stenting is recommended for the first-line treatment of TASC-II A, B lesions. Whereas stenting of TASC-II C, D iliac lesions is controversial and continues to be investigated. 7 Results of hybrid operations consisting of TASC-II C, D iliac lesion stenting and femoropopliteal bypass grafting are not widely reported. It is also unclear how endovascular treatment of complex inflow lesions can affect bypass patency and outcomes.
Our aim was to evaluate the outcomes of infrainguinal bypass with concurrent stenting of TASC-II C, D iliac artery lesions and compare to those patients without inflow disease.
Materials and methods
Study design
A retrospective observational cohort study of patients with peripheral artery disease (PAD) who underwent femoropopliteal artery bypass was conducted.
Patient selection and data collection
A retrospective review of all patients admitted to Meshalkin National Medical Research Center (Russian Federation, Novosibirsk) who underwent femoropopliteal bypass between November 2011 and May 2020 was carried out. Demographic information, preoperative characteristics, perioperative outcomes, and follow-up data including all medical records and diagnostic procedures were prospectively collected in a dedicated database. This study was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice guidelines. Institutional review board approval was not required for this study due to the retrospective nature of the study.
Inclusion criteria
Inclusion criteria were: adult patients > 40 years of age; informed consent; severe intermittent claudication (Rutherford category 3) or chronic limb-threatening ischemia (CLTI), including rest pain and ischemic lesions (Rutherford categories 4 to 6); femoropopliteal TASC-II C, D lesions with ipsilateral TASC-II C, D iliac artery lesions or without inflow disease.
Exclusion criteria
Exclusion criteria were: acute limb ischemia, any form of vasculitis, or embolic or traumatic femoropopliteal occlusions; previous ipsilateral bypass surgery; patients who had previous endovascular procedures of the iliac segment, patients with associated aortic thrombosis, and patients undergoing reconstruction of an aortic aneurysm.
Patients were divided into two comparison groups depending on the nature of the atherosclerotic lesions of the lower-extremity arteries and the type of surgery performed. Patients in the first (hybrid) group had occlusive lesions of the iliac and femoropopliteal arteries. Patients in the second (non-hybrid) group were characterized by an isolated lesion of the femoropopliteal artery. Patients from the first group underwent a hybrid operation which consisted of an endovascular intervention with primary stenting of the iliac arteries and femoropopliteal bypass grafting; patients from the non-hybrid group underwent femoropopliteal bypass only.
Treatment and revascularization procedures
All patients underwent preoperative peripheral arterial evaluation with physical examination according to the European Society for Vascular Surgery (ESVS) guidelines. All patients also underwent either digital subtraction angiography or computed tomography angiography (CTA).
All surgical procedures were performed by vascular surgeons with both open and endovascular expertise.
Revascularization technique: non-hybrid surgery
The standard femoropopliteal bypass technique was used with systemic heparinization. When the common femoral artery (CFA) was stenotic or occluded, endarterectomy was performed as well. Conduit choice (great saphenous vein (GSV) or synthetic prosthesis) was autogenous vein-dependent, on a case-by-case selection. A polytetrafluoroethylene (PTFE) graft was used only in cases of inadequate (< 3 mm diameter or varicosities) or absent autogenous vein. The location of the distal anastomosis was determined by the extent of occlusion of the femoropopliteal artery.
Revascularization technique: hybrid procedure
A hybrid procedure involved iliac stenting and femoropopliteal bypass. After femoropopliteal bypass, a standard iliac stenting procedure was performed. Retrograde access was through the CFA or patch in the CFA. In case of iliac artery occlusion, either intraplaque or subintimal recanalization was obtained with the passage of a hydrophilic wire and catheter via an antegrade or retrograde approach. The choice of the type of stent was operator-dependent, on a case-by-case selection. Self-expanding nitinol stents were used mainly in cases of lesions of the external iliac artery (EIA), as well as calcified lesions or long lesions involving both common iliac artery (CIA) and EIA. Balloon-expandable stents were used predominantly in cases of CIA orificial lesions at their origin. In all the cases, bare-metal stents (BMSs) were preferred. When the disease extended into the CFA determining a stenosis > 50%, open endarterectomy and patch angioplasty with xenopericardium was performed before iliac stenting.
Postoperative follow-up
Postoperatively, patients received 100 mg acetylsalicylic acid daily and prophylactic dosages of low-molecular-weight heparins for 3 days. Patients undergoing stenting of the iliac artery received clopidogrel, at 75 mg daily, for at least 3 months.
Duplex examination was performed before discharge. The follow-up evaluation of patency of the treated limb included assessment of symptoms, physical examination, and regular color-flow Doppler ultrasonography or CTA at 3, 6, and 12 months, and then yearly. Patients with worsening of clinical symptoms or abnormal physical and instrumental examinations were further assessed and a decision on the type of reintervention was made by the vascular surgeon.
Definitions and endpoints
Primary patency was defined as absence of occlusion or flow-limiting stenosis (peak systolic velocity ratio > 2.5 by duplex ultrasonography, or a reduced vessel diameter of at least 50% by digital subtraction angiography or CTA) of the treated segment including 1 cm proximal and distal of the anastomosis. Secondary patency was defined as absence of occlusion or flow-limiting stenosis after at least one reintervention to restore patency together with all cases of primary patency. Both primary and secondary patency as well as limb salvage were defined in accordance with the ESVS guidelines. 8 Reintervention was defined as revascularization due to clinical deterioration or the presence of a flow-limiting stenosis or occlusion in the treated segment of the artery. Clinical improvement was defined as change in Rutherford category compared with baseline. Freedom from amputation was defined as preservation of a functional foot without the need of major amputation. Early outcomes were defined as perioperative morbidity (complications) and mortality within 30 days following the revascularization procedures.
The primary endpoint of the study was to compare the primary patency between groups. The secondary endpoints were: secondary patency, 30-day postoperative complications, long-term amputation in a patient with CLTI, and survival.
Statistical analysis
Propensity score matching
Propensity score matching (PSM) was used to reduce bias due to confounding variables in comparing the non-hybrid group and the hybrid one. One-to-three matching was performed by greedy nearest neighbor matching without replacement followed by optimal rematching. 9 A patient from the hybrid group could be matched to no more than three patients from the non-hybrid group. When two or three non-hybrid patients were matched to one hybrid patient, the non-hybrid patients were assigned weights 1/2 or 1/3, respectively. The other patients were assigned weight 1. The propensity score was estimated as the predicted probability of a patient being in the hybrid group from the logistic regression model based on the following 21 covariates: age, sex, atherosclerotic lesion of the runoff, Rutherford categories (as three dummy variables for categories 3–6), smoking, coronary heart disease, hypertensive disease, chronic heart failure, renal insufficiency, dyslipidemia, diabetes mellitus, height, weight, body mass index, body surface area, occlusion of anterior tibial artery, occlusion of posterior tibial artery, occlusion of peroneal artery, significant lesion of common femoral artery, significant lesion of profunda femoral artery, patency of the third portion of the popliteal artery. The matching was exact for the Rutherford category. The caliper width 0.1 was applied to the score for the matching. Absolute standardized differences (ASD) were calculated as the ratio of absolute difference of weighted means to the pooled variance for continuous variables, and as the absolute difference of weighted proportions for binary variables. For continuous variables, variance ratios were calculated as ratios of weighted variances of the comparison groups. A variable was considered appropriately balanced between the groups when ASD was < 0.1 and, in the case of continuous variables, when the variance ratio was > 0.5 and < 2 for the variable. Cobalt R package (by N Greifer) version 4.2 was used to assess the covariates’ balance .
Testing noninferiority for primary patency
In order to test noninferiority for the primary patency of the hybrid group compared to the non-hybrid group, we calculated the 90% two-sided cluster-robust CI for the hazard ratio (HR). The CI was calculated by the univariate Cox regression with weights for the matched sample with loss of patency as the outcome. The upper limit of the CI was then compared to the noninferiority bound 1.31 corresponding to the 10% additive noninferiority margin for probabilities. The noninferiority bound was calculated by the formula: min0.10
Baseline characteristics, presentation, and assessment of outcomes at 30 days
For continuous variables, the data are presented as median (1st quartile; 3rd quartile) or as mean ± SD. For binary variables, the data are presented as unweighted count (percentage), the p-values were calculated with Fisher’s exact test for the unmatched data and by conditional logistic regression for the matched data. Significance was considered at p < 0.05.
Long-term outcomes
For continuous variables, the data are presented as median (IQR: 25%; 75%). Differences in continuous variables were tested using the Mann–Whitney U-test. Patency rates are presented as Kaplan–Meier curves. In the Kaplan–Meier graphs, the p-values for the log-rank test are shown. The corresponding probabilities are presented as percentage (95% CI). For matched data, cluster-robust CIs are shown.
To assess the association of baseline characteristics and operation-time variables, we considered the multivariable Cox regression model with primary patency as the outcome, applied to the unmatched data.
Statistical analyses were performed using R 3.6.3 software (R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline and procedural characteristics
A total of 227 patients met the inclusion criteria. It was not possible to establish contact with 33 patients and determine the outcome of the operation; therefore, 194 patients were included in the analysis: 133 patients in the non-hybrid group and 61 patients in the hybrid group. After PSM, 120 and 60 patients remained in the groups, respectively. The matching was appropriate, since absolute standardized differences were < 0.1 and variance ratios were > 0.5 and < 2 for all the variables (Figure 1). Baseline characteristics of the study population are shown in Table 1. No significant difference between the two groups was observed.
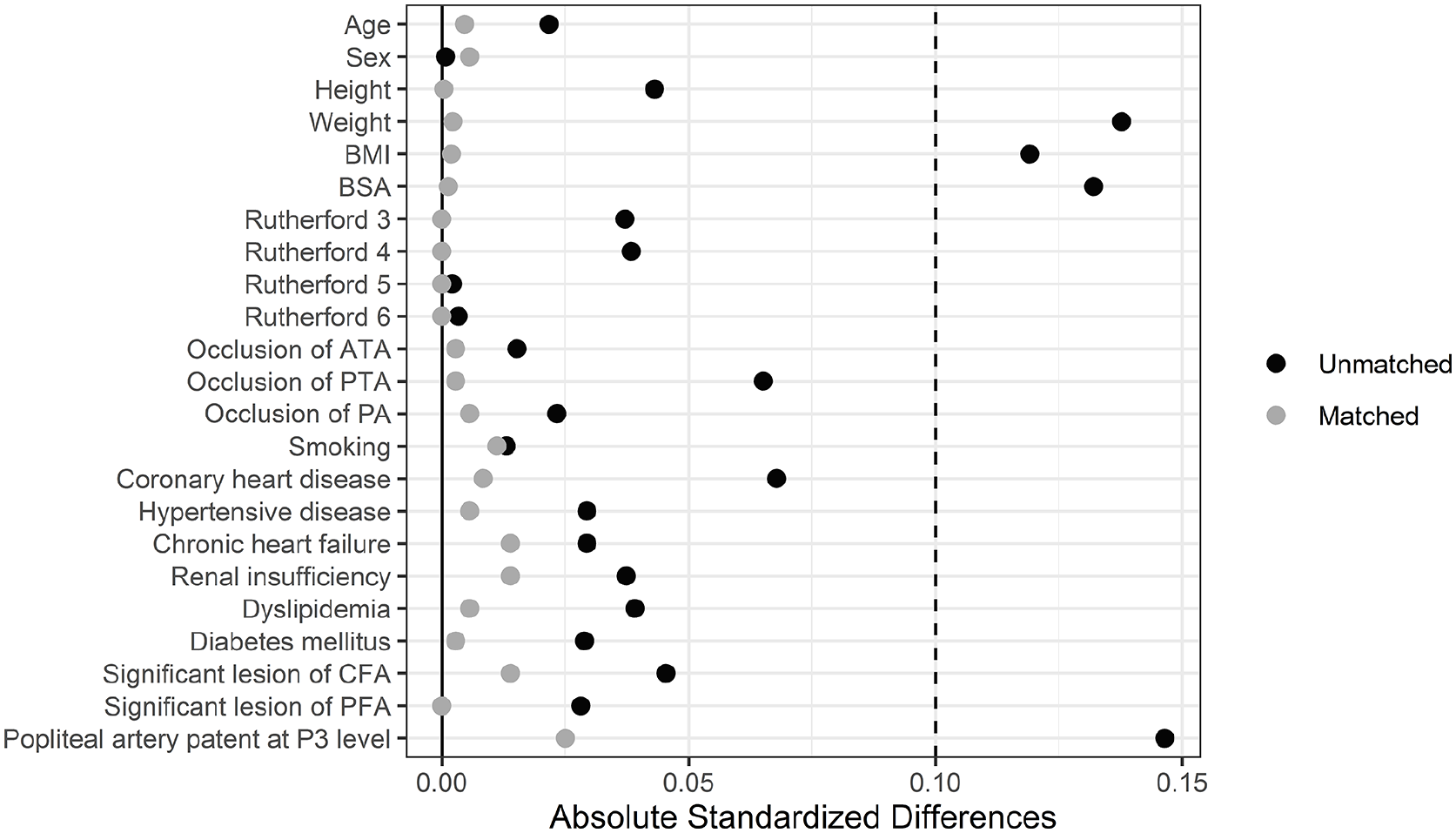
Сovariate balance before and after propensity score matching.
Baseline characteristics.
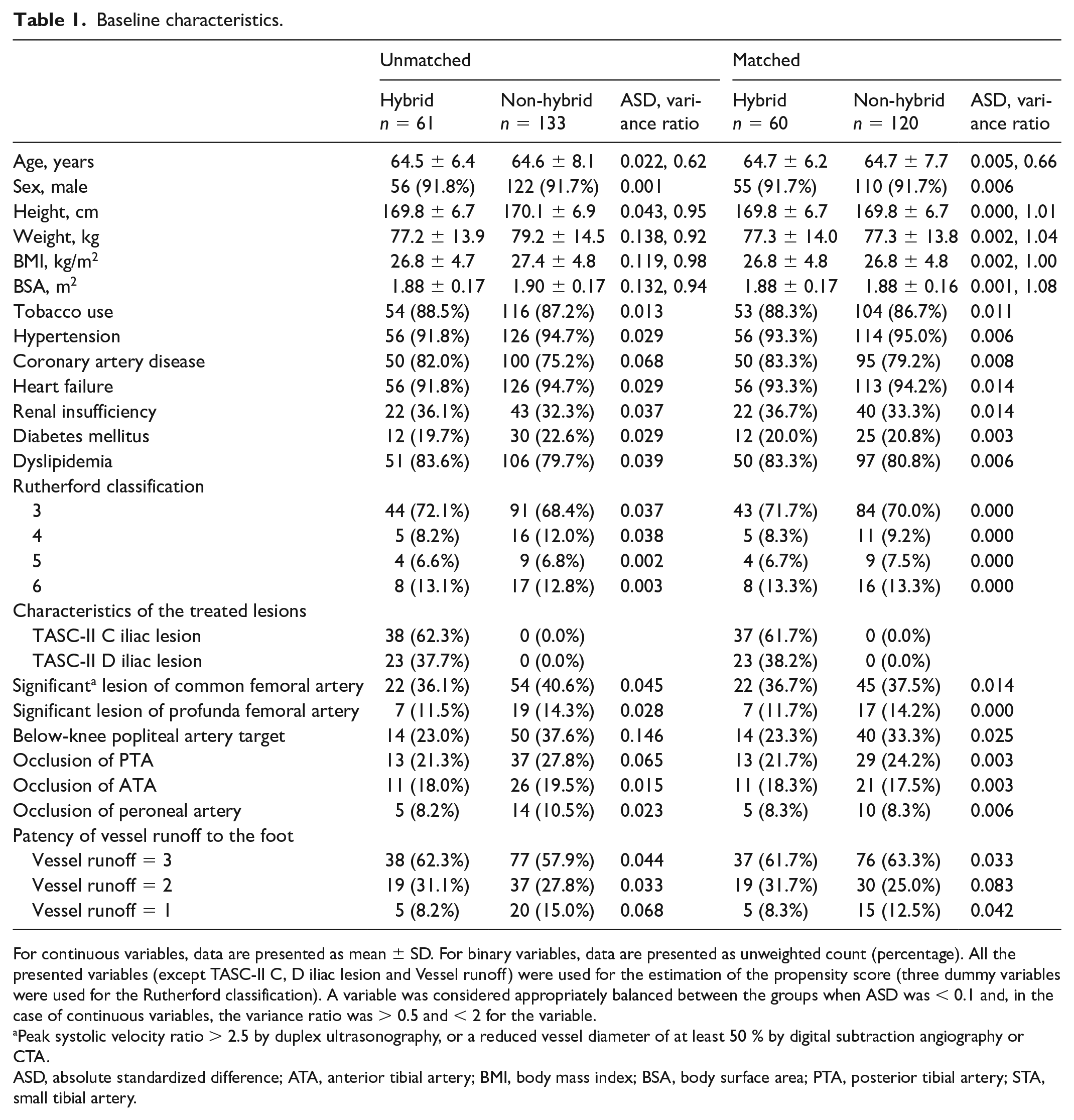
For continuous variables, data are presented as mean ± SD. For binary variables, data are presented as unweighted count (percentage). All the presented variables (except TASC-II C, D iliac lesion and Vessel runoff) were used for the estimation of the propensity score (three dummy variables were used for the Rutherford classification). A variable was considered appropriately balanced between the groups when ASD was < 0.1 and, in the case of continuous variables, the variance ratio was > 0.5 and < 2 for the variable.
Peak systolic velocity ratio > 2.5 by duplex ultrasonography, or a reduced vessel diameter of at least 50 % by digital subtraction angiography or CTA.
ASD, absolute standardized difference; ATA, anterior tibial artery; BMI, body mass index; BSA, body surface area; PTA, posterior tibial artery; STA, small tibial artery.
After the matching, in the hybrid and non-hybrid groups, a PTFE graft was used in 38 (63.3%) and 81 (67.5%) patients (p = 0.33), autogenous vein in situ in eight (13.3%) and 20 (16.7%) (p = 0.36), and reversed autogenous vein in 14 (23.3%) and 19 (15.8%) (p = 0.15), respectively. A synthetic graft was implanted below the knee joint in four (10.5%) and nine (11.1%) patients in the hybrid and non-hybrid groups (p = 0.91), respectively. The hybrid and non-hybrid groups were similar with regard to target artery for distal anastomoses (below-knee popliteal artery 23.3% vs 33.3%, p = 0.63).
Patients who underwent a hybrid operation with iliac artery stenting in 91.7% of cases received a self-expanding BMS (Absolute Pro: (Abbot Vascular, USA) 53 patients; Protégé GPS (Medtronic, Ireland): one patient; Protégé EverFlex (Medtronic, Ireland): one patient). In other cases (8.3%), balloon-expandable stents Omnilink Elite (Abbot, USA) (five patients) were implanted. The stents had an average length of 75.6 ± 25.5 mm and an average diameter of 8.7 ± 0.9 mm. In 100% of cases, the primary stenting strategy was used since the included patients had TASC-II or D iliac artery lesions.
Early outcomes
There was no significant difference in the length of stay for patients in both groups (median 11 (9; 14) days for each of the groups; p = 0.80). The complications in the early postoperative period (30 days) are presented in Table 2. There were no significant differences between the groups. In the 30-day postoperative period, there were no major adverse cardiovascular events (death, myocardial infarction, or stroke) in either group.
Overview of morbidity until 30-day follow-up.
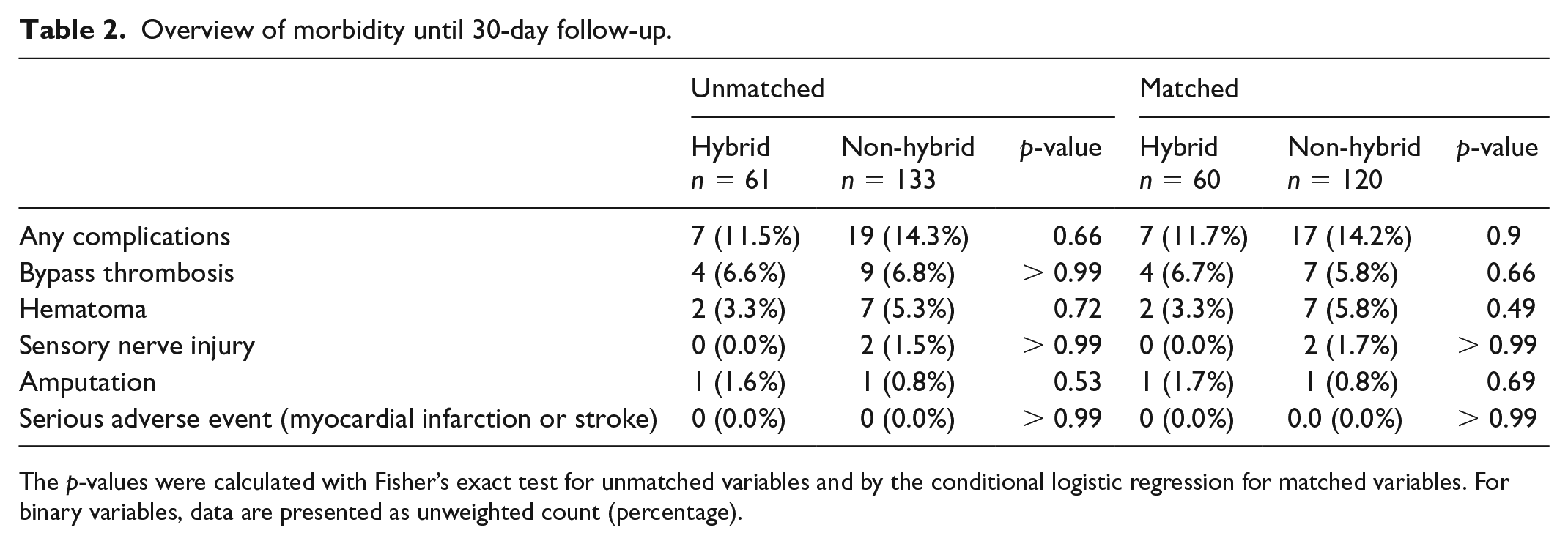
The p-values were calculated with Fisher’s exact test for unmatched variables and by the conditional logistic regression for matched variables. For binary variables, data are presented as unweighted count (percentage).
In the early postoperative period, there were four cases of acute femoropopliteal bypass thrombosis in the hybrid group and seven cases in the non-hybrid group. In the non-hybrid group, six patients had a reintervention for occlusion and two patients required reintervention due to hematoma. Also, in the non-hybrid group, a patient with CLTI underwent one amputation due to bypass thrombosis and unsatisfactory runoff vessels. In the hybrid group, four patients had a reintervention for bypass thrombosis.
The causes of femoropopliteal bypass thrombosis in the early postoperative period in the hybrid group were iliac stent thrombosis (two patients), cardiogenic thromboembolism in one patient with atrial fibrillation, and unsatisfactory runoff vessels (one patient). In the non-hybrid group, the causes of early bypass thrombosis were an underappreciated runoff vessel in three cases. It was not possible to reliably determine the cause of thrombosis in four patients with satisfactory runoff arteries without atrial fibrillation. It is possible that these cases of thrombosis can be related to coagulopathic. In all patients with satisfactory runoff arteries, patency of the femoropopliteal bypass was successfully restored after thrombectomy.
Long-term outcomes
The median follow-up in the hybrid group was 432 (193; 1313) days; in the non-hybrid group, 472 (196; 1376) days (p = 0.94).
The data for 1-, 2-, and 3-year primary and secondary patency of femoropopliteal bypass for the hybrid and non-hybrid groups are presented in Table 3. The Kaplan–Meier curves of the primary and secondary patency are shown in Figures 2 (A and B) and 3 (A and B), respectively. At 3 years, primary and secondary bypass patency for the hybrid and non-hybrid groups were 62.2% versus 59.9% (p = 0.36) and 63.7% versus 64.3% (p = 0.077), respectively.
Femoropopliteal bypass patency by Kaplan–Meier analysis.
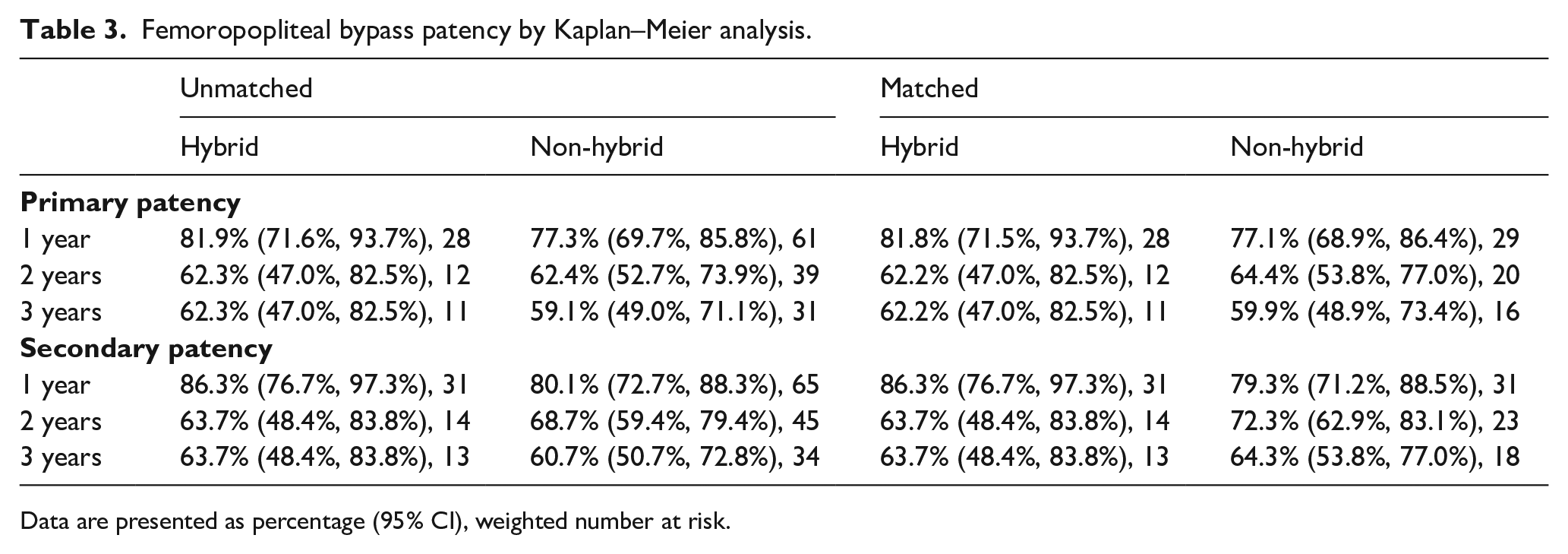
Data are presented as percentage (95% CI), weighted number at risk.
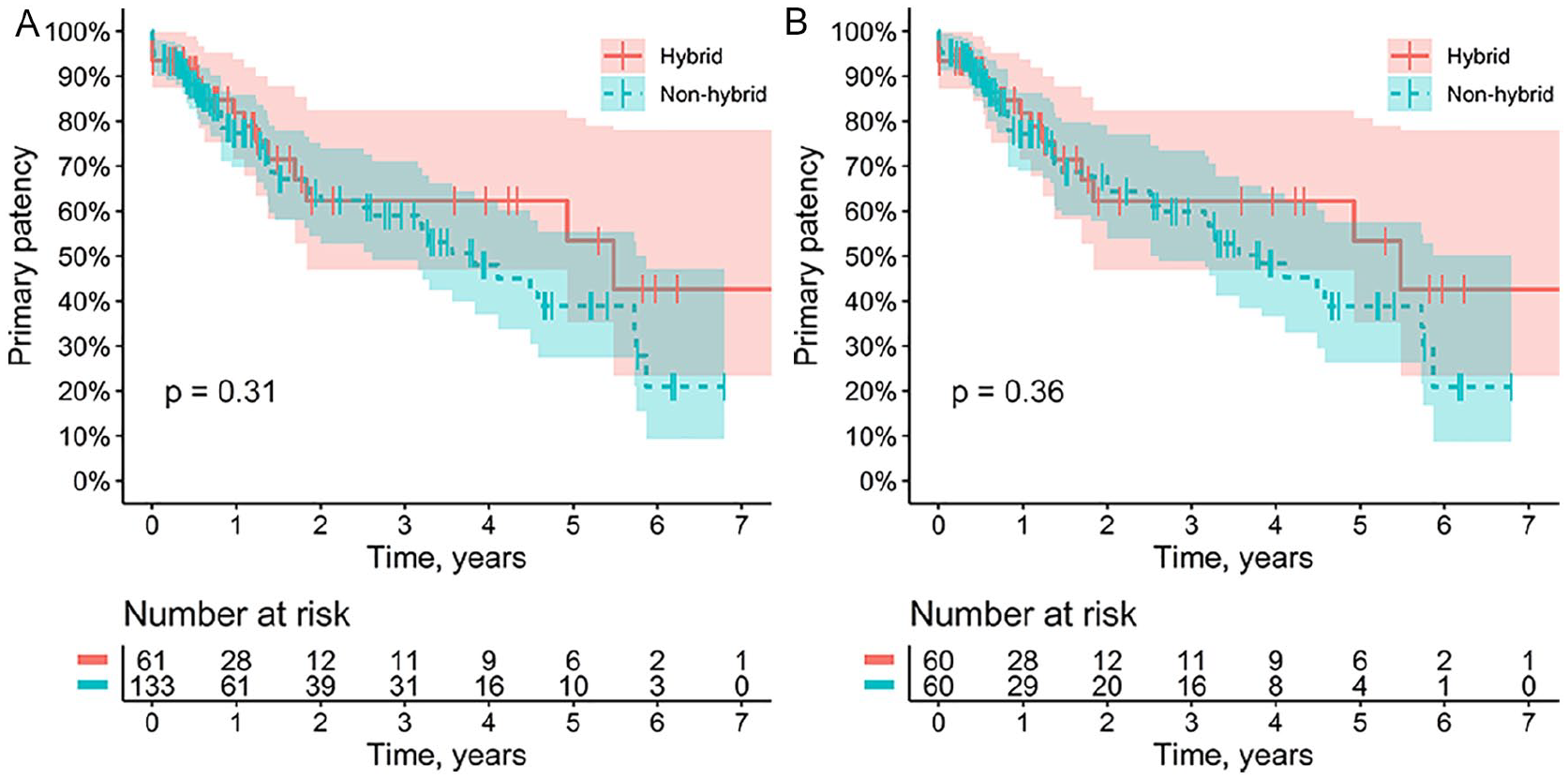
The primary patency of the femoropopliteal bypass. Kaplan–Meier curve presenting the primary patency for the hybrid (blue) and non-hybrid (red) groups according to unmatched analysis (
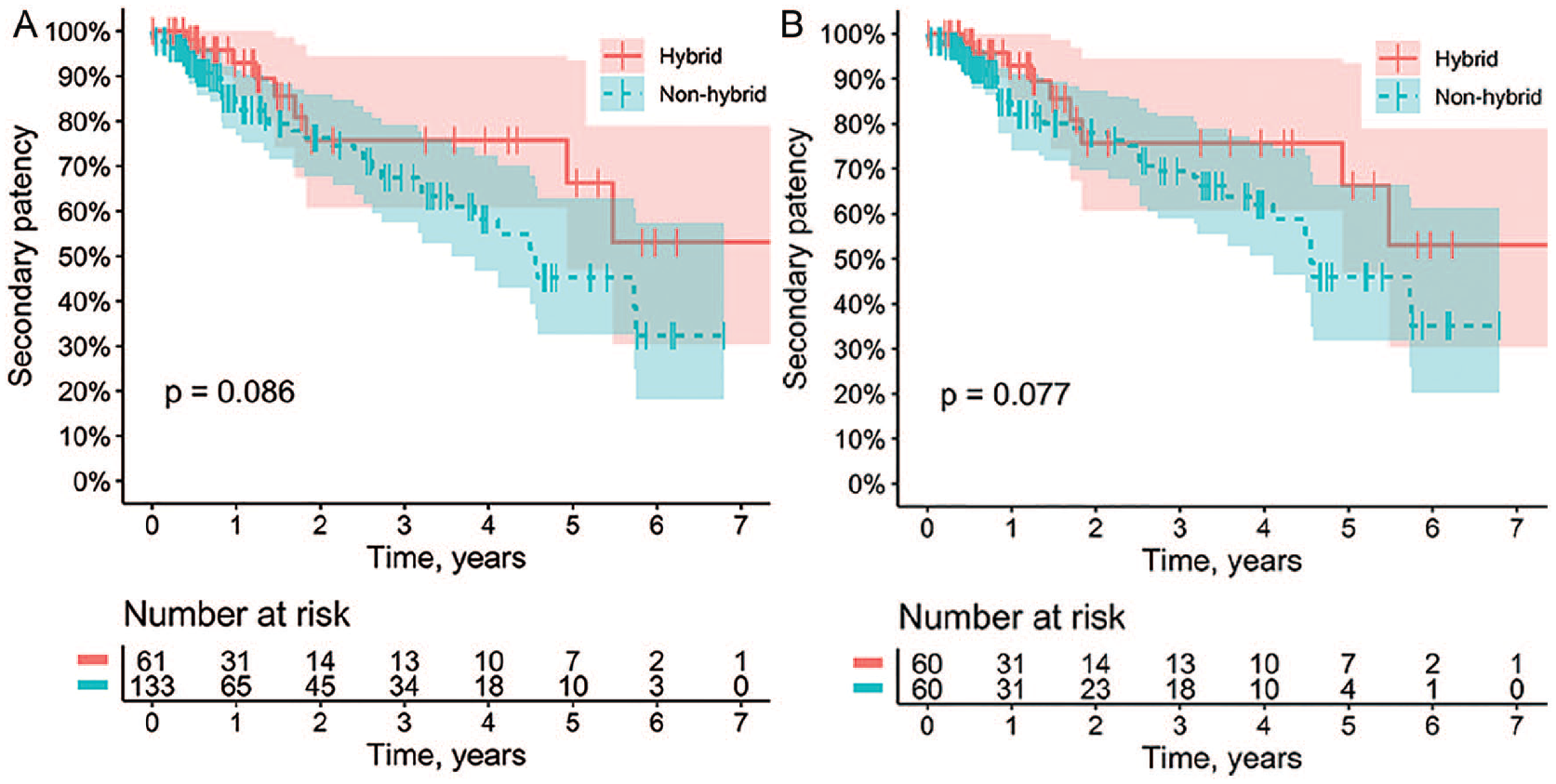
The secondary patency of the femoropopliteal bypass. Kaplan–Meier curve presenting the secondary patency for the hybrid (blue) and non-hybrid (red) groups according to unmatched analysis (
The estimated HR of cumulative primary bypass patency between the hybrid group and the non-hybrid group was 0.77; 90% CI: 0.50–1.21. As the noninferiority bound was fixed at 1.31, noninferiority (upper limit of the two-sided 90% CI < noninferiority bound) was demonstrated at the 5% significance level. Based on our research data, we can assume that the patency of the femoropopliteal bypass with stented TASC-II C, D iliac lesions is not worse than bypass with a native iliac artery. There was no statistical evidence of violation of the Cox assumptions for the model (p = 0.19 for the Grambsch–Therneau test).
The cumulative primary patency of the iliac stents in patients from the hybrid group reached 95.0%.
The multivariable Cox regression model showed that the following variables were associated with the bypass occlusion (Table 4): Rutherford category (HR 1.31 [1.0; 1.7] corresponding to the increase of the category by 1, p = 0.04), dyslipidemia (HR 0.47 [0.23; 0.95], p = 0.03), and below-knee popliteal artery target (HR 2.17 [1.10; 4.24], p = 0.02). There was no statistical evidence of violation of the Cox assumptions for the model (p = 0.057 for the Grambsch–Therneau test).
Factors associated with femoropopliteal bypass occlusion.
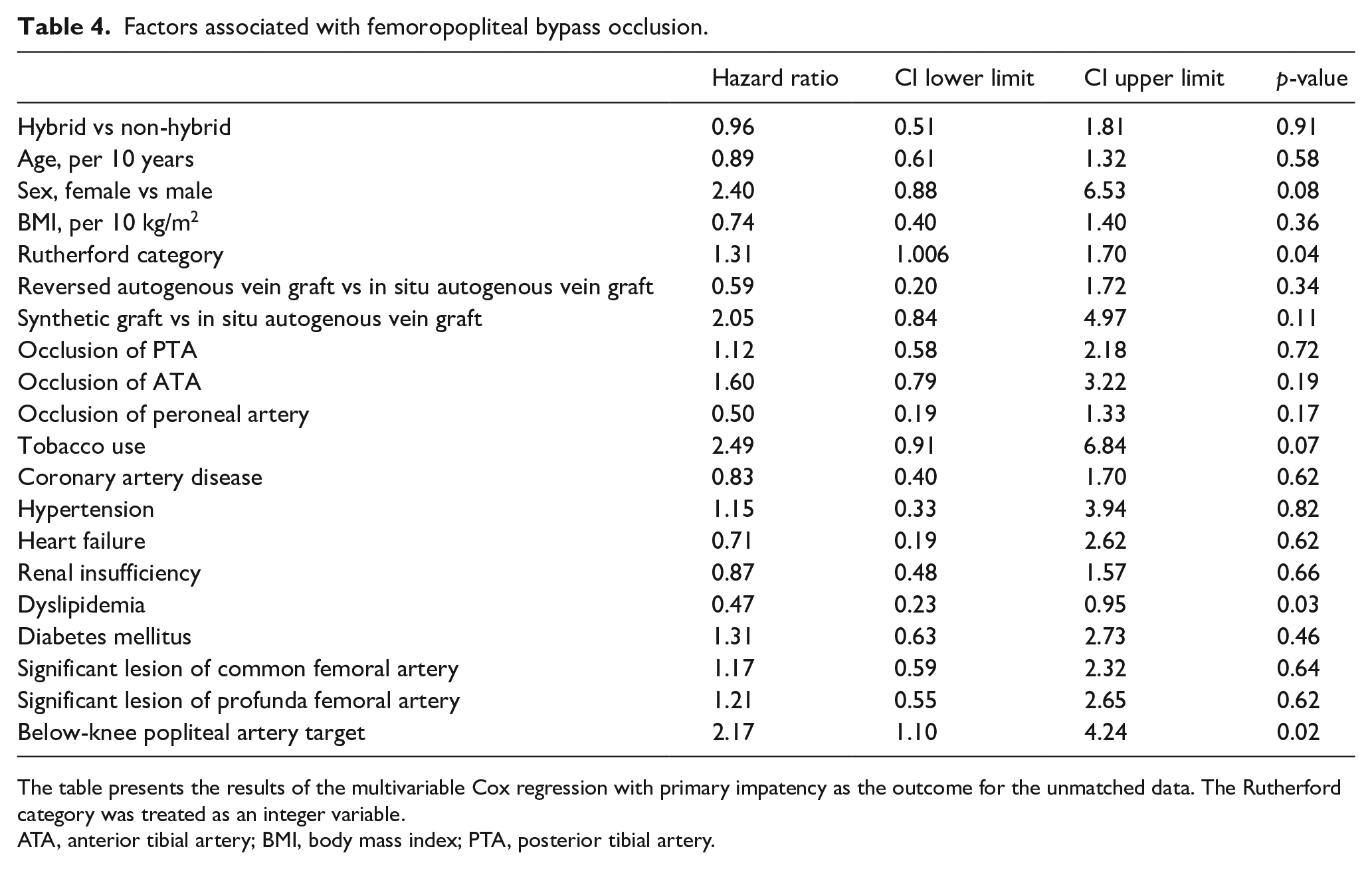
The table presents the results of the multivariable Cox regression with primary impatency as the outcome for the unmatched data. The Rutherford category was treated as an integer variable.
ATA, anterior tibial artery; BMI, body mass index; PTA, posterior tibial artery.
Both groups showed an improvement in Rutherford category compared with baseline (Figure 4). The 3 years of freedom from amputation in patients with CLTI was 94.1% and 75.0% in the hybrid and non-hybrid groups, respectively (p = 0.09). The long-term survival in the hybrid group was 98.3%, and in the non-hybrid group was 95.8% (p = 0.34).
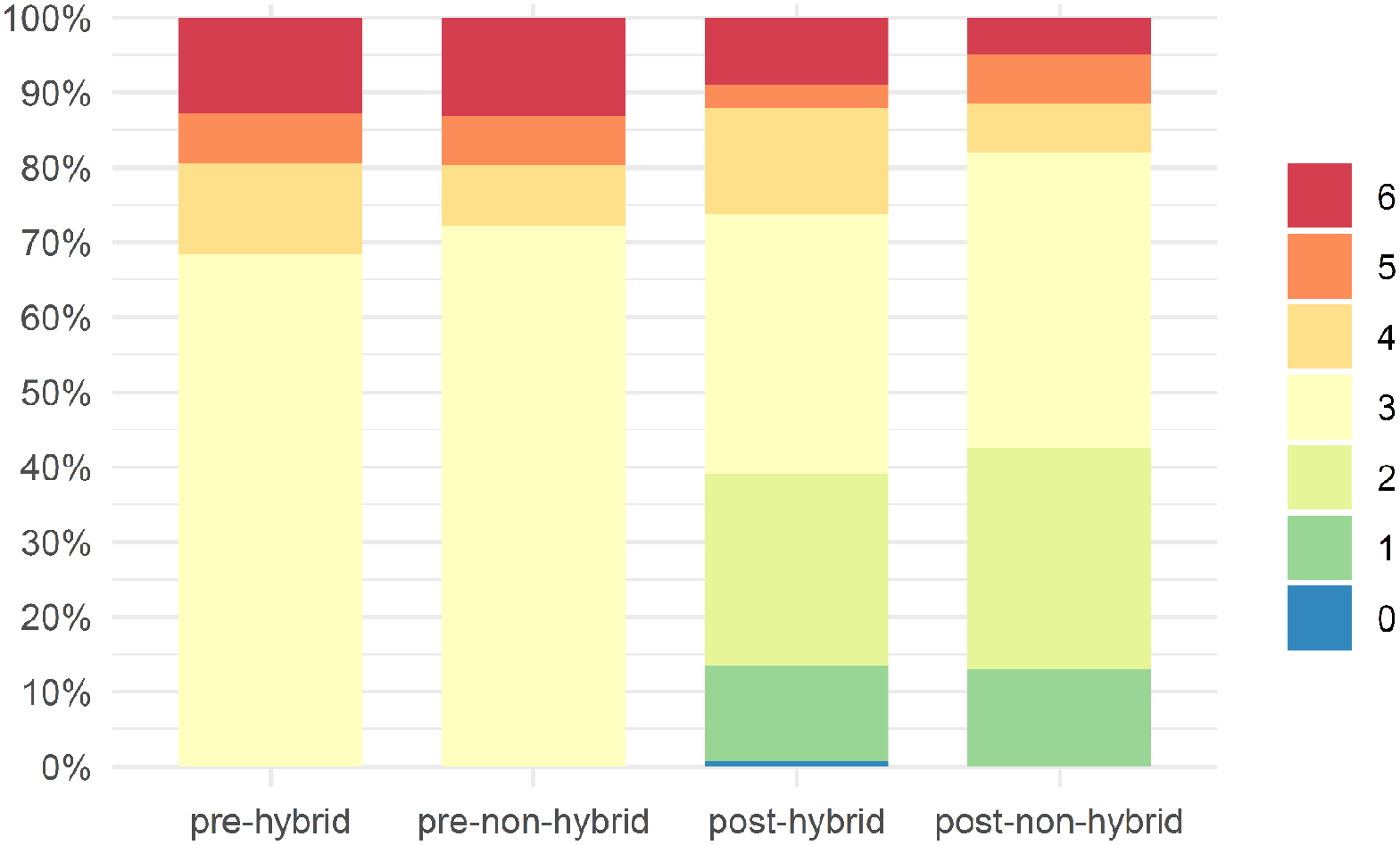
Evolution of the Rutherford category.
Discussion
This study compared the early and long-term clinical outcomes of femoropopliteal bypass in 180 patients with stented TASC-II C, D iliac lesions or native iliac artery. The femoropopliteal bypass patency was similar in both hybrid and non-hybrid groups. Freedom from major adverse limb events (MALEs) was also similar for both groups in patients with CLTI.
Eagleton et al. demonstrated the importance of the inflow patency for the patency of infrainguinal arterial reconstructions. 11 They retrospectively assessed the effect of the reconstructed inflow on the infrainguinal bypass patency in 495 patients. For inflow, patients underwent aortoiliofemoral bypass procedures, extraanatomic bypass procedures, balloon angioplasty with and without stent placement, and iliofemoral endarterectomy, of which 72% were concurrent with the infrainguinal bypass procedures. Four-year primary patency rates in vein grafts with reconstructed inflow sources were lower than those in grafts with nonreconstructed inflow (41% vs 54%; p = 0.006). Assisted primary patency rates and secondary patency rates, however, were similar (62% vs 74% and 64% vs 77%, respectively). The 4-year primary patency rate (45% vs 55%), assisted primary patency rate (60% vs 60%), and secondary patency rate (60% vs 61%) in prosthetic grafts did not vary based on inflow source. The main cause of occlusion of the femoropopliteal bypass was inflow problems. In our study, we selected to perform only endovascular interventions on the iliac inflow due to lower morbidity.1,2,12,13
The reported 24-month primary patency of hybrid procedures in iliac and femoropopliteal arteries ranges from 72.2% to 93.3%.3,14–16 When assessing the patency of the femoropopliteal bypass, the type of conduit and the level of distal anastomosis are important. Thus, the 5-year primary patency bypass above-knee popliteal artery is 63–75% for GSV17,18 and 63 ± 9% for synthetic prostheses. The 3-year primary patency bypass below-knee popliteal artery ranges from 18% to 41%. 19 The patency of synthetic conduits in our study was 70.9% and 59.5% (p = 0.33) in the hybrid and non-hybrid groups, respectively, whereas the patency of GSV was 78.9% and 66.6% (p = 0.64) in the hybrid and non-hybrid groups, respectively. In two out of three cases, a prosthetic graft was used due to a lack of autogenous conduit, as was below-knee popliteal artery bypass in two out of three cases. The risk factors for femoropopliteal conduit thrombosis in the long-term period, according to our data, were Rutherford category and below-knee popliteal artery target. Dyslipidemia reduced the risk of bypass thrombosis. Potentially due to these, patients received lipid-lowering therapy.
However, femoropopliteal bypass patency in hybrid cases was dependent on the patency of the iliac stent. The ‘gold standard’ for treatment of TASC-II C, D iliac lesions is open surgery; however, many authors have shown good results from iliac stenting.20–22 De Donato et al. showed, in a large, prospective, multicenter (BRAVISSIMO) analysis that endovascular therapy may be considered the preferred first-line treatment option of iliac lesions, regardless of TASC-II lesion category. 20 The 24-month primary patency was 91.9% for TASC-II C, and 84.8% for TASC-II D. Based on the complexity of the iliac artery lesion, Dosluoglu et al. classified hybrid operations into simple (group simple sHYBRID – iliac artery lesion corresponds to TASC A/B) and complex (group complex cHYBRID – iliac artery lesion corresponds to TASC-II C, D), with a technical success rate of 96% and 100%, respectively. 12 However, with an average follow-up of 30.3 months, 12- and 36-month primary patency rates in patients who underwent interventions at the aortoiliac segment level in the sHYBRID group were 80% and 75%, respectively, and were similar to those in the cHYBRID group, which were 87% and 81%, respectively (p = 0.863). The frequency of reinterventions was also not statistically significantly different between the groups. 12 The iliac artery reinterventions did not affect long-term patency or limb recovery. Piazza et al. retrospectively assessed the patency of hybrid procedures in 75 patients with femoropopliteal bypass and stented TASC-II C, D iliac lesions. 13 The 42-month primary patency of the iliofemoral segment was 65.2% (95% CI: 53–86%). This finding was primarily related to femoropopliteal bypass occlusion (primary patency, 69.5%), rather than iliac stent loss of patency (primary patency, 94.6%). These results are most consistent with our data: in the hybrid group, the 3-year primary patency of the femoropopliteal conduit was 62.2%, аnd the cumulative primary patency of the iliac stents reached 95.0%.
Study limitations
Our analysis has some limitations. This was a retrospective observational study with a small sample size and the choice of technical aspects of the operation was left to the attending surgeon; besides, patients differed in the period of follow-up after surgery. Also, 15% of the patients were lost to follow-up, which may be a potential source of bias and potentially distort the results, especially those regarding long-term survival – which was observed to be higher than expected in patients with peripheral artery disease. The overwhelming majority were male, which may limit generalizability, given that female sex may affect patency rates of iliac stenting. However, prospectively collected data on the results of surgery allowed us to obtain reliable information about the patency of the operated segment and the patient’s clinical condition. The use of the PSM method at the stage of statistical data processing provided comparability of the two groups for further comparison. But there may be residual bias with PSM and potential issues with noninferiority testing. Randomized trials are needed to draw definitive conclusions.
Conclusion
Long-term femoropopliteal bypass patency in patients with stented TASC-II C, D iliac lesions were similar to those with normal inflow. Thus, stented complex lesions of the iliac arteries may provide comparable patency of the femoropopliteal bypass in multilevel lesions as does the native iliac artery in isolated femoropopliteal lesions. A hybrid procedure can be considered the optimal choice for a patient with multilevel lesions and complex iliac lesions.
Footnotes
Acknowledgements
The investigators thank Alik Farber and Jeffrey Siracuse (Boston University School of Medicine, Boston, MA, USA) for the discussion which has substantially improved this paper.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The work of Pavel Ruzankin and Evgeny Prokopenko was supported by the Mathematical Center in Akademgorodok under agreement No. 075-15-2019-1675 with the Ministry of Science and Higher Education of the Russian Federation.