
Abstract

Cardiovascular diseases (CVD), including peripheral vascular disease, is a leading cause of morbidity and mortality in the United States. Sedentary behavior, an important risk factor for CVD, 1 is becoming increasingly prevalent due to changes in the workplace environment that include increased automation leading to less physically demanding jobs, greater utilization of desktop computers for work, and the rapid development of a ‘work from home’ culture, most acutely driven by the coronavirus disease 2019 (COVID-19) pandemic. 2 The continued shift toward more sedentary behavior in the workplace could translate into increasingly greater risks for CVD among the working public over the next decade. To address this issue, several employer-based programs have been developed and tested to reduce sedentary behavior during work hours. These have included lifestyle counseling sessions, motivational interviewing, wrist-worn physical activity trackers, and altering the workstation to encourage less sedentary time. 3 However, implementation of these programs has shown varying results and generalizability across the global workforce is limited by cost, time constraints, and institutional resources. 3 Thus, alternative options are needed to reduce sedentary behavior during the working day.
In this issue of Vascular Medicine, Bodker and colleagues 4 assess the impact of providing adjustable sit-stand desks to employees in the workplace on sedentary time, metabolic biomarkers, and vascular function measured by flow-mediated dilation (FMD) of the brachial and superficial femoral arteries. In this nonblinded, nonrandomized, self-control crossover design, 15 sedentary office employees who were overweight or obese underwent baseline assessments with an accelerometer, anthropometric and metabolic measurements, and FMD testing. They were then provided with a low-cost, nonelectric, height-adjustable sit-stand desk at their office space and trained on its use but were not provided any prompting after the initial installation and training. Repeat endpoint testing was performed at 12 and 24 weeks. The majority of the cohort were middle-aged females with ~6.5 hours of sedentary work-time at baseline. The postintervention mean daily sedentary time at work decreased by approximately 90 minutes at 12 and 24 weeks compared with baseline and correlated with an increase in standing time at work. Superficial femoral artery FMD increased from 4.9 ± 1.7% to 6.4 ± 2.3% (p = 0.043) at 12 weeks and further to 8.1 ± 3.2% (p = 0.009) at 24 weeks, but brachial artery FMD did not change. Significant reductions in fasting insulin and triglyceride levels were also seen. Interestingly, the sit-stand option at work did not translate to less sedentary time outside of work hours nor did the intervention increase total daily or moderate/vigorous daily step counts during the intervention period.
Although this study has important limitations, including its modest sample size, nonrandomized design, and use of surrogate endpoints for CVD risk, there are several important lessons to be learned that can be applied to future studies of hard endpoints with a larger sample size to provide more generalizable, definitive results. 4 First, this study clearly demonstrated a decrease in sedentary time with the introduction of sit-stand desks in the workplace. Although employees were not specifically directed to stand at various points during the day, the simple option to stand at one’s leisure translated into a meaningful decrease in sedentary time with salutary physiological changes. Furthermore, use of a sit-stand desk, compared with a stand-only desk, may reduce low back pain and fatigue at work. 5 These secondary advantages may increase productivity and employee satisfaction at work. This intervention could also easily be implemented in the home (e.g. during the COVID-19 pandemic when there is a need to work remotely); 6 however, whether its use would decrease sedentary time at home by a similar magnitude while at work remains to be determined and requires further study.
Second, the study intervention yielded vascular and metabolic improvements with decreasing sedentary time alone but without any meaningful changes in weight or overall step counts. This finding certainly lends credence to the evidence that increasing physical activity alone, even if just from sedentary to modestly nonsedentary, and without changes in weight, can have important benefits. Indeed, studies have shown that the most cardiovascular benefit is accrued going from completely sedentary/no physical activity to relatively minimal physical activity, with diminishing improvements seen as the amount of physical activity increases. 7 The sit-stand desk may be one strategy to accomplish this in the workplace setting.
Third, the finding that superficial femoral, but not brachial FMD, improved is understandable given the standing-specific intervention. What this means for long-term vascular health, however, is unclear. Studies investigating the effects of brachial FMD on CVD risk have yielded mixed results. A prospective study with 2264 postmenopausal women showed that a low brachial FMD of less than 4.5% accounted for 56.6% of major cardiovascular events, suggesting that it may have prognostic value. 8 There are no studies thus far that investigate the effects of femoral FMD on the risk of CVD. The current study suggests a need to further investigate femoral FMD as a cardiovascular risk factor and whether improving lower limb FMD can have lasting benefits for peripheral vascular health.
The COVID-19 pandemic has completely changed the employment landscape. A greater number of people are working remotely from home now more than ever. Although this may allow opportunities for increased break time with more physical activity and greater flexibility for exercise, the social isolation and lack of need to interact with others or go anywhere to do so could instead lead to a worsening of sedentary behavior. Reducing occupational sedentary behavior may be more important now than ever. A recent study demonstrated interest and acceptability in using standing desks in the home environment. 9 From an employer standpoint, sit-stand desks may increase employee productivity. 10 This, combined with the potential health benefits of reducing sedentary behaviors, should more than offset the initial expenses of purchasing the desk. Furthermore, an expert statement recommended that predominantly desk-based workers should progress towards accumulating at least 2 hours/day of standing and/or light walking during work hours and highly recommended sit-stand adjustable stations to accomplish this goal. 11
The study by Bodker and colleagues moves the field of physical activity and vascular/metabolic health forward toward practical, simple solutions that are easy to implement yet may have lasting benefits. However, this study is only the beginning. Female subjects enrolled were of relatively low metabolic risk (mean visceral fat < 10%; waist-to-hip ratio < 1; triglycerides < 150 mg/dL), so it would be important for future studies to include participants with a higher cardiovascular risk profile to see if results are even more robust. Additional vascular and metabolic endpoints can be added to further define the impact of sit-stand desks. This study will also help to improve the design of future workplace-based research. Bodker and colleagues should be congratulated on a well-designed and insightful study. The study’s preliminary findings provide further support that it’s time to take a ‘stand’ against CVD by decreasing sedentary time in the workplace to improve vascular and metabolic health (Figure 1).
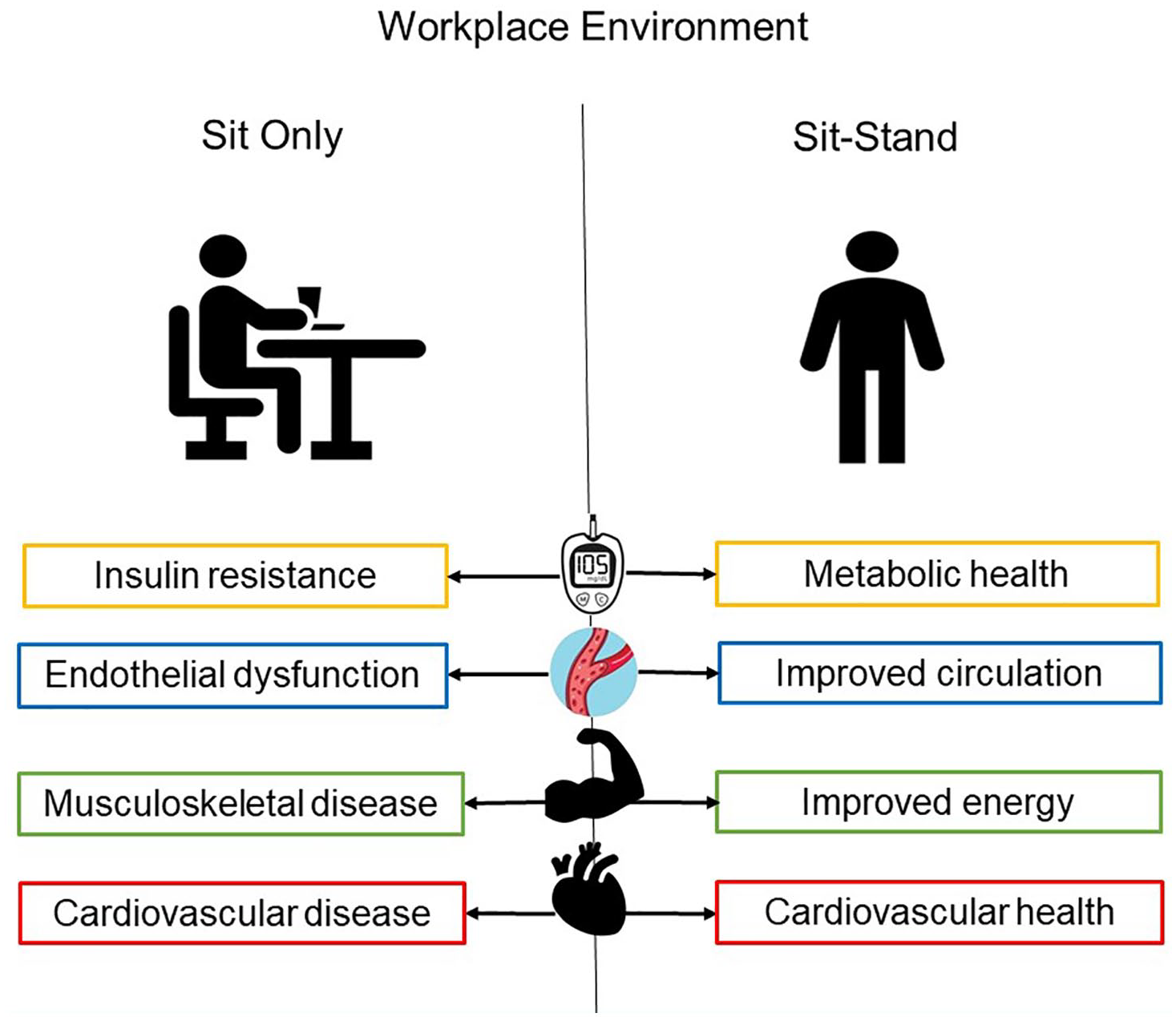
Potential effects of sitting versus alternating sitting and standing in the workplace. The sit–stand method has been shown to have multiple benefits: (1) improve fasting blood glucose levels, (2) increase blood supply to the femoral arteries, (3) decrease fatigue and low back pain, and (4) improve cardiovascular risk factors.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.