
Abstract
Firefighting is associated with an increased risk for a cardiovascular (CV) event, likely due to increased CV strain. The increase in CV strain during firefighting can be attributed to the interaction of several factors such as the strenuous physical demand, sympathetic nervous system activation, increased thermal burden, and the environmental exposure to smoke pollutants. Characterizing the impact of varying thermal burden and pollutant exposure on hemodynamics may help understand the CV burden experienced during firefighting. The purpose of this study was to examine the hemodynamic response of firefighters to training environments created by pallets and straw; oriented strand board (OSB); or simulated fire/smoke (fog). Twenty-three firefighters had brachial blood pressure measured and central blood pressure and hemodynamics estimated from the pressure waveform at baseline, and immediately and 30 minutes after each scenario. The training environment did not influence the hemodynamic response over time (interaction, p > 0.05); however, OSB scenarios resulted in higher pulse wave velocity and blood pressure (environment, p < 0.05). In conclusion, conducting OSB training scenarios appears to create the largest arterial burden in firefighters compared to other scenarios in this study. Environmental thermal burden in combination with the strenuous exercise, and psychological and environmental stress placed on firefighters should be considered when designing fire training scenarios and evaluating CV risk.
Keywords
Introduction
Firefighting is associated with an increased risk for cardiovascular (CV) events, which account for approximately 45% of line of duty deaths reported by the National Fire Protection Association (NFPA). 1 The increased CV risk during firefighting is likely related to increased CV strain from the interaction of several factors such as the strenuous physical demand, sympathetic nervous system activation, increased thermal burden, and the environmental exposure to smoke pollutants. 2 Currently, there is little research examining different combinations of these factors to determine the impact on the CV system.
Environmental conditions can be intentionally manipulated for objective-based training purposes that result in varying thermal burden and exposure to smoke pollutants, which in combination, alter sympathetic nervous system activation. 2 Firefighters are exposed to a large thermal burden both through the use of full personal protective equipment and working in environments with elevated temperatures and radiant exposures. Firefighters traditionally conduct training utilizing controlled burns fueled by wood and light combustible material for ignition (e.g. pallets and straw). Thermal burden and environmental smoke production can be increased by adding engineered wood products like oriented strand board (OSB) to the light combustible material. To decrease environmental thermal burden and pollutant exposure, fire and smoke can be simulated by utilizing theatrical fog and a visual display of fire glow.
Firefighters are faced with a variety of conditions in the real-world dependent on the type of fire they are summoned to attack. Elucidating the CV response to different training scenarios (pallet, OSB, fog) where environmental controls are in place, may provide insight into CV burden experienced during real-world firefighting. Despite substantial previous literature on the physiological response to live-firefighting,3–7 little research has been conducted in relation to the physiological responses to different environments. 8 This study examined the hemodynamic response of firefighters to different environments: OSB, pallet and straw, and simulated smoke/fog to generate obscured conditions. We hypothesized CV burden would be lowest in the thermoneutral fog environment compared to the live-fire pallet and OSB environments, and the OSB environment would generate the largest CV burden of all the training environments.
Methods
Ethical approval
This study was approved by the institutional review boards at the University of Illinois at Urbana-Champaign (#16497) and the National Institute for Occupational Safety and Health (16-DSHEFS-01) and was performed in accordance with the ethical standards of the Declaration of Helsinki. All participants provided written informed consent prior to participation.
Participants
Healthy volunteer and career firefighters aged 18–55 years from departments in Georgia, Illinois, Indiana, Massachusetts, New York, South Dakota, Texas, Virginia, and Wisconsin who had completed a medical evaluation consistent with the NFPA 1582 Standard within the previous 12 months were recruited via nationwide multimedia efforts to participate in the study. Menstrual cycle was not controlled for in female participants due to the nature of the study design. Exclusion criteria included known cardiovascular disease or gastrointestinal complications, current tobacco use, and pregnancy.
Study design
The study took place at the Illinois Fire Service Institute (IFSI) campus in Champaign, Illinois. This is a secondary analysis on the CV response in firefighters, thus the study design has been previously described in detail. 8 In brief, participants reported for testing following a standard meal ingested within 60 minutes of each trial. Each firefighter completed identical training activities in three different training fire environments (further described below) commonly used to simulate fire training in residential structures. These training environments utilized the burning of: (1) pallet and straw; (2) OSB with pallet and straw; or generation of (3) fog/simulated smoke to create conditions of visual obscuration without increased ambient thermal burden and pollutant exposure. Training trials were completed with 48 h of recovery in between. All participants wore full personal protective equipment and self-contained breathing apparatus prior to entering any of the training structures.
Firefighters conducted a common ‘coordinated attack’ training scenario in groups of four firefighting trainees in which the firefighters must suppress all active fire and rescue two simulated victims (75 kg manikins). Within a given test day, groups of firefighters would engage in one bout of testing at approximately 09:00, 12:00 or 15:00 (i.e. three groups of four firefighters were studied on each day). This sequence was repeated for each scenario (pallet, OSB, fog). Firefighting trainees reported at approximately the same time of day for each of their three scenarios to control for diurnal variation. The order in which the training environments were introduced was staggered in an attempt to partially balance the order within the constraints of the overall study design. One group of firefighters completed the scenarios in the order of fog, pallet, OSB, while another group of firefighters completed scenarios in the order of OSB, pallet, fog.
Firefighters performed suppression of two rooms of fire in three different training fire environments, defined below (schematics of structural layouts previously reported 8 ):
Pallet – In a concrete and steel training structure laid out similar to a mid-20th century single family dwelling, the fire was ignited using three pine wooden pallets and one bale of straw in two separate bedrooms.
OSB – In a T-shaped metal shipping container-based prop, fires were ignited in burners using two pallets and one bale of straw along with a sheet and a half of OSB along the ceiling of two separate bedrooms.
Fog – In a building constructed from metal shipping containers to have an identical layout to the pallet scenario, two theatrical smoke machines were utilized in conjunction with a commercially available fire simulation panel that provides digital flames and sound effects, which reacts to the application of water through thermal sensors (Attack Digital Fire System; Bullex, Albany, NY, USA).
Measures
Participants’ height (cm) and weight (kg) were measured via a standard stadiometer and digital scale, respectively. Participants were seated in a chair for a 10-minute rest period where multiple measurements were collected prior to the initiation of the fire training. 8
Brachial blood pressure was measured at baseline, immediately after returning from the training environment, and 30 minutes post-training (Mobil-O-Graph 24 PWA System; IEM, Stolberg, Germany). The appropriately sized cuff based on the circumference of the upper arm was placed on the left arm with participants seated with their feet flat on the floor and back supported with no talking. Baseline measures were completed in duplicate and averaged. Outcomes obtained were brachial systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP), pulse pressure (PP), and heart rate (HR).
Brachial pulse waves were automatically collected by the Mobil-O-Graph following the brachial blood pressure measurement by inflation of the cuff to diastolic pressure and holding this inflation pressure for approximately 10 seconds. A central blood pressure waveform was estimated via a transfer function using the built-in ARCSolver method (Austrian Institute of Technology, Vienna, Austria) from the brachial pulse waves to estimate central SBP and central PP, 9 cardiac output (CO), stroke volume (SV), and total vascular resistance (TVR).10,11 Wave separation analysis was performed to obtain augmentation index normalized to HR. 12 By combining parameters from the pulse wave and wave separation analyses, a mathematical model was used to estimate pulse wave velocity (PWV).13,14 PWV was also divided by MAP to control for the influence of pressure. Rate pressure product (RPP) was determined by multiplying HR by central SBP as a measure of myocardial work.
During each live-fire scenario, core body temperature and HR were continuously monitored. For core body temperature, participants swallowed a small core temperature sensor capsule (VitalSense Core Temperature Capsule; Phillips Respironics, Murrysville, PA, USA) 6–12 hours prior to activity. For HR, participants wore a base layer shirt (Globe Manufacturing, Pittsfield NH, USA) with an integrated HR monitoring system (BioHarness 3, Zephyr Technologies, Annapolis, MD, USA). Baseline and peak core temperature and HR were recorded for this analysis.
Statistical analysis
All data are reported as mean ± SD. Normality was assessed with the Shapiro–Wilk test. The main effects of time (baseline, immediate post-firefighting, and 30 minutes post-firefighting) and training environment (pallet, OSB, fog) and their interactions on all CV outcomes were assessed with a 3 × 3 repeated measures analysis of variance (ANOVA). When significant effects were observed, post-hoc analyses with the Bonferroni adjustment were conducted. Data analyses were performed in IBM SPSS version 24 (IBM Corp., Armonk, NY, USA) with an a priori α-level of 0.05 deemed significant. As a secondary analysis, no a priori power calculation was undertaken.
Results
Twenty-four firefighters participated in this study. Owing to field data collection challenges at a single time point for one firefighter, the final analyses included 23 firefighters (21 males, 2 females) with complete hemodynamic data. Firefighters were, on average, aged 40 ± 9 years and overweight, with a BMI of 28.7 ± 5.1 kg/m2 (height, 178.5 ± 6.3 cm; weight, 91.8 ± 18.1 kg). During the training scenarios, both core temperature and HR increased (time p < 0.01) and were different between training environments (environment, p < 0.05, Table 1).
Peak core temperature and heart rate.
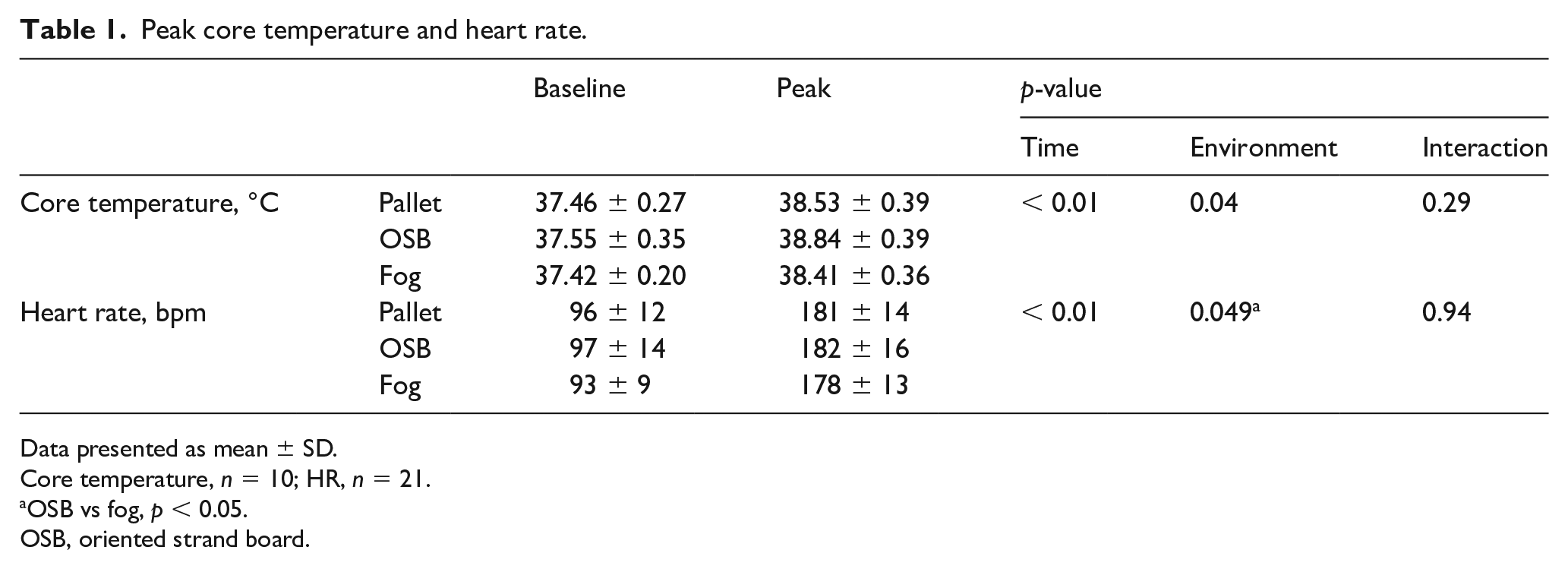
Data presented as mean ± SD.
Core temperature, n = 10; HR, n = 21.
OSB vs fog, p < 0.05.
OSB, oriented strand board.
Table 2 provides a summary of the hemodynamic responses of firefighters to the different training environments. Firefighting activity in the different training environments led to similar changes in all outcome variables over time (p for interactions > 0.05). A main environment effect was observed in which the OSB training fire environment resulted in greater SBP, MAP, PP, and PWV (Figure 1) for firefighters in comparison to the fog training environment (p < 0.05). When PWV was controlled for changes in MAP, the environment effect was no longer significant (p = 0.15). There were several main time effects, indicating that firefighting activity altered all hemodynamic variables except total vascular resistance (p > 0.05). Peripheral and central systolic and pulse pressure increased immediately following fire-training and returned to, or decreased below baseline values at 30 minutes. The increase in systolic pressure in combination with the increase and partial recovery of HR at the immediate and 30-minute assessment led to an increase and partial recovery of RPP immediately and 30 minutes post-training, respectively. PWV was elevated immediately post-fire training, even after controlling for MAP. Similarly, augmentation index was elevated immediately following fire training and partially recovered toward baseline values at 30 minutes.
Firefighter hemodynamic response to firefighter training in different training environments (n = 23).
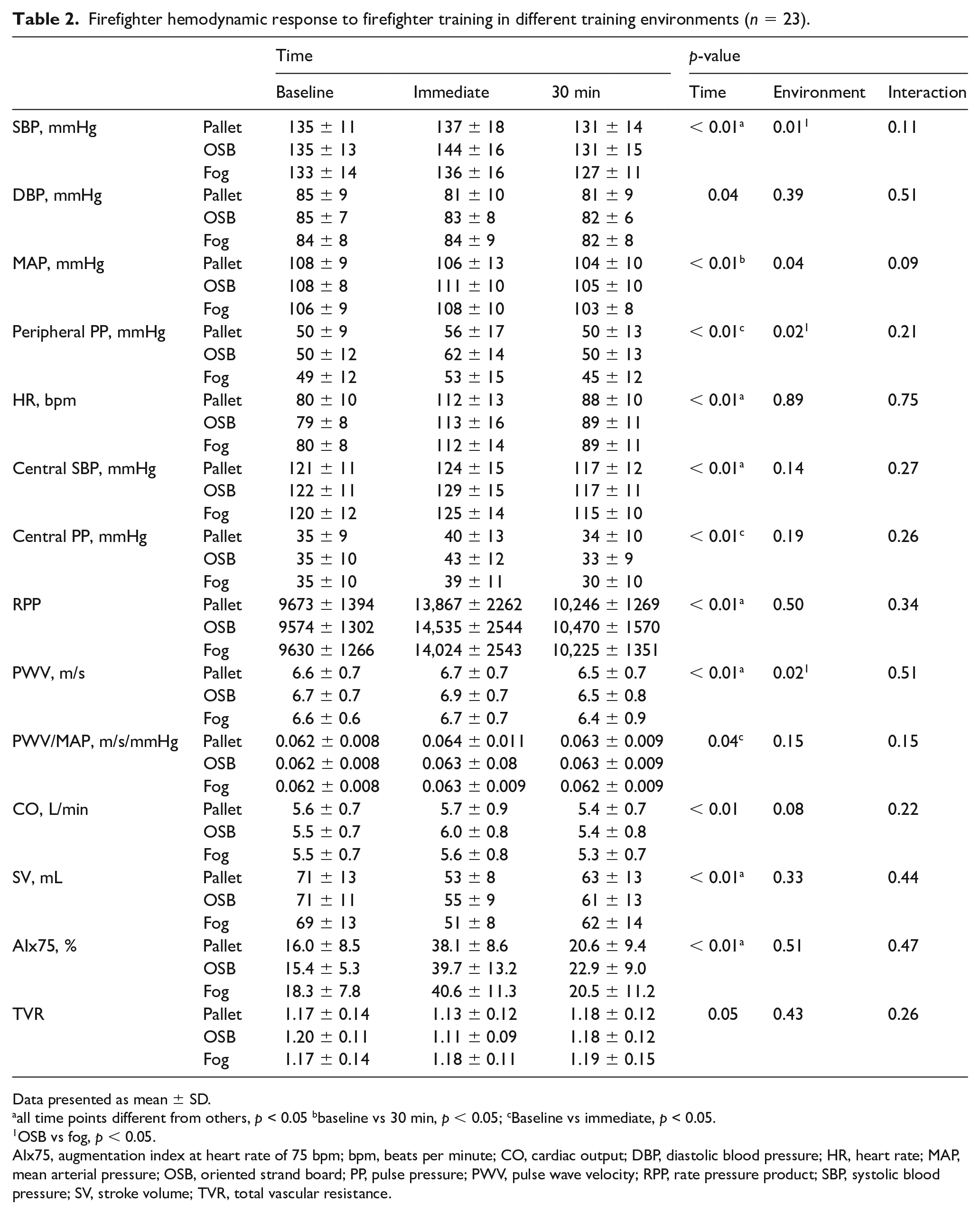
Data presented as mean ± SD.
all time points different from others, p < 0.05 bbaseline vs 30 min, p < 0.05; cBaseline vs immediate, p < 0.05.
OSB vs fog, p < 0.05.
AIx75, augmentation index at heart rate of 75 bpm; bpm, beats per minute; CO, cardiac output; DBP, diastolic blood pressure; HR, heart rate; MAP, mean arterial pressure; OSB, oriented strand board; PP, pulse pressure; PWV, pulse wave velocity; RPP, rate pressure product; SBP, systolic blood pressure; SV, stroke volume; TVR, total vascular resistance.
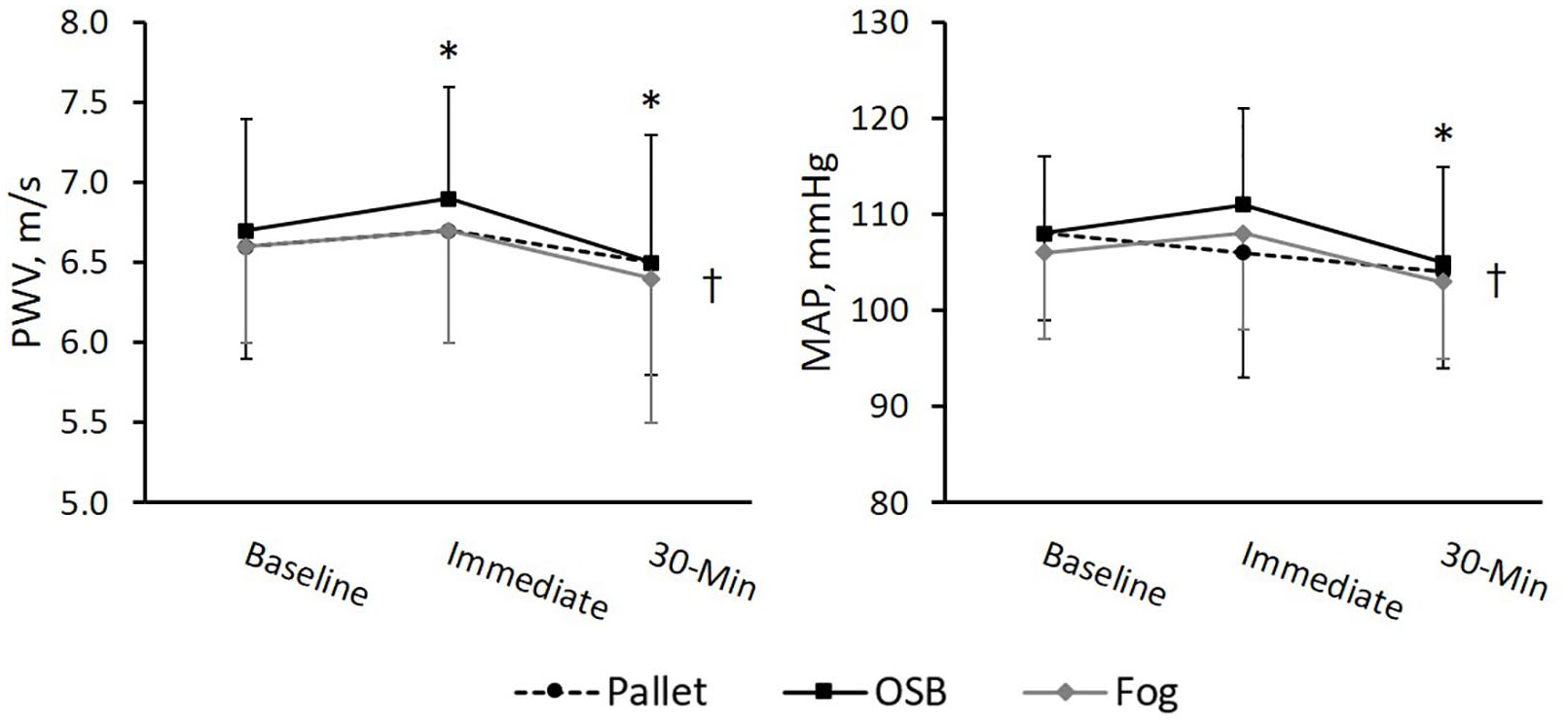
Firefighter PWV and MAP response to firefighter training in different fire environments.
Discussion
To our knowledge, this study is the first to report the hemodynamic response to training environments with different thermal burden and smoke pollutant conditions in firefighters. Our data indicate that even with consistent strenuous work across environments, PWV and systolic, mean, and pulse pressure were higher in firefighters after conducting training in the OSB environment compared to the fog environment; however, the differences in arterial stiffness between environments was likely driven by the increased blood pressure. Cumulatively, our data provide some evidence to suggest the training environment impacts the CV stress placed on firefighters.
As expected, we found an increase in hemodynamic variables following fire training;4,7,15 however, the responses were not different between environments as no interaction effect was observed. We also observed a reduction in SV immediately post-firefighting and 30 minutes following the fire training scenarios,4,6 but coupled with elevated HR, CO was only lower at 30 minutes. Central and peripheral SBP dropped below baseline (~6 mmHg) in the firefighters at 30 minutes post-firefighting, similar to post-exercise hypotension. However, we observed no statistical reduction in TVR (p = 0.052), which was expected given the typical response to an acute exercise bout. This may be explained by the unchanged MAP and CO post-firefighting compared to baseline. Thus, despite observing reductions in SBP, the absence of post-exercise hypotension with MAP at the immediate post-firefighting time point may explain the unexpected discrepancy in TVR.
Interestingly, we observed significant elevations in RPP at 30 minutes in comparison to baseline values (30 min: 10,298 ± 1212; baseline: 9736 ± 1194) during all conditions. The observed elevation in RPP suggests that even during recovery there was an increase in myocardial oxygen demand. Perfusion of myocardial tissue, however, may have declined as we observed a reduction in DBP at 30 minutes. Together this suggests a demand-perfusion mismatch and drop in myocardial perfusion during a period of increased oxygen demand. 16 In combination with the increases in arterial stiffness and augmentation index following fire training activities, our data imply an elevated myocardial load. These data would support the theory that the combination of physical work, heat stress, and CV strain may provide a mechanistic link with increased risk of sudden cardiac events that has been reported following fire suppression activities in firefighters.17,18
We observed a modest overall effect of the OSB environment on vascular hemodynamics compared to the other training environments. We noted higher PWV during OSB in comparison to the fog condition. These training environment condition effects may reflect differences in structural temperatures between the environments, which increased progressively from fog (average environmental temperatures during firefighting ~21°C), to pallet (~40°C), and OSB (~65°C). 8 Similarly, moderate-heat stress induced by exercising with firefighter personal protective equipment has previously been shown to increase carotid arterial stiffness. 19 The larger thermal load incurred by working in the OSB environment likely also contributed to our observations of slightly higher core temperatures and higher blood pressure, in which the higher blood pressure in the OSB condition contributed to the greater PWV. The observed differences in core temperature magnitudes were relatively small and the different training environments led to similar changes over time (p for interaction > 0.05), so heat stress alone may not fully explain the observed changes in vascular hemodynamics. The physical demand required during firefighting could also impact the changes in PWV. Acute resistance and aerobic exercise have been shown to increase and decrease PWV, respectively.20–22 Firefighting activities contain aspects of both resistance and aerobic exercise, so delineating between aerobic and resistance exercise and the influence of other stressors on PWV during firefighting is difficult; however, the increases in PWV may contribute to the increased CV risk with firefighting. Our results may therefore suggest the arterial stiffening and blood pressure response in firefighters is related to the level of heat stress imposed by the surrounding environment and likely the combination of stressors associated with different training environments. For example, these effects may be partially attributed to the different environmental smoke conditions experienced prior to entering the training structure or psychological stress from responding to different training fire environments.
Increasing thermal burden in combination with exercise and psychological stress during live-firefighting drives increases in blood pressure. We observed an increase in core temperature from 37.5°C to 38.6°C, on average, with the highest peak occurring during the OSB environment at 38.8°C. These peak core temperatures are similar to previous training studies of both short and long duration4,23,24 and the change in temperature of approximately 1.1°C falls within the range of 0.3°C to 1.4°C reported by Horn et al. 24 over different firefighting scenarios. Additionally, this peak core temperature is similar to that observed in firefighters combating a fire in a residential structure opposed to a training condition. 25 Surprisingly, we did not observe differences in firefighter HRs during recovery among the three environmental conditions. However, peak HR during the OSB condition was greater than the fog condition. Previous data suggest HR recovers more slowly following hot environment firefighting activities. 5 In the study by Smith et al., 5 the hot environment was 89.6°C whereas our average temperature in the OSB condition was ~65°C throughout the training structure. Thus, participants not being exposed to a thermal burden as large during our training may partially explain these disparate HR recovery results.
Implications
In combination with the previous literature, it appears the mechanism behind the differing hemodynamic load between conditions for firefighters may be the thermal burden in combination with exposure to environmental smoke and stress as training activities in OSB environments elicited a modest effect on hemodynamic parameters. The OSB training fire environment exposed firefighters to a larger radiant heat load, 8 which may increase personal protective equipment temperatures, further increase thermal burden, and increase perceived emotional stress. However, the different smoke chemistry and particulate concentration from the OSB condition merit consideration as factors that may also play a role. 26 Our data indicate that OSB environments create greater CV strain and therefore suggest the environment may impact CV risk for firefighters; however, further research is warranted to fully elucidate its full effects. To maximize training effectiveness and minimize CV (and exposure) risk for firefighters, it is recommended to select training fuels to provide the most realistic training possible, while limiting unnecessary thermal and chemical exposures. In light of the high CV strain associated with firefighting, it is important that firefighters receive proper medical screening and it is essential that the fire service continue efforts to improve the fitness and overall health of firefighters. Finally, monitoring firefighters after completion of firefighting and training may be important to ensure appropriate recovery from exposure to various stressors encountered in any fire environment.
Limitations
This study has important limitations. As these scenarios were conducted following typical training protocols, the participants were aware of the upcoming tasks and may have had an anticipatory response for baseline values. This appears to have minimally influenced the results given the consistency across scenarios and we attempted to minimize the effects by staggering the order the scenarios were completed. Relatively small numbers may have limited our ability to parse differences in environments. We used a validated cuff-based method to estimate arterial stiffness instead of the gold-standard carotid-femoral PWV. Our immediate post-firefighting measures were obtained after firefighters doffed their gear and entered the research facility, allowing a brief time for recovery. Thus, our immediate post-firefighting values do not represent ‘peak’ values. We were unable to investigate the effects of age, sex or obesity on our outcomes despite the variability in our sample, which would be important next steps given the high prevalence of obesity for firefighters in the fire service 27 and the impacts of CV health. Additionally, we are unable to examine the role of physical activity and cardiorespiratory fitness within our sample, which may be important for evaluating CV risk for firefighters. 28
Conclusion
Firefighters are at an increased risk of CV events, with approximately 40–50% of fatalities occurring on-scene (often shortly after fire suppression), 17% of deaths within several hours of an emergency call, and 13% during training. 17 The physical exertion, exposure to ambient smoke pollution as a by-product of combustion, and heat stress associated with firefighting and fire training initiate a large challenge for the CV system as it attempts to maintain cardiac output to active muscles while also dissipating heat. Our results are the first to show the environment in which firefighters are working may influence hemodynamics with firefighting activities. The OSB training fire environment studied here appears to create the largest arterial and hemodynamic burden on firefighters compared to lower environmental temperature, heat flux, and smoke and reduced stress produced by pallet or fog scenarios. Despite a similar hemodynamic response to each environment, the environmental thermal and chemical exposure burden, in combination with the stress and strenuous exercise placed on firefighters, should be considered when designing fire training scenarios and when evaluating CV risk for firefighters.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Department of Homeland Security Fire Prevention and Safety Grant program under Grants EMW-2014-FP-00590 and EMW-2016-FP-00379.
Disclaimer
The findings and conclusions are those of the authors and do not necessarily represent the official position of the National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention.