
Abstract
The tridecapeptide neurotensin has been implicated in the pathogenesis of cardiometabolic disease. Its stable precursor, pro-neurotensin/neuromedin N (pro-NT/NMN), has been associated with composite cardiovascular outcomes including coronary heart disease (CHD) and stroke. The exclusive association of pro-NT/NMN with ischemic stroke has not been evaluated. We conducted a prospective case-cohort study in the REasons for Geographic And Racial Differences in Stroke (REGARDS) study. From 2003 to 2007, REGARDS enrolled 30,239 white or black adults aged ⩾ 45 years. Baseline fasting pro-NT/NMN was measured by immunoassay in the analytic sample including 448 incident ischemic stroke cases and 818 random cohort sample participants. A total of 464 ischemic strokes occurred. Risk of stroke was assessed with a Cox proportional-hazards model incorporating demographic covariates and a second adding stroke risk factors. Increased pro-NT/NMN was associated with ischemic stroke in the demographic model overall (hazard ratio (HR) per standard deviation (SD) pro-NT/NMN 1.16, 95% confidence interval (CI) 1.01–1.33) and in men (HR per SD pro-NT/NMN 1.25, 95% CI 1.04–1.50); HRs were attenuated in the risk factor model. Pre-existing diabetes mellitus and CHD were the largest confounders of ischemic stroke risk, each accounting for an estimated 19% of the association of pro-NT/NMN with ischemic stroke observed in the demographic model. There were no significant interactions of race or sex with pro-NT/NMN. Further research on associations of pro-NT/NMN with stroke risk factors such as diabetes mellitus is indicated.
Introduction
Stroke and cerebrovascular disease have an enormous global burden 1 and considerable variation by geography, 2 race, 3 and sex. 4 Conditions such as diabetes mellitus, coronary heart disease (CHD), and hypertension have long been recognized to augment stroke risk. 5 Neurotensin, a tridecapeptide initially isolated from the central nervous system, 6 is present in relatively massive proportions in the periphery, 7 where it has important effects on metabolism, including insulin resistance and obesity, 8 and may be involved in regulation of blood pressure. 9 Measurement of its stable precursor, pro-neurotensin/neuromedin N (pro-NT/NMN), in humans has implicated the neurotensin-related peptides in risk of obesity, 8 diabetes mellitus, 10 and composite incident cardiovascular disease (CVD) outcomes including CHD events and stroke.10–12 Some associations of pro-NT/NMN with diabetes mellitus10,11 and CVD 10 were specific to or had a greater magnitude in women, suggesting the particular importance of neurotensin in women’s cardiometabolic health. 13
That pro-NT/NMN was not associated with incident CHD events in a recent study from the REasons for Geographic And Racial Differences in Stroke (REGARDS) cohort 14 makes it likely that previously reported associations of pro-NT/NMN with incident composite CVD are driven by an association of pro-NT/NMN with stroke, which has not been exclusively studied. While the risks of CHD and stroke are correlated, there are differences in risk factors, such as the weak association of lipid fraction levels with stroke despite a strong association with CHD. 15 Hence, individuals may have substantially different risk for these two conditions. 16 The purpose of this investigation was to assess the association of pro-NT/NMN with ischemic stroke in REGARDS, a modern, biracial cohort.
Methods
Sample
The REGARDS study was previously described. 17 Briefly, REGARDS enrolled 30,239 black or white participants aged ⩾ 45 years from 2003 to 2007. Black Americans and a region of the southeastern US known as the Stroke Belt were oversampled. Immediate exclusions included insufficient English proficiency, apparent cognitive impairment on telephone interview, active cancer treatment, residence in or waitlisting for a nursing home, and medical conditions precluding long-term follow-up. Medical history and verbal consent were obtained during the initial telephone interview, followed by an in-home visit at which written consent, medication inventory, biometrics, electrocardiogram (EKG), fasting phlebotomy, and urine samples were obtained. The methods of the REGARDS study have been approved by the institutional review board of each involved institution.
Participants or their representatives are surveyed every 6 months by telephone to assess for the presence of stroke occurrence or symptoms. Reports of possible stroke, TIA, or death were screened by a stroke nurse, validated by medical record review, and adjudicated by a committee of stroke experts. Validation of stroke cases required focal neurologic symptoms of ⩾ 24 hours’ duration or nonfocal neurologic symptoms in conjunction with imaging findings suggesting stroke. 18 Stroke events were initially classified as ischemic or hemorrhagic, with ischemic strokes further subclassified according to the TOAST criteria. 19
For this analysis, a random cohort sample of 1127 participants, stratified on age, race, and sex, was drawn from the full REGARDS cohort. 20 In addition to this subcohort, 553 adjudicated cases of incident ischemic stroke occurring prior to September 1, 2011 were identified and added to the random cohort sample to form a raw case-cohort 21 analytic sample. Participants were excluded from analysis based on the criteria shown in Figure 1. Those excluded for being nonfasting were similar to those who were fasting, except they were more likely to have diabetes mellitus or atrial fibrillation (data not shown).
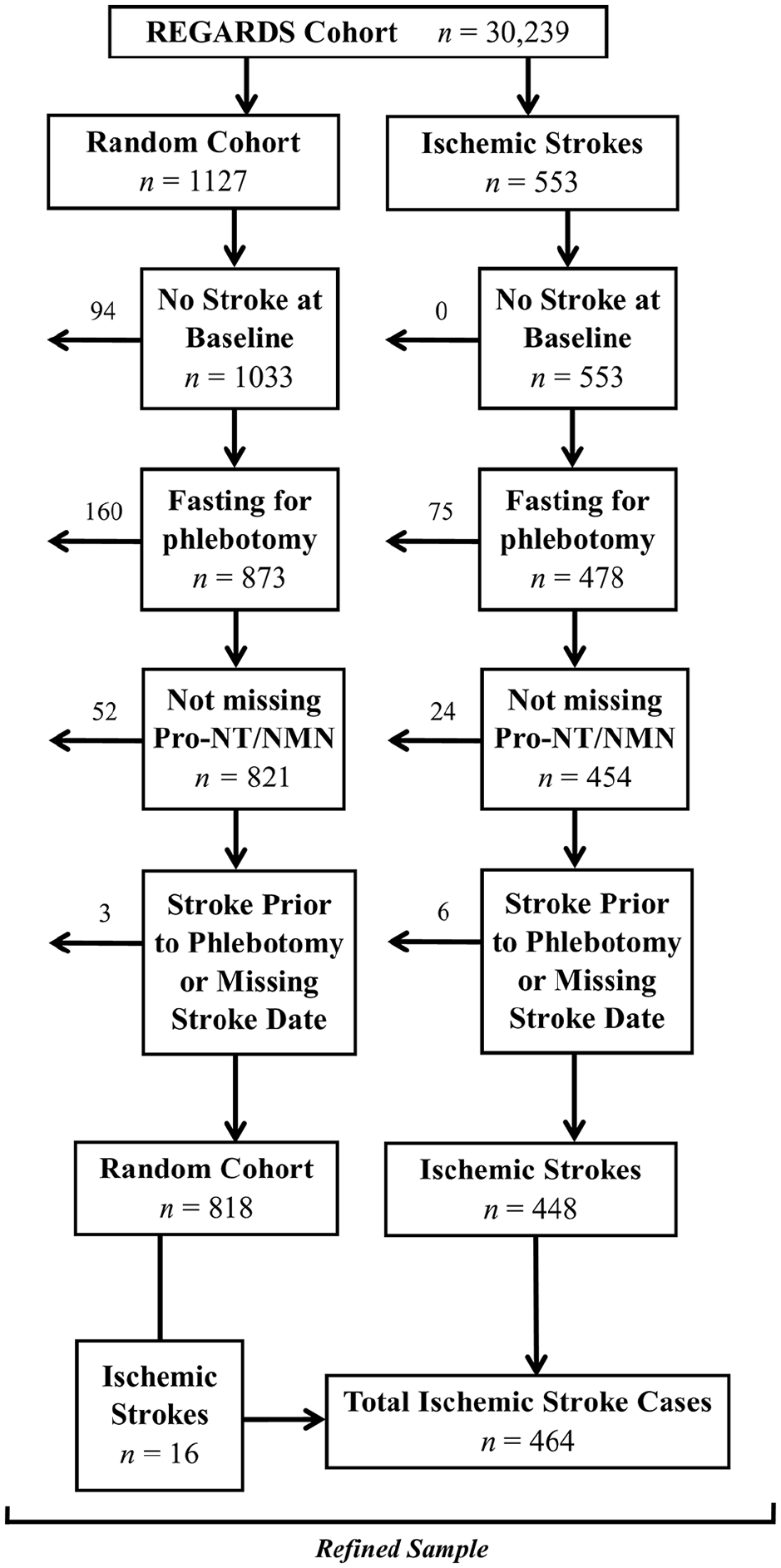
Exclusions of participants from analysis.
Variables
Self-reported demographic variables included age (years), sex, race, education (less than high school graduate, high school graduate, some college, or ⩾ college degree), annual income (< $20,000, $20,000 – $34,999, $35,000 – $74,999, ⩾ $75,000, or refused), geographic region 22 (Stroke Belt, Stroke Buckle, or other), tobacco smoking in pack-years or baseline status (never, current, or past smoker), alcohol use (none, moderate [1–7 alcoholic drinks per week in women, 1–14 alcoholic drinks per week in men], or heavy [> 7 alcoholic drinks per week in women, > 14 alcoholic drinks per week in men]), weekly exercise frequency (none, 1–3 times per week, ⩾ 4 times per week; each occurrence was defined as intense physical activity sufficient to work up a sweat).
Clinical variables included history of stroke (self-reported physician diagnosis), diabetes mellitus (self-reported use of antihyperglycemic medications or insulin or fasting glucose ⩾ 126 mg/dL), CHD (self-reported physician diagnosis of myocardial infarction, coronary revascularization procedure, coronary artery bypass graft surgery, or EKG findings to suggest prior infarct), atrial fibrillation (AF; self-reported physician diagnosis or EKG finding), left ventricular hypertrophy (LVH; EKG finding using Sokolow-Lyon criteria 23 ), hypertension (self-reported use of antihypertensive medications, systolic blood pressure (SBP) ⩾ 130 mmHg, or diastolic blood pressure (DBP) ⩾ 80 mmHg). 24 Body mass index (BMI), in kg/m2, was calculated from baseline height and weight measurements.
Laboratory variables
Fasting blood samples were obtained at the in-home visit, centrifuged locally for 10 minutes, then shipped on ice to the central laboratory at the University of Vermont, where they were re-centrifuged and stored at –80°C. Glucose was measured using colorimetric reflectance spectrophotometry with the Ortho Vitros 950 IRC Clinical Analyzer (Johnson & Johnson Clinical Diagnostics, New Brunswick, NJ, USA). Pro-NT/NMN was measured in the random cohort and stroke cases from thawed EDTA plasma using a single-step sandwich immunoassay (SphingoTec GmbH, Hennigsdorf, Germany) based on a coated tube technique and chemiluminescence label. The assay has a functional sensitivity of 10 pmol/L, detection limit of 1.9 pmol/L, and interassay precision of 20% of the coefficient of variation (5–9%). Pro-NT/NMN assays were performed at an independent laboratory (ICI Immunochemical Intelligence GmbH, Berlin, Germany) by technicians who were blinded to clinical data.
Statistical analysis
All analyses were weighted to account for case-cohort design, using a Taylor series as a finite population correction, and were two-sided with α = 0.05 and interaction α = 0.10. Pro-NT/NMN was positively skewed and was thus common logarithm-transformed for continuous analyses or quartiled for other analyses. Baseline variables were tabulated by pro-NT/NMN quartiles, with Pearson chi-squared tests with second-order correction according to Rao and Scott 25 used to compare categorical variables and simple linear regression used to compare continuous variables.
Two multivariable Cox proportional-hazards models 26 were fitted to examine the association of baseline pro-NT/NMN with ischemic stroke. Model 1 included demographic variables: age, sex, region, income, education, and an age*race multiplicative interaction term (previously shown to be significant in REGARDS). 27 Model 2 added Framingham Stroke risk factors: SBP, antihypertensive drug use, smoking, baseline diabetes mellitus, CHD, AF, and LVH. 28 The association of log pro-NT/NMN with ischemic stroke was presented visually with sex-stratified restricted cubic splines, with prespecified knots determined by Harrell’s method 29 and referencing the sex-specific median. Kernel density plots show distributions of log pro-NT/NMNN stratified by sex.
Stroke-free survival time was measured from date of phlebotomy (in-home visit) to date of stroke or censoring. Those who did not develop stroke in follow-up were censored on the earliest date of: last follow-up, death, or September 1, 2011 (index date of case-cohort creation). Failure date was the adjudicated date of stroke cases. The interaction of sex and race with log pro-NT/NMN was tested with multiplicative interaction terms.
An attenuation analysis was planned to examine the potential confounding of stroke risk factors (Model 2) on an overall or group-specific association of log pro-NT/NMN with stroke. Model 1 covariates were used as a base, yielding HRModel 1. Each Model 2 covariate was individually and separately added to this base model, producing HRModel 1 + Risk Factor. The estimated attenuation of a Model 1 association of pro-NT/NMN with stroke was calculated accordingly:
Statistical analysis was conducted with Stata, version 16.0 (StataCorp, College Station, TX, USA).
Results
Sample characteristics
A total of 1266 participants were included following exclusion criteria shown in Figure 1: 818 from the cohort random sample (including 16 incident ischemic strokes), and 448 incident ischemic stroke cases from the remainder of the REGARDS cohort. Thus, there were 464 ischemic strokes occurring over the median follow-up time of 4.7 years (IQR 2.5–6.4 years). Of the incident ischemic strokes, 94 (20.3%) were cardioembolic, 78 (16.9%) were small-vessel, 59 (12.7%) were large-vessel, and 233 (50.2%) were of a miscellaneous but known cause or had an unclassifiable cause based on available data.
Baseline characteristics
In the cohort random sample, pro-NT/NMN ranged from 21 pmol/L to 1278 pmol/L, with median 169 pmol/L and interquartile range 105–273 pmol/L. Table 1 shows baseline characteristics of cohort random sample participants across pro-NT/NMN quartiles. Higher quartiles of pro-NT/NMN had larger proportions of participants who were less educated, of a lower annual income category, not current alcohol users, and had pre-existing diabetes mellitus or hypertension (p < 0.05).
Baseline characteristics of cohort random sample a by pro-NT/NMN quartile (n = 818).
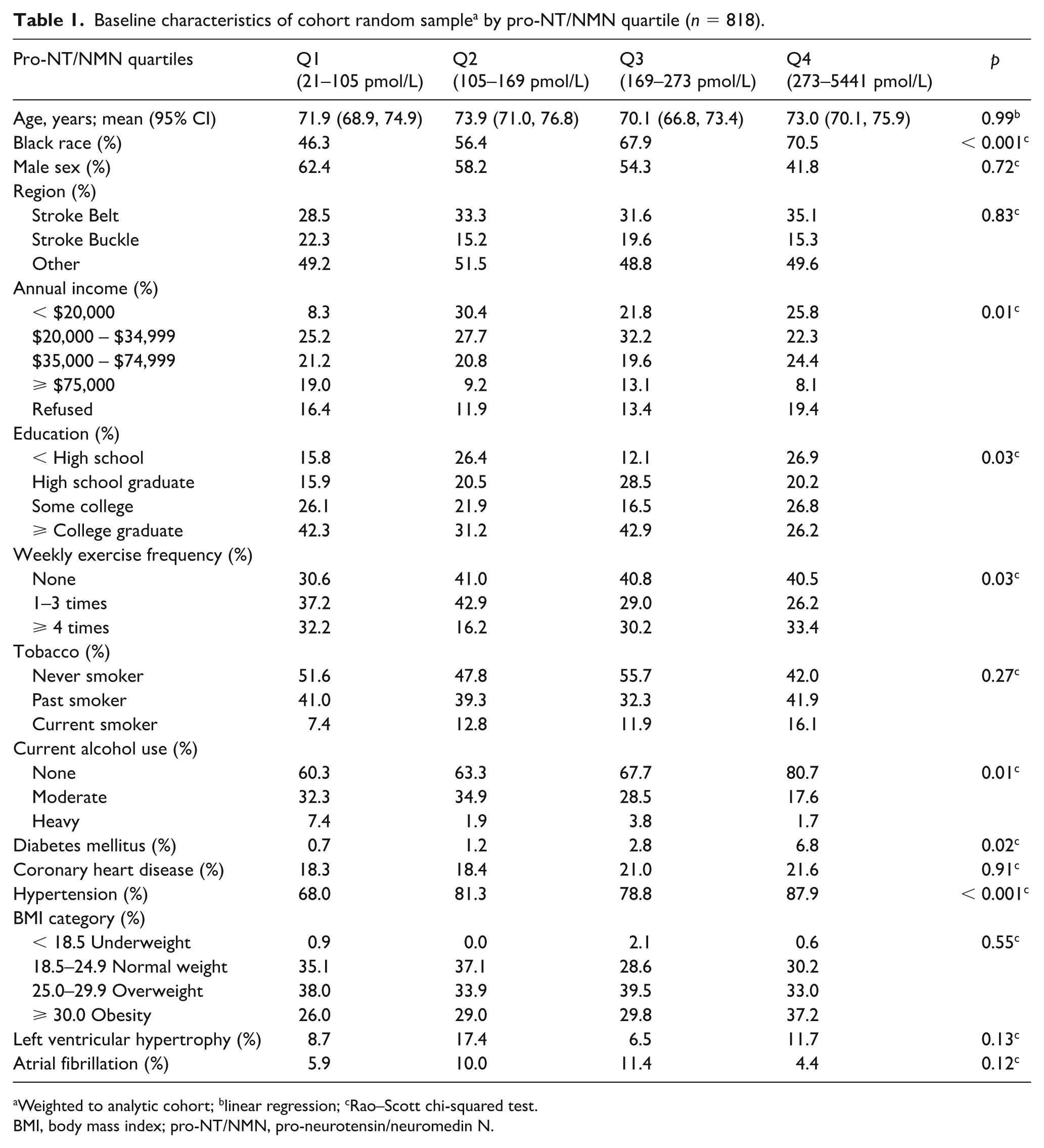
Weighted to analytic cohort; blinear regression; cRao–Scott chi-squared test.
BMI, body mass index; pro-NT/NMN, pro-neurotensin/neuromedin N.
Association of pro-NT/NMN with incident ischemic stroke
Table 2 shows an association of increased pro-NT/NMN with risk of ischemic stroke in Model 1 (HR per SD log pro-NT/NMN 1.16, 95% CI 1.01–1.33; 4th versus 1st quartile, HR 1.49, 95% CI 1.04–2.15), with a significant trend of increased risk across successive quartiles (p = 0.03). This association was not maintained with further adjustment for stroke risk factors.
Hazard ratio (95% CI) for ischemic stroke by pro-NT/NMN, overall and stratified by sex. a
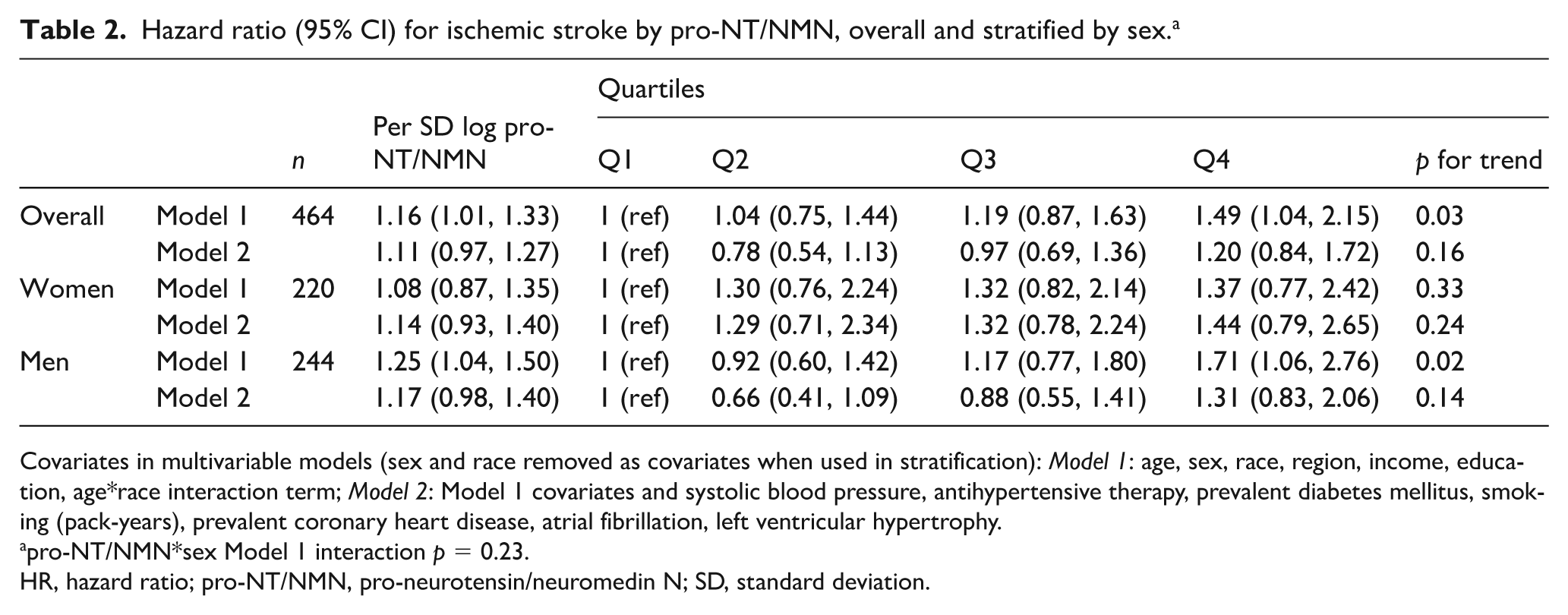
Covariates in multivariable models (sex and race removed as covariates when used in stratification): Model 1: age, sex, race, region, income, education, age*race interaction term; Model 2: Model 1 covariates and systolic blood pressure, antihypertensive therapy, prevalent diabetes mellitus, smoking (pack-years), prevalent coronary heart disease, atrial fibrillation, left ventricular hypertrophy.
pro-NT/NMN*sex Model 1 interaction p = 0.23.
CI, confidence interval; HR, hazard ratio; pro-NT/NMN, pro-neurotensin/neuromedin N; SD, standard deviation.
Similarly, increased pro-NT/NMN was associated with ischemic stroke in men with minimal adjustment (HR per SD log pro-NT/NMN 1.25, 95% CI 1.04–1.50; 4th versus 1st quartile, HR 1.71, 95% CI 1.06–2.76), with a significant trend across quartiles (p = 0.02); this association was attenuated in the full model. No association of pro-NT/NMN with ischemic stroke was observed in women; the apparent sex difference was not statistically significant (interaction p = 0.23 in Model 1). The online supplemental Figure 1 shows sex-stratified restricted cubic splines of the association of pro-NT/NMN with incident ischemic stroke. The association of pro-NT/NMN with ischemic stroke did not differ by race (interaction p = 0.41 in Model 2).
Online supplemental Table 1 reports the associations of pro-NT/NMN with ischemic stroke subtypes. Pro-NT/NMN was not associated with a specific risk of small-vessel, large-vessel, or cardioembolic stroke, but an association of log pro-NT/NMN with miscellaneous or unclassified stroke was observed in the fully adjusted model (HR per SD log pro-NT/NMN 1.22, 95% CI 1.03–1.44).
Attenuation analysis of association of pro-NT/NMN with ischemic stroke
As shown in Table 3, pre-existing diabetes mellitus and CHD were the most prominent confounders of the association of log pro-NT/NMN with incident stroke, each accounting for an estimated 19% of the per SD log pro-NT/NMN risk of ischemic stroke. For men, CHD at baseline was the most prominent confounder, accounting for an estimated 12% of the per SD log pro-NT/NMN hazard of ischemic stroke.
Covariate attenuation of the association of log pro-NT/NMN with ischemic stroke in Model 1.
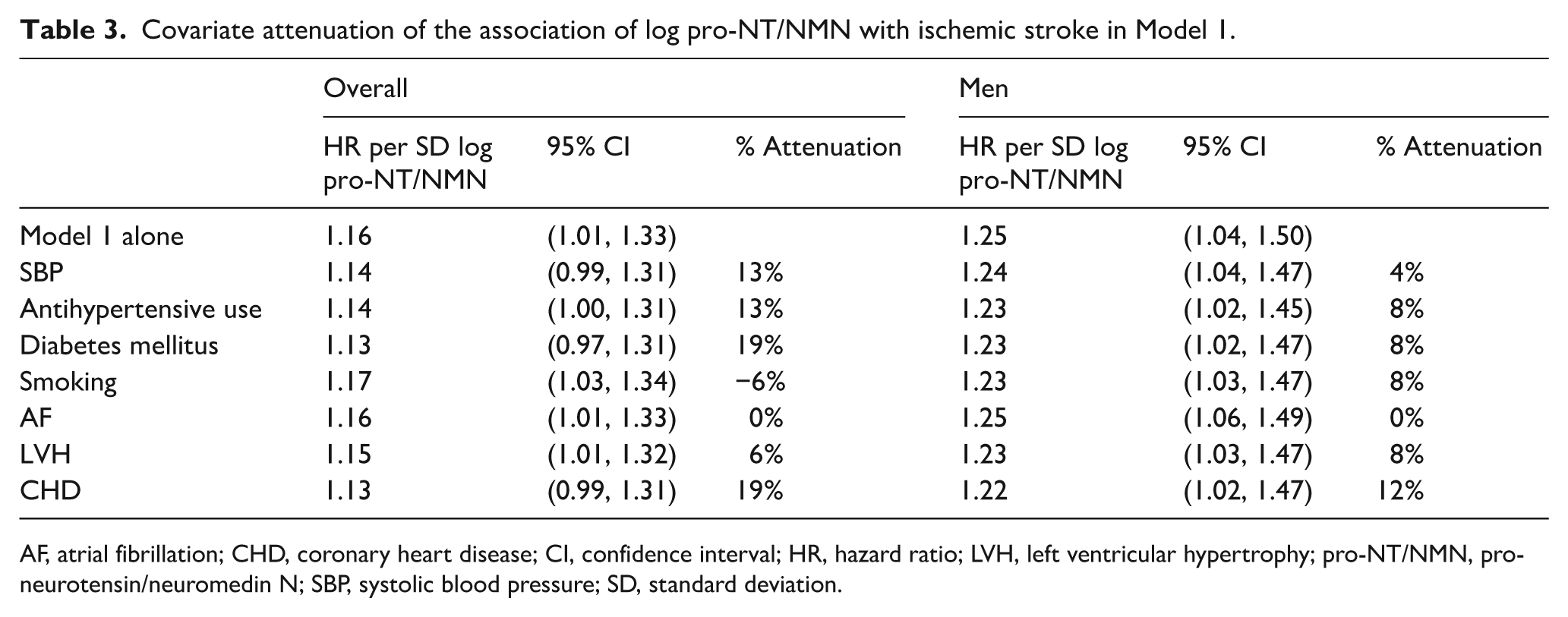
AF, atrial fibrillation; CHD, coronary heart disease; CI, confidence interval; HR, hazard ratio; LVH, left ventricular hypertrophy; pro-NT/NMN, pro-neurotensin/neuromedin N; SBP, systolic blood pressure; SD, standard deviation.
Discussion
In this prospective case-cohort study within the modern and biracial REGARDS study, higher baseline plasma pro-NT/NMN was associated with increased risk of ischemic stroke overall and in men when controlling for participant demographics. Specifically, participants with a 4th versus 1st-quartile pro-NT/NMN had a 49% increased ischemic stroke risk overall; men had a 71% increased risk when controlling for demographics. These associations were attenuated after controlling for traditional stroke risk factors. Together, these findings suggest that pro-NT/NMN augments stroke risk – particularly in men – through its influence on traditional stroke risk factors such as diabetes mellitus and CHD.
Our findings are consistent with reports of three previous epidemiologic studies, which found a 10–24% increased risk of composite CVD per SD higher pro-NT/NMN.10–12 However, unlike previously documented women-specific or larger-magnitude associations of pro-NT/NMN in women with composite CVD10,12 and diabetes mellitus,10,11 we did not observe similar sex differences in the association of pro-NT/NMN with ischemic stroke. Rather, we observed a 25% increased risk of ischemic stroke per SD log pro-NT/NMN in men but no association in women, although the difference in associations by sex was not statistically significant. We find it most probable that this discordance is due to the exclusive study of stroke in the present investigation. This notion underscores that, while stroke and myocardial infarction share some common risk factors, they are separate disease processes with heterogenous etiologies. Thus, their separate consideration as outcomes in human epidemiologic studies may improve validity.
We expected to find some differences in associations of pro-NT/NMN with subtypes of ischemic stroke. Surprisingly, and unlike N-terminal pro-B-type natriuretic peptide, 30 pro-NT/NMN was not associated with cardioembolic stroke. Together with the observed lack of association of pro-NT/NMN with atrial fibrillation, findings suggest pro-NT/NMN does not reflect atriopathy leading to stroke.
The association of pro-NT/NMN with ischemic stroke is plausibly related to the influence of the neurotensinergic peptides and their receptors on inflammation 31 and metabolism. Pro-NT/NMN was previously associated with incident diabetes mellitus,10,11 which substantially confounded the association of pro-NT/NMN with stroke in this study. This may be rooted in insulin resistance occurring as a result of neurotensin-driven augmentation of dietary fatty acid absorption.8,32 Variation at the SORT1 gene, encoding a receptor to which neurotensin is a ligand, has been critically linked to CVD risk 33 and insulin resistance. 34 Accordingly, broader exploration of the interplay between pro-NT/NMN, diabetes mellitus, and dietary patterns in human subjects is necessary to fully explain these findings. As SBP and use of antihypertensive drugs also appreciably confounded the association of pro-NT/NMN with stroke, investigation of the association of pro-NT/NMN with hypertension is similarly warranted.
Study limitations and strengths
Several limitations of this study must be considered. Firstly, the generalizability of findings to race groups other than black or white is limited. Participants excluded for not fasting prior to phlebotomy were more likely to have atrial fibrillation and diabetes mellitus at baseline; omission bias might have occurred. Such a bias would likely push findings toward the null, except in the setting that excluded participants, like those with more severe diabetes mellitus who did not fast, might have different relationships of pro-NT/NMN with stroke. That a large number of ischemic strokes were not classifiable into subtype is a potential limitation of the subtype-stratified results. These strokes likely represent the range of stroke etiologies and were not classified primarily due to lack of a definite etiology as documented in medical records. Baseline characteristics and pro-NT/NMN levels did not differ among miscellaneous or unclassified stroke cases and the other ischemic stroke cases (data not shown). Lastly, pro-NT/NMN was measured at varied times from participants’ individual phlebotomy dates, raising concern for time-related breakdown of the molecule in storage, but this is unlikely given the general stability of peptides in frozen storage at –80°C or colder. 35
This study has several strengths. REGARDS is a large, prospective, and population-based cohort with ongoing follow-up and high retention (87.3% cumulative retention). 30 While previous cohort studies evaluating the association of pro-NT/NMN with aggregate CVD were ethnically homogenous,36–38 REGARDS is the first study we are aware of to measure pro-NT/NMN in a significant proportion of non-white participants, improving on the generalizability of these findings. The rigorous screening and adjudicating of stroke cases by stroke experts minimized misclassification bias, although subtype could often not be determined. Semiannual monitoring for stroke and the addition of biometry and laboratory testing to participant self-report in establishing diagnoses of medical conditions further bolster the integrity of these data.
Conclusion
In this large and modern prospective cohort, increased baseline pro-NT/NMN was associated with increased risk of ischemic stroke when controlling for demographic factors. This finding may be specific to men, standing in contrast to prior investigations associating pro-NT/NMN with aggregate cardio- and cerebrovascular outcomes with findings specific to women. Pro-NT/NMN was not significantly associated with ischemic stroke when controlling for traditional stroke risk factors, and the less adjusted association was especially explained by the confounding effects of pre-existing diabetes mellitus and CHD. Further study of the relationship of pro-NT/NMN with incidence of stroke risk factors such as diabetes mellitus and hypertension is warranted.
Supplemental Material
ProNT_Supp_VascMed_18AUG – Supplemental material for Pro-neurotensin/neuromedin N and risk of ischemic stroke: The REasons for Geographic And Racial Differences in Stroke (REGARDS) study
Supplemental material, ProNT_Supp_VascMed_18AUG for Pro-neurotensin/neuromedin N and risk of ischemic stroke: The REasons for Geographic And Racial Differences in Stroke (REGARDS) study by Charles D Nicoli, Nicholas Wettersten, Suzanne E Judd, George Howard, Virginia J Howard, Joachim Struck and Mary Cushman in Vascular Medicine
Footnotes
Acknowledgements
Declaration of conflicting interests
Dr Struck is employed by SphingoTec Gmbh, which funded measurement of pro-neurotensin/neuromedin N. The other authors report no disclosures.
Funding
This research is supported by cooperative agreement U01 NS041588 co-funded by the National Institute of Neurological Disorders and Stroke (NINDS) and the National Institute on Aging (NIA), National Institutes of Health, Department of Health and Human Services. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NINDS or the NIA. Representatives of the NINDS were involved in the review of the manuscript but were not directly involved in the collection, management, analysis or interpretation of the data.
Supplemental material
The supplemental material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.