
Abstract
Objective
To evaluate the value of the urocortin (UCN) level to predict preterm delivery in women with threatened preterm labour.
Methods
This prospective cohort study included 96 women with a singleton pregnancy between 28 and 34 weeks of gestation who were admitted with threatened preterm labour. The participants were monitored until delivery. The UCN level was compared between those with preterm and with full-term deliveries.
Results
The mean UCN level was higher for preterm deliveries (96 ± 24.34 pg/mL) than for full-term deliveries (62.62 ± 23.63 pg/mL). A UCN cutoff level of 92 pg/mL had 20% sensitivity, 100% specificity, 100% positive predictive value, and 10% negative predictive value. Thus, 17.7% of women had a UCN level ≥ 92 pg/mL, and all delivered preterm. Among the 82.3% of women who had a UCN level < 92 pg/mL, 88.6% delivered preterm, and 11.4% delivered at full term. Moreover, 88.2% of women who had a UCN level ≥ 92 pg/mL delivered within 7 days and only 11.8% delivered after 7 days. However, 58.2% of women with a UCN level < 92 pg/mL delivered within 7 days and 41.8% delivered after 7 days.
Conclusion
A UCN cutoff level of ≥92 pg/mL predicts preterm delivery within 7 days of admission.
Keywords
Introduction
Preterm birth is defined as the delivery of a baby before completing 37 weeks of pregnancy. 1 This can occur spontaneously (spontaneous preterm labour) or may be medically indicated (indicated preterm labour) as in the case of preeclampsia, intrauterine growth restriction, or maternal diseases. 2 The incidence of preterm birth is approximately 5.0% to 10% and varies according to geographic distribution. Global statistics have shown approximately 15 million babies are born preterm annually, which differs significantly in various parts of the world. 3 Preterm birth is a significant complication of pregnancy and is responsible for considerable neonatal morbidity and mortality. Nearly 3.1 million babies die each year as a direct result of premature birth. 4 Approximately 85% of early neonatal deaths among infants that do not result from congenital malformation are attributed to preterm birth. 2
Preterm birth is also the leading cause of mortality under the age of five worldwide, accounting for 52% of children's deaths in 2013. 5 Preterm delivery is not a single disease. However, it is a syndrome that might result from one or multiple causes. Several mechanisms, except for true cervical weakness or incompetency, have described the pathogenesis of preterm labour. These mechanisms appear to share a final common pathway encompassing the upregulation of prostaglandin, uterotonic agents, and enzymes that weaken the foetal membrane and degrade the cervical stroma. Activation of the foetal hypothalamic-pituitary-adrenal axis, which was previously hypothesized as a possible initiating mechanism in normal labour, may also be involved in preterm labour. 6
Preterm birth is the single most important cause of morbidity and mortality in neonates worldwide. Identifying women at risk of spontaneous preterm birth and applying screening tests is therefore important, as this may allow preventative measures to reduce preterm birth and related complications. 1
Urocortin (UCN) consists of 40 amino acid residues and belongs to the neuropeptide family linked to corticotrophin-releasing factor (CRF). The UCN sequence is 45% homologous to that of CRF. Studies have demonstrated that UCN and CRF increase uterine contractility stimulated by endometrial prostaglandin F2a. UCN stimulates adrenocorticotropic hormone and prostaglandin E2 secretion by the trophoblast and has a vasodilatory effect on the placenta. 7 UCN also up-regulates myometrial expression of pro-inflammatory cytokines via corticotropin-releasing hormone receptor 2 because of the likely positive feedback loop between UCN and inflammatory cytokines. UCN expression is increased by the inflammatory stimulus tumour necrosis factor-alpha, probably through NF-κB signalling. 8
From the first to third trimesters of pregnancy, UCN shows stable concentrations in maternal plasma. However, maternal plasma levels of CRF and UCN were increased in patients with preterm deliveries and decreased in those with post-term deliveries compared with term pregnancies and coincided with labour onset. 9 The fine-regulated expression of these neuropeptides seems essential in setting the length of human gestation. 10 Thus, this study aimed to evaluate the value of the serum UCN level in predicting preterm delivery in pregnant women presenting with threatened preterm labour.
Patients and methods
Study design and setting
This prospective cohort study was conducted at Sulaimani Maternity Teaching Hospital, Sulaimaniyah City, Iraq, over 9 months, from 1 April 2022 to 31 December 2022.
Inclusion criteria
The participants included women with a singleton pregnancy and a gestational age between 28 and 34 weeks who presented with regular uterine contractions, cervical dilation of ≤3.0 cm, and intact membranes.
Exclusion criteria
Women with multiple pregnancies, diabetes mellitus, preeclampsia, antepartum haemorrhage, intrauterine growth restriction, foetal anomalies, and preterm pre-labour rupture of membranes were excluded.
Study protocol
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 11 After hospital admission, a detailed history was obtained from the consecutively selected women, followed by a complete examination using a standard questionnaire. Gestational ages were calculated from the last menstrual period and confirmed by early ultrasound (before 20 weeks of gestation). Other clinical data, including maternal age, the number of births that the women had after 24 weeks of gestation (para), the total number of confirmed pregnancies (gravida), and the number of abortions, were obtained. Then, blood samples were collected before any interventions, such as betamethasone and tocolytic drug administration. Briefly, 2.0 mL of venous blood was drawn from each patient, collected in an EDTA tube, and centrifuged immediately at 277 × g for 15 minutes; the supernatant was collected and stored at −70°C until the UCN determination assay was performed. The UCN concentration was then measured using an Abbexa® ELISA kit (Abbexa, Cambridge, UK). The participants were then followed up until their delivery and were divided into two groups: those who delivered preterm (before completing 37 weeks) and those who delivered at term (≥37 completed weeks). Then, their serum UCN levels were compared.
Ethical considerations
Ethical approval was obtained from the Ethical Committee of the College of Medicine, University of Sulaimani, Sulaimaniyah, Iraq, with reference number 34 on 4 April 2022. This study was conducted according to the Helsinki Declaration of 1975 as revised in 2013. Approval of the Institutional Review Board of Sulaimani Maternity Teaching Hospital, Sulaimaniyah City, Iraq, was also obtained (number 04 on 15 March 2022). Participants were informed regarding the nature and purpose of the study, and then written informed consent was obtained. De-identified patient details were used for the study.
Statistical analysis
The GPower 3.1 program (IBM Corp., Armonk, NY, USA) was used to estimate the sample size to obtain a study power of >95%, and IBM SPSS Statistics (version 25, IBM Corp.) was used for the data analysis. In addition, the Pearson chi-square test was used to determine the association between independent and dependent variable pairs, and the Pearson R correlation was used to calculate the direction of the association between the two variables. A value of p ≤ 0.05 was considered statistically significant. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and likelihood ratio for the UCN level were then calculated.
Results
The study included 96 pregnant women who were admitted to the hospital with threatened preterm labour during the study period. Regarding the patients’ sociodemographic data, the mean age of the participating women was 27.7 ± 6.6 years (ranging from 15–43 years), the mean gravida was 2.8 ± 1.8 (ranging from 1–8), the mean para was 1.4 ± 1.4 (ranging from 0–5), the mean number of abortions was 0.4 ± 0.8 (ranging from 0–4), the mean gestational age at admission was 32.6 ± 1.5 weeks (ranging from 28–34.4 weeks), and the mean gestational age at delivery was 34.1 ± 2.2 weeks (ranging from 29–39 weeks) (Table 1).
Sociodemographic characteristics of the participating pregnant women.

SD: standard deviation.
Among the participating pregnant women (n = 96), 87 (90.6%) delivered preterm, and only 9 (9.4%) delivered at full term. The mean plasma UCN level in women who delivered preterm was higher than that in those who delivered at term (96 ± 24.34 pg/mL versus 62.62 ± 23.63 pg/mL), but without a significant difference (p = 0.34). Seventeen women had UCN levels ≥92 pg/mL (17.7%), and all delivered preterm (≤37 weeks). The remaining 79 women (82.3%) had UCN levels < 92 pg/mL; among those, 70 (88.6%) delivered preterm (≤37 weeks) and 9 (11.4%) delivered at full term (38–40 weeks), (p = 0.14) (Table 2). Receiver operating characteristic (ROC) curve analysis revealed that a UCN cutoff value of 92 pg/mL had a sensitivity of 20%, specificity of 100%, PPV of 100%, and NPV of 10% as a marker for preterm labour (Figure 1 and Table 2).
Correlation between urocortin level and gestational age at delivery.

LR: likelihood ratio, NPV: negative predictive value, PPV: positive predictive value.

Receiver operating characteristic (ROC) curve for serum urocortin level and gestational age. Diagonal segments are produced by ties.
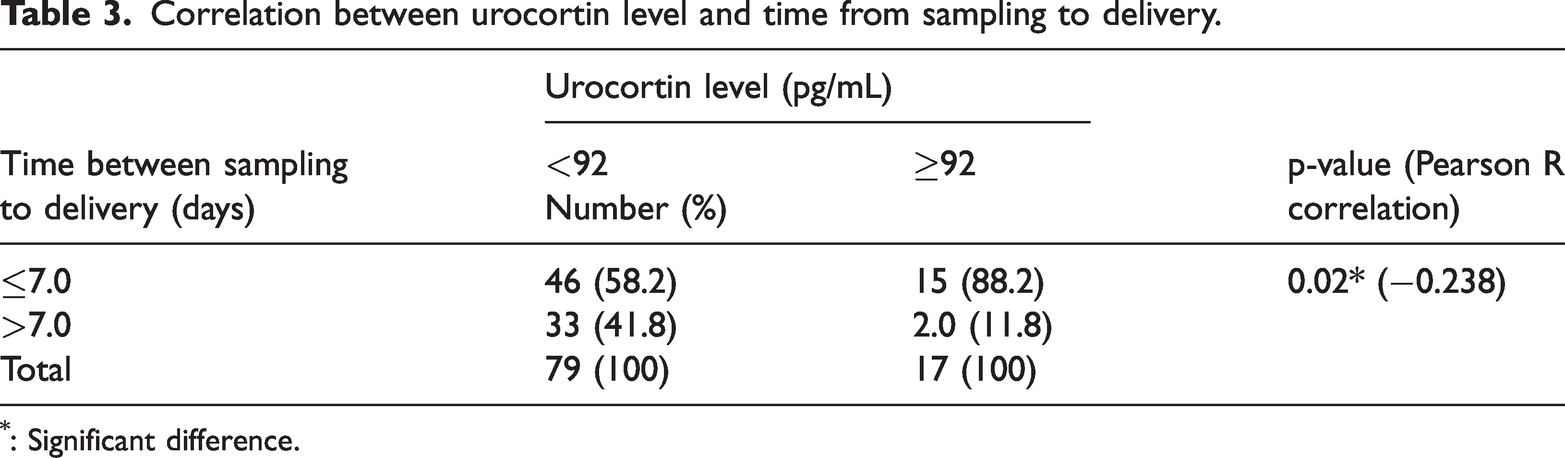
Regarding the correlation of the time from admission/sampling to delivery with the UCN level, among the 17 women who had a UCN level ≥ 92 pg/mL, 15 (88.2%) delivered within 7 days and only 2 (11.8%) delivered after 7 days. Among 79 women who had a UCN level of <92 pg/mL, 46 (58.2%) delivered within 7 days and 33 (41.8%) delivered after 7 days, with a significant difference (p = 0.02) between the two groups (Table 3).
Correlation between urocortin level and time from sampling to delivery.
: Significant difference.
Discussion
Maternal plasma UCN levels are correlated with the contractility status of the human myometrium. This study evaluated the value of the maternal plasma UCN level as a biomarker to predict preterm delivery in women with threatened preterm labour. Among the 96 women studied, 90 (90.6%) delivered preterm, and 9 (9.4%) progressed to full term. The mean UCN level was higher in those who delivered preterm (96 ± 24.34 pg/mL) than in those who delivered at full term (62.62 ± 23.63 pg/mL), but without a significant difference. This result was similar to that of Kashanian et al., who found that the mean serum level in women who delivered preterm (92.5%) was higher (392.6 ± 29.23 pg/mL) than that in women who delivered at full term (113.2 ± 11.0 pg/mL), but without a significant difference (p = 0.252). 8 In contrast, an observational study by Florio et al. including 85 women with a singleton pregnancy (28–34 completed gestational weeks) with threatened preterm labour showed that 35.3% of patients had preterm delivery within 7 days of admission, whereas the remaining patients delivered later. They also found that the UCN level was significantly higher in women who delivered preterm (median 131.2 pg/mL, with an interquartile interval of 115.1–139.4 pg/mL) than in those who progressed to term delivery. 12
In this study, the ROC curve analysis revealed that a UCN level of ≥92 pg/mL can predict preterm labour with 100% specificity and 100% PPV, as all women with a UCN level of ≥92 pg/mL delivered preterm within 7 days, while a level of <92 pg/mL had only a 10% NPV for preterm delivery. A ROC curve analysis was performed to assess the predictive power of plasma UCN.
The area under the ROC curve in the current study was 0.59, with an insignificant association between the UCN level and gestational age (p = 0.34). This finding was consistent with that of Kashanian et al., whose area under the ROC curve was 0.618, which was of no diagnostic value for predicting delivery < 48 hours from the beginning of labour pain. 8
The area under the ROC curve regarding the ability of plasma UCN to predict deliveries at <32 weeks was 0.5, which also showed no significant diagnostic value. In a study by Sabaa in 2016, the ROC curve analysis was performed using the DeLong method to assess the predictive power of the plasma UCN level, C-reactive protein level, and white blood cell count for delivery within 7 days. Only the plasma UCN level showed a significant ROC curve value with a high area under the curve (the best cutoff criterion of the plasma UCN level was >365.2 pg/mL). They also found that the plasma UCN level had a highly significant predictive power for delivery within 7 days, 13 which disagrees with the result of this study. Furthermore, in the study by Florio et al., ROC curve analysis revealed that a plasma UCN concentration at or above the cutoff value of 113.9 pg/mL was increased among women with threatened preterm labour and preterm delivery, and the authors suggested plasma UCN measurement as a biochemical marker to assess preterm delivery. 12
Regarding the correlation between other molecules (rather than UCN) and preterm labour, Özdemir et al. found no relationship between the maternal galectin-9 level and threatened preterm labour in complicated pregnancies. 14
The limitation of this study is that it is a single institutional-based study with limited cases and a short duration.
Conclusions
Although the UCN level was higher in women with preterm labour than in women progressing to term labour, the difference was not statistically significant. However, a UCN cutoff level of ≥ 92 pg/mL may predict preterm delivery within 7 days of admission. Further studies with larger sample sizes are needed to verify the value of UCN in predicting preterm labour.
Footnotes
Acknowledgements
I would like to express my gratitude to the senior house officer who work in the Maternity Teaching Hospital (Dr. Banaz Jamal) for her help during sample collection and patient monitoring.
Declaration of conflicting interests
The author declares that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.