
Abstract

What is cholesterol? What are lipids? Why are they important?
Cholesterol and other lipids are fat-like, waxy substances that circulate through the blood. Although the terms ‘cholesterol’ and ‘lipids’ are sometimes used to mean the same thing, cholesterol is one type of lipid that is commonly monitored on blood testing because of its effects on cardiovascular (heart and blood vessel) health.
Cholesterol is made by the liver and is also consumed through foods in the diet. A certain amount of cholesterol within the body is normal – cholesterol is used to build cells and hormones for normal functioning.
Elevated lipid levels (called ‘hyperlipidemia’) or imbalanced lipid levels (‘dyslipidemia’) can lead to heart and blood vessel disease, such as heart attack, stroke, or peripheral artery disease (PAD). Hyperlipidemia and dyslipidemia are the medical terms used to describe cholesterol and lipid problems. It is important to recognize and treat these conditions to reduce the risk of cardiovascular disease. 1
What is meant by ‘bad’ and ‘good’ cholesterol? What are the different lipids shown on a blood test?
There are a few main lipid types that are commonly measured in the blood, and they each have different roles.
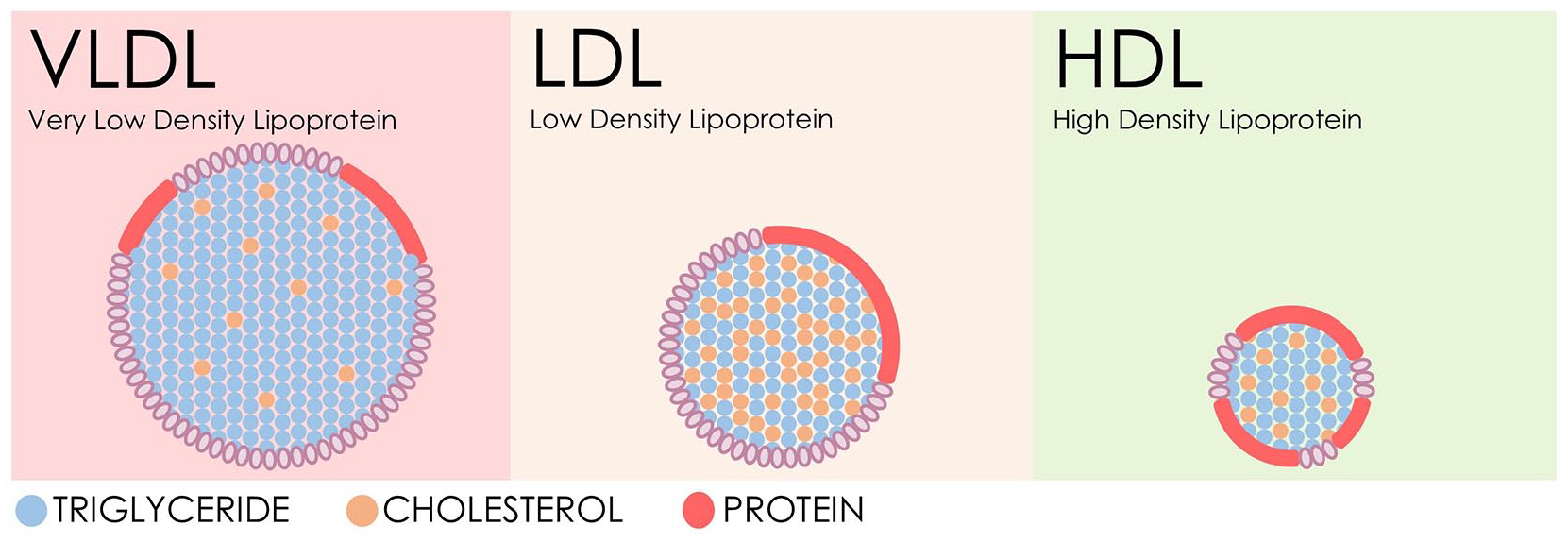
Cholesterol subtypes include very low-density lipoprotein (VLDL), low-density lipoprotein (LDL), and high-density lipoprotein (HDL). These three components make up the total cholesterol.
Cholesterol is transported through the blood in packages called
What is the ideal cholesterol level?
The goal levels for cholesterol partly depend on a person’s overall risk of cardiovascular disease and other health factors. For example, the target level for LDL is much lower in patients who have had a heart attack or stroke. There can also be differences in laboratory measurements or calculations used to determine values, so it is important to work with a physician to determine individual goals.
A general guide is given in Table 1.
General guide for cholesterol levels.
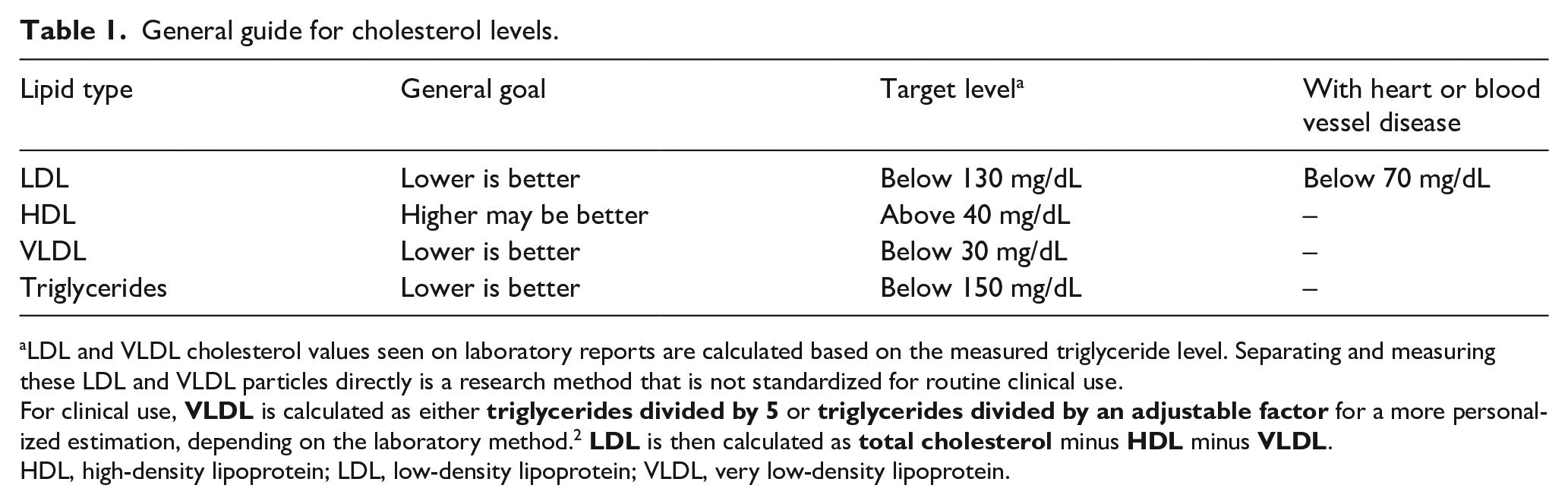
LDL and VLDL cholesterol values seen on laboratory reports are calculated based on the measured triglyceride level. Separating and measuring these LDL and VLDL particles directly is a research method that is not standardized for routine clinical use.
For clinical use,
HDL, high-density lipoprotein; LDL, low-density lipoprotein; VLDL, very low-density lipoprotein.
What causes cholesterol problems or dyslipidemia?
The major factors that determine lipid levels include genetics (family history), nutrition or diet, physical activity, body weight, and tobacco use. When lipid imbalance occurs together with certain other health problems, the overall risk of heart attack and stroke increases.
A genetic condition known as familial hypercholesterolemia (FH) can make it difficult for the body to clear extra LDL away, leading to very high LDL levels. Adults with FH generally have LDL levels above 190 mg/dL, and they are at high risk for atherosclerosis and cardiovascular disease if untreated. Because FH is inherited, it is a good idea to have family members screened when FH is suspected.
What are the health risks of having abnormal lipid levels? What factors can increase these risks?
Dyslipidemia (high LDL, high triglycerides, and/or low HDL) leads to fatty plaque build-up in the artery walls in a process called ‘atherosclerosis’, meaning thickening and hardening of the arteries (Figure 2). Because arteries carry blood to all parts of the body, including to the heart muscle itself, this cholesterol build-up and artery narrowing can lead to multiple health problems.
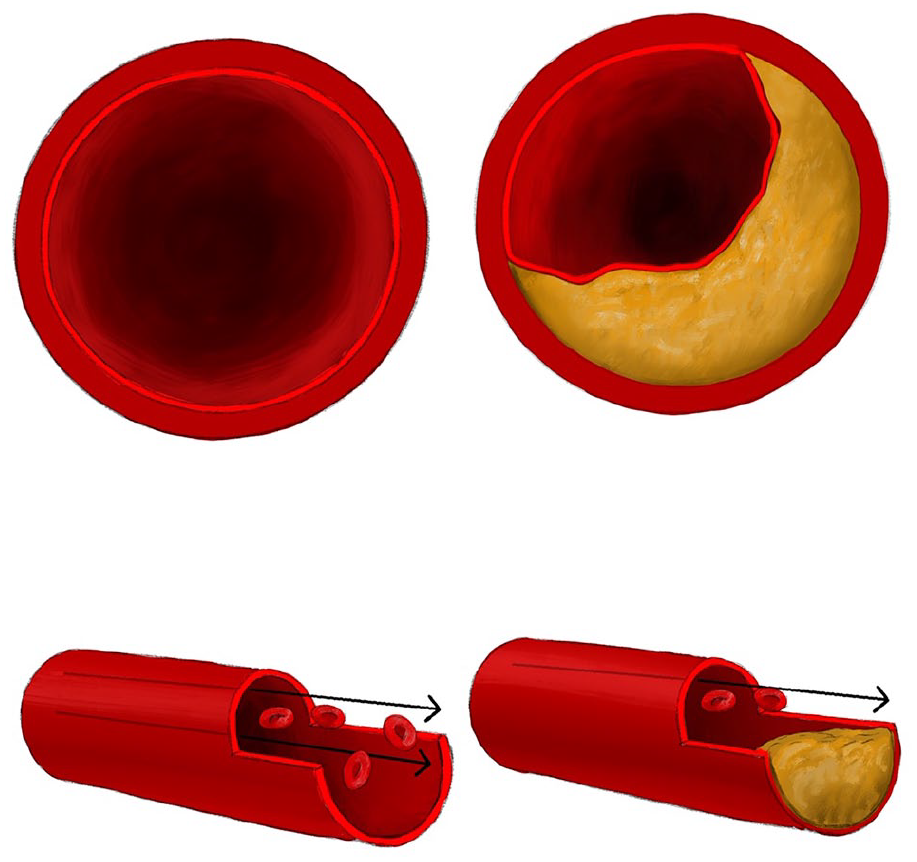
Atherosclerosis causes narrowing or blockages of the arteries, limiting blood flow. The artery on the left is normal, but the artery on the right is narrowed by plaque.
Atherosclerosis is the major cause of cardiovascular disease, including PAD (in the leg arteries); heart attacks (in the coronary arteries to the heart); and strokes (in the arteries to the brain).
Very high levels of triglycerides contribute to atherosclerosis and can also lead to pancreatitis (inflammation of the pancreas) or fatty liver.
Having diabetes, hypertension (high blood pressure), kidney disease, obesity, and/or tobacco use together with abnormal lipids (from any cause) will further increase the risk of cardiovascular disease such as heart attack or stroke.
What can I do to improve my lipid levels?
The foundation of lipid health and overall cardiovascular health is lifestyle, which includes good nutrition, regular exercise, and avoiding smoking. Following healthy habits can reduce the risk of cardiovascular disease, even in inherited lipid disorders. 3
Smoking contributes to abnormal lipid levels and is a major risk factor for cardiovascular disease. Quitting smoking is one of the best ways to improve cardiovascular health. Many resources are available to help with quitting, such as the Quitline (1-800-QUIT NOW) and www.smokefree.gov. Meeting with a health care provider to work on a quit plan is a good first step. To learn more about smoking cessation, read the Vascular Disease Patient Information Page on ‘Smoking Cessation’. 4
Nutrition is another key to managing lipids. Although the liver makes much of the circulating cholesterol, dietary changes can still make a big impact. Dietary changes are especially important when the triglycerides are high and for patients with diabetes.
Consuming fresh vegetables and fruits as about half of each plate, along with 100% whole grains and lean proteins is a good start. Choosing water or unsweetened beverages instead of sugary sodas or sports drinks is also helpful, as is replacing saturated fats from butter or coconut oil with unsaturated fats from olive oil. It is important to avoid excess sugar and to avoid packaged and processed foods, which are often high in saturated fats and sodium. The DASH (Dietary Approaches to Stop Hypertension) diet and Mediterranean diet are eating patterns that promote good cardiovascular health.
Exercising at a moderate intensity (brisk walking or jogging, for example) for at least 30 minutes each day is another important way to improve lipid levels and cardiovascular health. For more on exercise to improve cardiovascular health, read the Vascular Disease Patient Information Page on ‘Exercise as Medicine’. 5
When are medications needed?
Lifestyle improvements are important and are recommended for everyone; however, medications are also necessary for some patients with abnormal lipids to reduce the risk of cardiovascular disease, including heart attack and stroke.
The decision to start medications should be made together between a patient and a health care team, taking into consideration key risk factors such as diabetes, family history, lipid values, blood pressure, and existing heart or vascular disease. These and other risk factors can be used to calculate an estimated risk of heart attack or stroke in the next 10 years and over the course of a lifetime.
When risk is on the borderline, special blood tests or imaging (such as a non-invasive coronary artery calcium computed tomography (CT) scan) may help determine the potential benefit of starting a cholesterol medication.
What are the medication options?
The first-choice medications to treat LDL are called
If LDL cannot be controlled with lifestyle changes and a statin, or if statins cannot be used, a medication called
If additional LDL lowering is needed after trying lifestyle changes, statin therapy, and ezetimibe, a group of medications called
A newly US Food and Drug Administration (FDA)-approved medication,
There are currently no proven therapies that improve cardiovascular health outcomes by raising HDL.
To lower triglycerides,
Additional research is underway to develop new cholesterol therapies. In the future, some medications may be available that are taken just twice per year. Working with the health care team is the ideal way to determine whether medication is needed, and if so, which options are best.
What about natural supplements and alternative treatments?
The best natural treatment to improve abnormal lipids is to work toward a healthy lifestyle (nutrition, exercise, and not smoking).
Alcohol, and wine in particular, has been suggested as a ‘heart-healthy’ option, but is of unclear benefit, and the risks tend to outweigh the benefits when it comes to cholesterol. It is not recommended to begin consuming alcohol for the purpose of lowering cholesterol levels.
Over-the-counter supplements are not evaluated by the FDA with the same safety and efficacy standards as prescription medications. Supplements are generally of questionable benefit and inconsistent quality. Over-the-counter fish oil, omega-3 supplements, and red yeast rice have unfortunately not been shown to affect artery plaque or prevent cardiovascular events. Consuming nutrients through a healthy diet is a more reliable option.
When is clinical follow-up recommended? Do I need to fast (avoid eating) before having my cholesterol checked again?
The need for fasting depends on the lipid problems being monitored and the type of lab test available. Many clinical labs now use a newer calculation for LDL that may not require fasting before the test. In certain situations, such as with triglyceride disorders, it is still important to fast before a blood draw. Patients should be provided with instructions on whether fasting is needed before the blood test.
In general, laboratory follow-up within 4–12 weeks is recommended after starting, or adjusting, therapy for lipid problems.
Summary
Cholesterol and other lipids are key components of the cardiovascular risk profile. Lipids can be modified through lifestyle change and, when needed, through medications to reduce the risk of cardiovascular problems. Everyone can improve his or her lipid levels and cardiovascular health through good nutrition, daily exercise, and avoiding tobacco. It is important to keep track of lipid values and other risk factors, and to work with a physician and clinical team if abnormal lipid levels are identified.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Seth Martin – research support from the American Heart Association, Aetna Foundation, National Institutes of Health, the David and June Trone Family Foundation, and CASCADE FH; consultant to Akcea, Amgen, AstraZeneca, Esperion, Kaneka, Novo Nordisk, Quest Diagnostics, Sanofi, Regeneron, and REGENXBIO; inventor of a system to estimate LDL cholesterol levels (patent pending); and founder and equity holder in Corrie Health, which intends to further develop the platform. This arrangement has been reviewed and approved by the Johns Hopkins University in accordance with its conflict of interest policies. The other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.