
Abstract

Heated tobacco products (HTPs) might lead to negative side effects on the cardiovascular system. 1 An HTP is a hybrid between an e-cigarette and a combustible cigarette. It uses the energy of a battery to heat tobacco to temperatures between 250°C and 350°C and to evaporate the nicotine it contains.2,3 Although HTPs heat tobacco up to 350°C only, they generate aerosols containing nicotine as well as smoke, tar, and lower levels of harmful chemicals than conventional cigarettes.2,4 However, little is known about the effects of HTPs on the cardiovascular system, especially when using arterial stiffness as a marker for prognostic relevant side effects on the cardiovascular system. We and others recently showed that both conventional cigarettes and e-cigarettes containing nicotine induce significant effects on arterial stiffness.5–7 The purpose of the current study was to determine the acute effects of HTPs compared to e-cigarettes and conventional cigarettes on arterial stiffness.
Twenty active, healthy smokers (10 men and 10 women; 21.9 ± 2.6 years; 1 ± 1 py) were studied during and after smoking or vaping in a partly double-blinded randomized, cross-over trial with wash-out of at least 48 hours between visits. 7 During the screening, all participants were checked for inclusion criteria: (i) active smoking or vaping; (ii) no mental health disorders; (iii) no cardiovascular diseases; (iv) no thyroid disease; (v) non-diabetic; (vi) no abnormalities in physical examinations; (vii) no hypertension; and (viii) no hypercholesterolemia. Furthermore, female participants had to be using oral contraceptives to be included in the study. Participants were excluded if previously enrolled in any other kind of study and if they declared being strict non-smokers. Subjects provided written informed consent. The study was approved by the local ethics committee (AZ 15-171 and amendment) and registered at DRKS (German Clinical Trials Register: DRKS00012919).
The subjects had to abstain from alcohol and smoking/vaping for 24 hours prior to the measurements. After resting for 30 minutes, the subjects were followed up 2 hours after smoking or vaping. The four different study visits consisted of: (a) HTP 2.2 (IQOS, Philip & Morris; 0.5 mg nicotine); (b) a tobacco cigarette (Cig) (Marlboro Gold, Philip & Morris; 0.5 mg nicotine); (c) e-cigarette with nicotine (ECig(+)) (16 mg/mL, tobacco flavor); and (d) e-cigarette without nicotine (ECig(–)) (0 mg/mL, tobacco flavor) (both DIPSE, eGo-T CE4 vaporizer, third generation, 3.3 volts, 1.5 ohms, 7.26 watts). Visits (c) and (d) were blinded by a person not involved in the investigator’s team. Each subject had to vape the e-cigarette with a minimum of a puff every 30 seconds for 10 puffs, each lasting for 4 seconds. 8 Each smoking or heating session took a single cigarette or heet. Peripheral blood pressure was measured using a conventional blood pressure monitor (Omron MIT Elite Plus™, Omron, Kyoto, Japan), while central blood pressure and parameters of arterial stiffness were measured by Mobil-O-Graph™ (IEM, Stolberg, Germany) as previously described. 7 Differences between the groups were calculated by two-way repeated-measures analysis of variance (ANOVA) and a post hoc test was performed at p < 0.05.
Peripheral systolic blood pressure (SBP) (baseline 122.3 ± 8.8 mmHg) increased significantly within the Cig, ECig(+), and HTP groups by more than +3% (p < 0.05; Figure 1A). SBP returned to baseline after 60 minutes. Similar effects were observed for mean arterial pressure (MAP). Heart rate (HR) (baseline 70.0 ± 9.0 bpm) initially increased more than 9% in the Cig and HTP groups (p < 0.01; Figure 1B) and returned to baseline after 45 minutes. The four groups differed significantly from each other within the two-way repeated-measures ANOVA and post hoc test for at least 30 minutes for SBP, MAP, and HR (p < 0.05). The augmentation index, adjusted for a HR of 75 bpm (AIx75), significantly increased in the Cig group after 5 (p < 0.01), 10 (p < 0.05), and 15 minutes (p < 0.05) and in the HTP group after 5 minutes (p < 0.05; Figure 1C). After adjusting for sex, age, MAP, and HR, results remained significant (Box tests: p > 0.05; Levene tests: p < 0.05; multivariate tests – Wilks’ lambda: p < 0.05) for Cig and HTP. Calculated pulse wave velocity (PWV) showed a significant alteration after 15 minutes for the Cig group (p < 0.05; Figure 1D) and a trend for ECig(+) (p ≈ 0.072) and HTP (p ≈ 0.066) (Figure 1D), whereas no significant changes occurred within the ECig(–) group (p > 0.05; Figure 1D). The four groups did not differ significantly within the ANOVA for AIx75, except for PWV (p < 0.05). Further statistics demonstrated no significant differences between genders for peripheral or central hemodynamics or arterial stiffness.
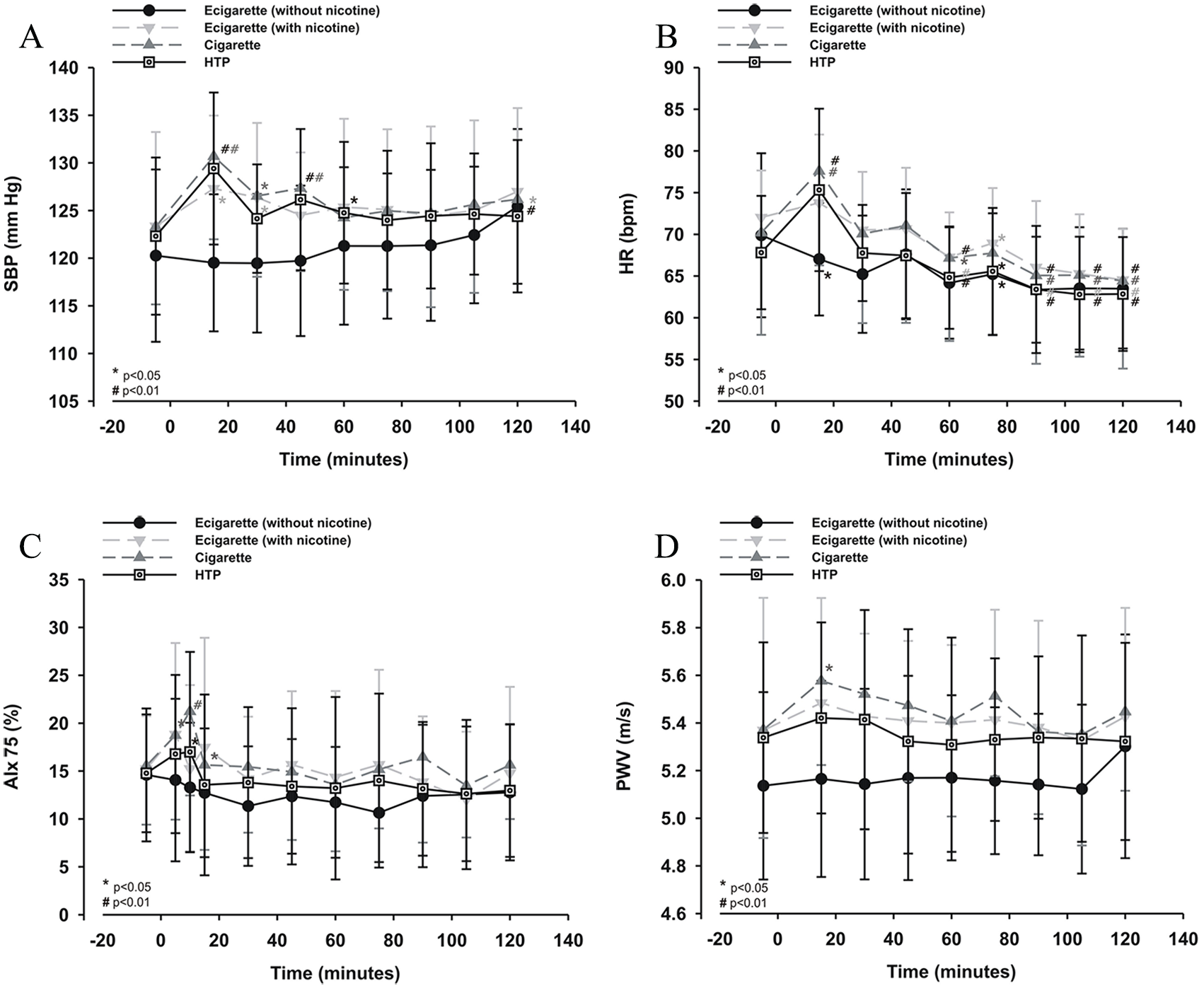
Peripheral blood pressure parameters were measured with the Omron MIT Elite Plus as well as with the Mobil-O-Graph. (A) Peripheral SBP – Omron; (B) HR – Omron; arterial stiffness – Mobil-O-Graph; (C) AIx75 – Mobil-O-Graph; (d) PWV – Mobil-O-Graph.
To the best of our knowledge, this is the first study in humans focusing on the acute effects of HTPs on arterial stiffness as a marker for cardiovascular events. Our data show acute changes in peripheral and central blood pressure. As expected, HTP, cigarettes, and ECig(+) lead to an increase of SBP, HR, and adjusted AIx75. As a further parameter of arterial stiffness, we demonstrate significant changes in PWV for conventional cigarettes, HTP, and ECig(+) showed trends. Our results indicate similar profiles for HTP and ECig(+), whereas conventional cigarettes show a trend towards numerically more pronounced changes.
These temporary alterations of hemodynamics and arterial stiffness are likely caused primarily by nicotine and further by an increase of local and circulating catecholamines. As a consequence, these changes can lead to an increase of sympathetic neuronal discharge-impaired nitric oxide production in the central nervous system. 6 Since Brossard et al. showed comparable levels of nicotine in serum after smoking or heating, the differences between HTPs and cigarettes on the one hand and e-cigarettes on the other hand, in our study, may be explained by the different pharmacokinetic profiles of nicotine delivered by the different cigarette types. 9 Although part of the change in arterial stiffness remains unexplained after calculating the statistics, any additional effects or chemicals do play a role. In line with these findings, the combination of nicotine and other harmful compounds in smoke and vape is one of the most likely explanations for the effects on the cardiovascular system 10 and lungs.3,11,12 These components might also trigger an endothelial dysfunction and an increase of arterial stiffness, which might trigger cardiovascular events. 13
The first limitation of our study is the number of subjects who were studied. Another limitation is that we did not explicitly ask the subjects about their sports or fitness levels in advance of this real life experiment, but established a resting period of 30 minutes in order to exclude acute effects in fitness or cycling. Furthermore, we looked for acute cardiovascular effects only. Therefore, long-term studies evaluating the chronic effects of heating compared to vaping or smoking on the cardiovascular system might be warranted.
In summary, we found a similar profile for heating, vaping or smoking a conventional cigarette on surrogate markers of increased cardiovascular risk.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed by Medizinische Klinik III, University Medical Center Schleswig-Holstein, Campus Lübeck and DZL (German Center for Lung Research). No funds were given by the tobacco industries.