
Abstract

We present a 35-year-old man who suffered from paroxysmal vertigo without recent history of head and neck trauma. Despite the finding of no significant stenosis in the right subclavian artery, there was a 20 mmHg blood pressure gradient, the mechanism of which could not be specifically identified. The remaining findings of the physical examination were all normal.
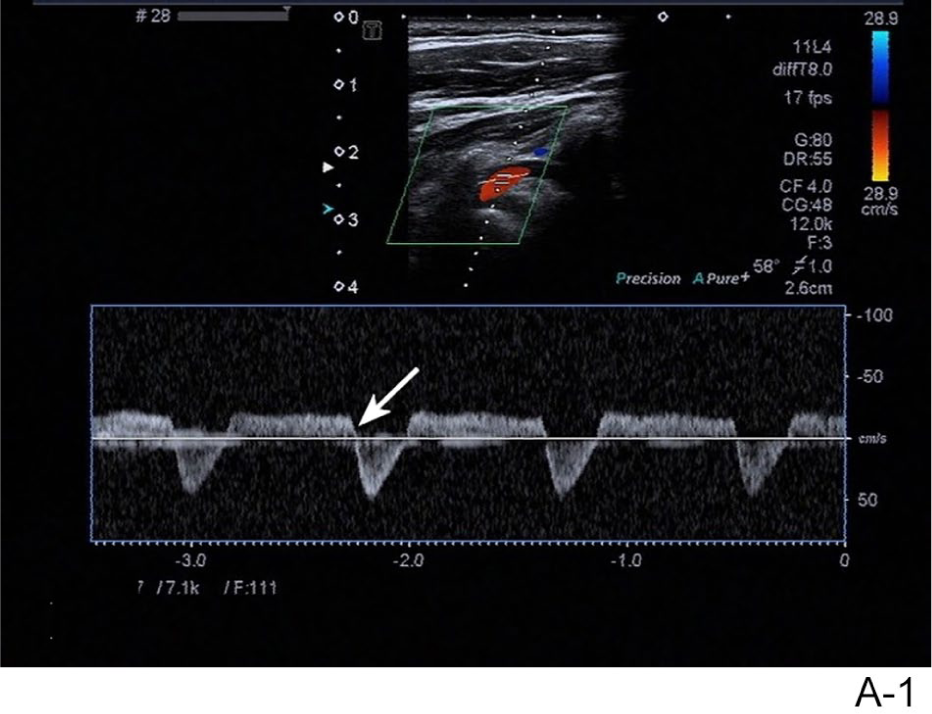
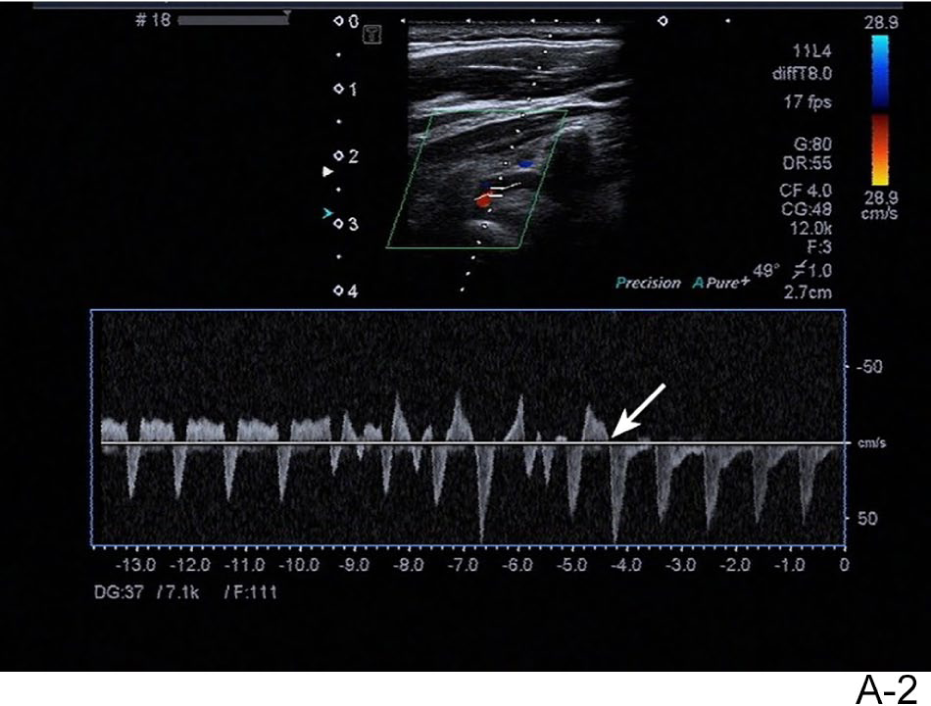
Transcranial Doppler (TCD) and duplex ultrasonography examination revealed retrograde and antegrade flow in the V4 and V2 segment of the vertebral artery (VA) (Panel A1: arrow). With fist-pumping, the right vertebral artery waveform transitioned from biphasic flow indicative of incomplete subclavian steal, to complete retrograde flow consistent with complete subclavian steal (Panel A2: arrow).
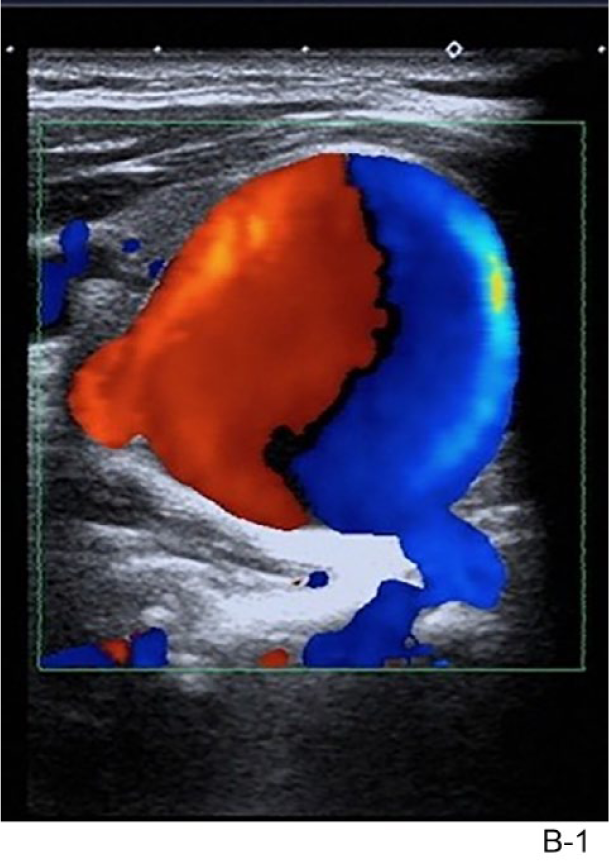
Beyond the innominate and proximal right subclavian arteries, which appeared normal, three separate aneurysms were visualized: a 2.5 × 2.3 cm aneurysm in the mid subclavian artery with a swirling blood flow pattern on color analysis (Panel B1); immediately distal to this, another 1.4 × 1.1 cm aneurysm was visualized with a swirling blood flow pattern on color analysis (Panel B2: arrow); and finally, a 1.1 × 0.9 cm aneurysm distal to a tortuous segment of the subclavian artery was visualized at the origin of the vertebral artery (Panel B3: arrow). Computed tomographic angiography (CTA) confirmed the findings on duplex ultrasound (Panel C).
Subclavian artery aneurysm (SAA) is a rare type of peripheral vascular aneurysm that manifests with various clinical symptoms. 1 There are few reports of subclavian steal syndrome (SSS) caused by SAA. Most often, the physiology of SSS involves a stenosis or occlusion on the subclavian artery proximal to the origin of the VA, which results in a pressure gradient between the bilateral vertebral arteries. 2
In our patient’s case, multiple SAA resulted in similar SSS phenomenon. The Bernoulli equation states that the potential energy of Newton’s liquid is inversely proportional to the kinetic energy. Thus, as the pressure inside the aneurysm decreases, the blood flow speed along the inner wall of the SAA will inevitably accelerate. This acceleration will reduce pressure at the vertebral artery opening (Venturi tube principle) and result in the aneurysm ‘stealing’ blood from the vertebrobasilar system, causing paroxysmal vertigo via vertebrobasilar insufficiency. Ultrasonography is a reliable method for the evaluation of the VA hemodynamics. 3
We suggest that SAA-induced SSS is an unnoticed cause of vertigo. Thus, clinicians treating young patients who suffer from vertebrobasilar insufficiency should consider low-pressure lesions in the subclavian artery as a possible cause, and consider duplex ultrasonography in the evaluation of these patients.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.