
Abstract

The left ventricular outflow tract (LVOT) velocity-time integral (VTI) is a key hemodynamic datum that is often obtained by transthoracic echocardiography. The stroke volume (SV) is calculated as the product of the LVOT VTI and the LVOT cross-sectional area (CSA); the product of the SV and the heart rate (HR) yields the cardiac output. Given the inaccuracies in obtaining the LVOT CSA, the LVOT VTI, which has been proved to be independent of the body surface area, is used as a surrogate of the SV index and cardiac index. 1 Yuriditsky and colleagues identify patients with pulmonary embolism (PE) with a worse prognosis using the LVOT VTI (or stroke distance). Their efforts are commendable, and their findings seem to open the door for reclassification of those patients in whom a poor outcome is not anticipated by traditional risk stratification methods. 2 However, one point deserves full consideration: how to measure the LVOT VTI in the right way. Wrong LVOT VTI measurements carry the risk of making wrong conclusions, both at the patient’s bedside and in research studies. Of note, one important mistake can be observed in the figure (Figure 1A and 1B) provided by the authors, 2 where there is an unacceptable angulation between the Doppler beam and LVOT, leading to underestimating the LVOT VTI (Figure 1).
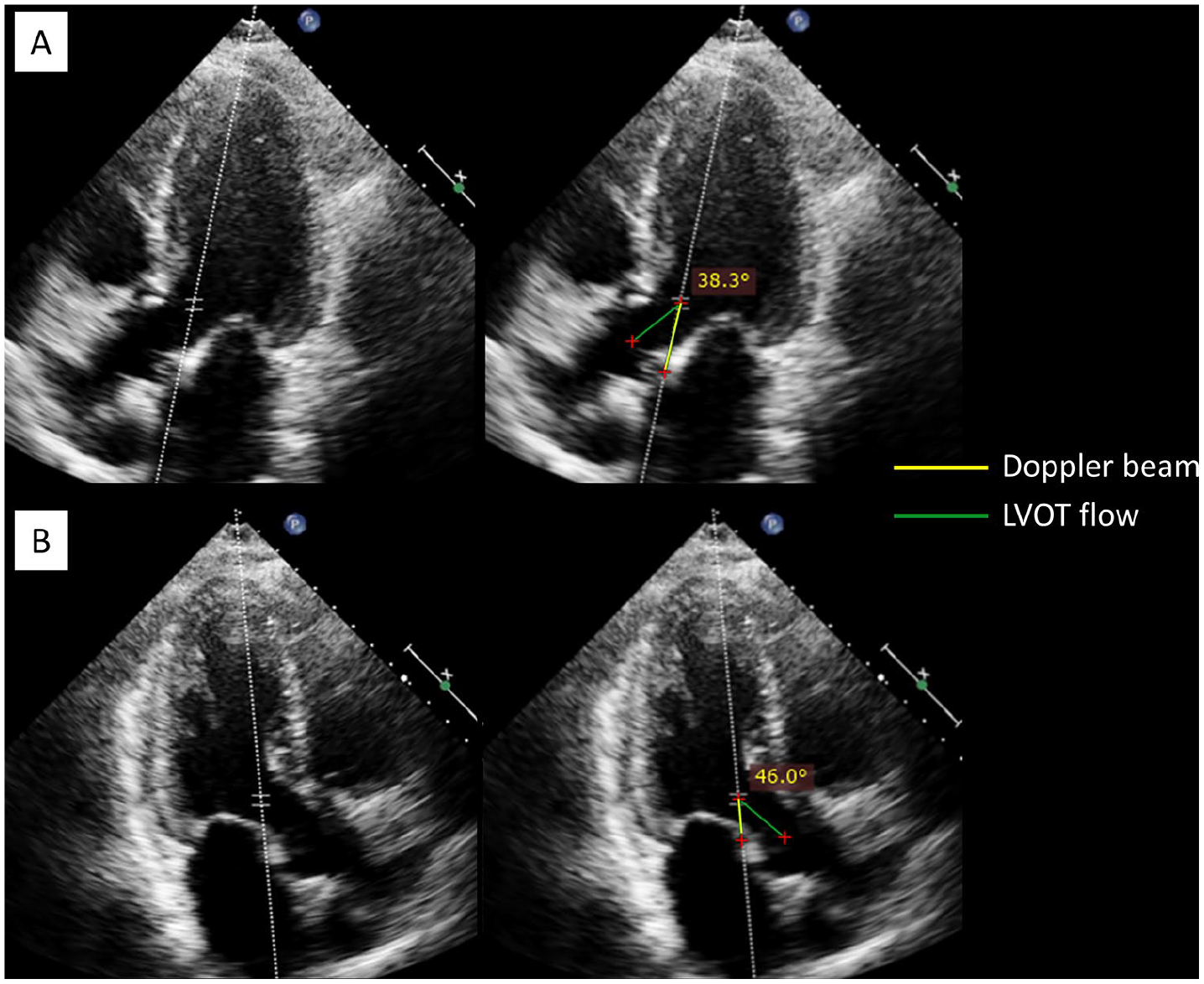
Unacceptable Doppler beam-flow angle for measuring the LVOT VTI from Yuriditsky et al. 2 A proper beam-flow angle must be maintained close to 0 degrees (< 20°) to obtain reliable VTI measurements. (A) Apical five-chamber view; (B) apical three-chamber view.
Based on the Doppler formula, the Doppler beam-flow angle is the most important variable for maximizing the Doppler shift and obtaining reliable velocity values. The LVOT VTI, or stroke distance, which is equal to the product of the mean LVOT velocity (cm/s) and LVOT flow duration (s), 3 is of course greatly affected by the beam-flow angle. According to this, the beam-flow angle must be maintained close to 0 degrees (< 20°) to get a reliable LVOT VTI. 4 Given that electronic angle correction is not recommended on echocardiography, 4 the only possible solution to align the beam and flow is by manipulating the probe and/or the patient position. Of note, obtaining an adequate beam-flow angle is particularly challenging in some patients with enlarged right heart chambers, such as in patients with acute cor pulmonale (e.g. central PE).
In conclusion, the LVOT VTI, as with any measurement taken by ultrasound, must be carefully performed to obtain reliable values, particularly in light that this datum may have an important impact in patient outcome and management, as indicated by Yuriditsky and colleagues.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.