
Abstract

Keywords
Loeys–Dietz syndrome (LDS) is an autosomal dominant connective tissue disorder characterized by a wide spectrum of skeletal, craniofacial, cutaneous, and vascular findings; the latter comprising cerebral, thoracic, and abdominal arterial aneurysms and/or dissections and severe arterial tortuosity.1,2 Diagnosis is confirmed by the identification of a heterozygous pathogenic variant in one of several genes directly influencing the transforming growth factor beta signaling pathway. 3 Wide phenotypic variability has been reported in patients with LDS, even among individuals belonging to the same family, who share the same pathogenic variant.2–4
Prevalence of cerebral aneurysm (CA) in patients with LDS has been reported to be 10–32%,1,5 but no data are available on potential risk factors for the development of CA in this patient population. The aim of this study was to investigate the relationship between CA and the extracranial vascular manifestations characteristic of LDS, as well as the influence of demographic and clinical features.
We retrospectively reviewed the clinical records and imaging studies of all patients with genetically confirmed LDS (n = 40) that were referred until May 2019 to the hub center for heritable connective tissue disorders of the University of Bologna (Italy).
We included in this study all patients (n = 36) for whom at least one imaging study of the intracranial arterial system, either magnetic resonance angiography (MRA) or computed tomography angiography (CTA), was available. In accordance with current guidelines, at our institution all patients diagnosed with LDS undergo full vascular imaging every 2 years. The patients who were excluded (n = 4) had not yet undergone a brain imaging study due to the very recent diagnosis of LDS.
Brain imaging studies were independently reviewed by two experienced neuroradiologists (LF and LS) who were blinded to the concurrence of extracranial vascular pathology.
Additionally, the vertebral tortuosity index (VTI) was calculated from 3D reconstruction of either CTA or MRA of the neck, following the protocol described by Morris et al. 6 using the formula: [(center-line distance) / (straight-line distance) – 1] ×100. Vessel analysis was performed with IntelliSpace Portal 8.0 software (Philips Medical Systems, Best, The Netherlands). Center-line distance and straight-line distance were calculated from the origin of the vertebral artery to a point proximal to the vertebral artery bend at the level of C2. The VTI of the most tortuous vertebral artery was assigned to each patient.
This study was approved by the institutional review board. Informed consent from all patients or parents/legal guardians for children was obtained.
A preliminary analysis of the association between presence of CA and explanatory variables was performed with Fisher’s exact test for categorical variables and the Wilcoxon rank-sum test for numerical variables. At multivariate analysis, odds ratio (OR) and 95% CI were estimated with a logistic regression model including variables with p < 0.1 on univariate analysis. All tests were two-sided, and p < 0.05 was considered statistically significant. Statistical analysis was performed using R version 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria).
Of the 36 patients included in this study (Table 1), 18 (50%) were probands while the others were identified through family screening. Ten patients presented de novo mutations and the remaining 26 belonged to eight families (Table 2). Median age was 40.5 years and nine patients (25%) were < 16 years old. Hypertelorism was found in 10 patients (27.8%), bifid uvula in nine (25%), and cleft palate in two (5.6%). The most frequent skeletal anomaly was pectus deformity (n = 16, 44.4%), followed by kyphoscoliosis (n = 14, 38.9%) and clubfoot (n = 3, 8.3%). Translucent skin was reported in 27 patients (75%) and osteoarthritis in 10 (27.8%).
Comparison of demographic and clinical characteristics between patients with CA and controls; results of the univariate and multivariate analysis.
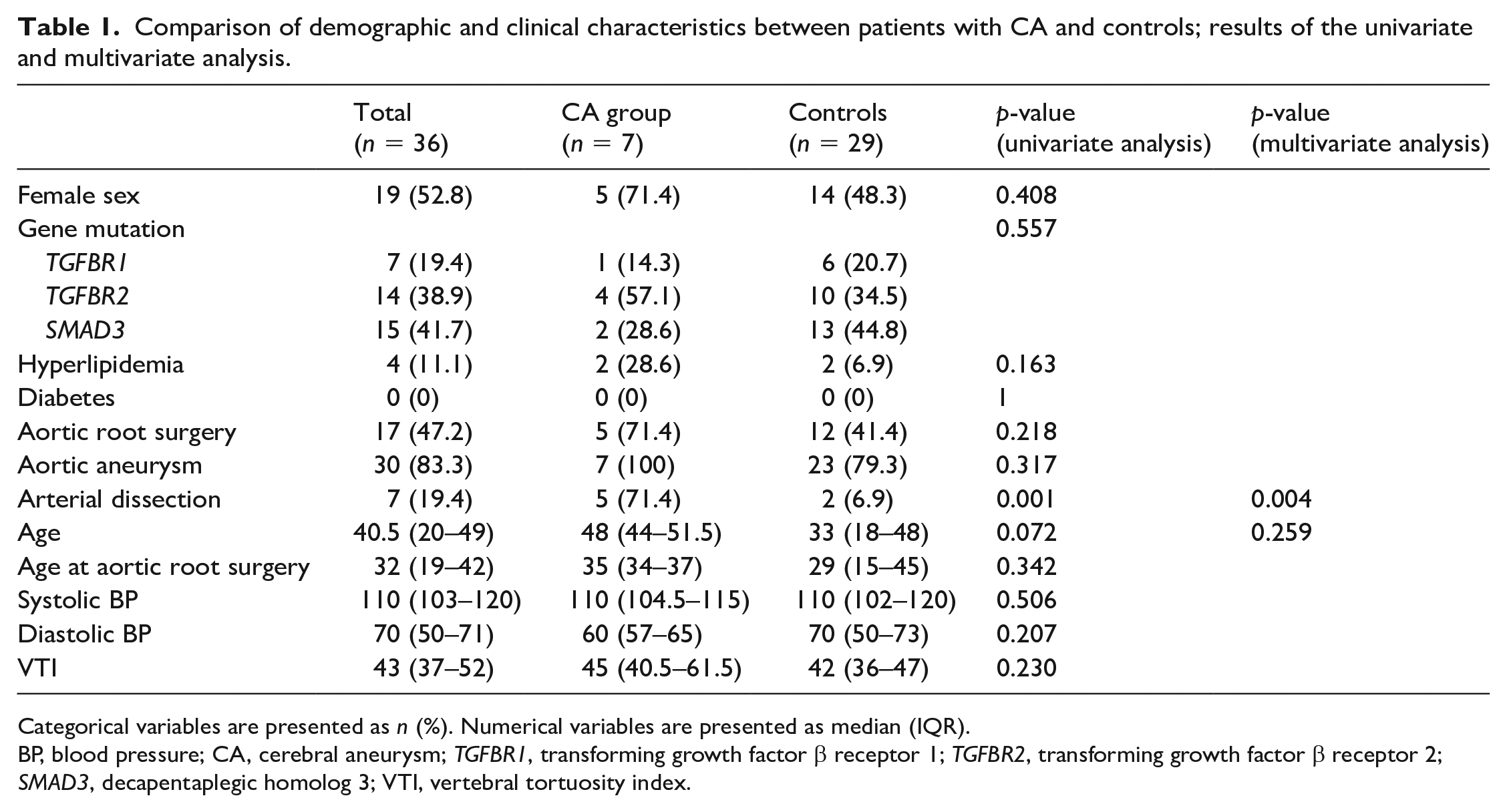
Categorical variables are presented as n (%). Numerical variables are presented as median (IQR).
BP, blood pressure; CA, cerebral aneurysm; TGFBR1, transforming growth factor β receptor 1; TGFBR2, transforming growth factor β receptor 2; SMAD3, decapentaplegic homolog 3; VTI, vertebral tortuosity index.
Mutations identified in the 18 probands.

SMAD3, decapentaplegic homolog 3; TGFBR1, transforming growth factor β receptor 1; TGFBR2, transforming growth factor β receptor 2.
In accordance with current guidelines,2,3 all patients were treated with antihypertensive medications. In 33 patients (91.7%), angiotensin II receptor blockers were used either alone (n = 20, 55.6%) or in combination with beta-blockers (n = 13, 36.1%), while in three patients (8.3%) only beta-blockers were employed.
Seven patients (19.4%) harbored at least one CA, confirming the previously reported high prevalence of this cerebrovascular pathology among patients with LDS.5,7 In one patient (2.8%), two aneurysms were found. The average CA diameter was 3.6 mm (range 2–5 mm). No patients presented with subarachnoid hemorrhage during an average follow-up period of 7 years.
Arterial dissection was reported in seven patients (19.4%). In three of them (8.3%) the aorta was affected (one Stanford type B and two Stanford type A dissections), three patients (8.3%) presented with coronary artery dissection, and one (2.8%) with dissection of the cervical internal carotid artery.
Arterial dissection was found in five patients (71.4%) in the CA group and in two patients (6.9%) among controls (Table 1). Univariate analysis showed a significant association between CA and extracranial arterial dissection (p = 0.001), which was confirmed by the multivariate model, including arterial dissection and age as explanatory variables (OR 26.39, 95% CI 2.88–241).
Two of the five patients with both arterial dissection and CA presented with arterial dissection after the diagnosis of CA. In the remaining three patients, the first brain imaging study was carried out between 2 and 7 years after arterial dissection, therefore it was not possible to determine whether aneurysm formation preceded arterial dissection.
Previous studies demonstrated elastic fiber fragmentation in the aortic wall of patients with LDS as well as in CA specimens of patients without a known connective tissue disorder.8,9 The presence of CA in patients with LDS may indicate a phenotype with more severe vessel wall involvement, which would also explain the higher prevalence of arterial dissection in this group of patients.
After evaluation by a multidisciplinary team, including neuroradiologists, neurosurgeons, and cardiologists, two of the seven patients with CA underwent elective aneurysm treatment: one via endovascular coiling, the other by surgical clipping. In both instances a durable result was achieved, without any complications.
All patients demonstrated severe tortuosity of the intracranial arteries (determined by subjective assessment), confirming previous studies.1,7 The median VTI in our patient population was 43, which was similar to the data reported by Morris et al. 6 in patients with LDS. No significant difference in VTI was found between the CA group and controls (Table 1). Although the median VTI was higher in patients with arterial dissection (45, IQR = 42.5–61.5) compared to patients without acute vascular events (42, IQR = 36–47), this difference was not significant (p = 0.167).
While increased vertebral arterial tortuosity has been reported as a marker of adverse aortic outcome, 6 the implications for increased tortuosity of the cerebral arterial system has not yet been elucidated.
The present study has some limitations, including its retrospective nature and the small number of enrolled patients. Additionally, the diagnosis of CA was based on brain MRA or CTA, which may make it difficult to diagnose very small aneurysms.
This is the first study investigating the association between CA and extracranial vascular manifestations in patients with LDS. We confirmed a high prevalence of CA in this patient population and found a significant association between this cerebrovascular pathology and extracranial arterial dissection. The discovery of a CA at brain imaging screening may therefore suggest the need for closer monitoring of these patients due to the higher risk of severe extracranial vascular events. While this is one of the largest cohorts of patients with LDS reported in the literature, our findings need to be confirmed in larger prospective studies which should include multiple centers in order to enroll a greater number of patients with this rare connective tissue disorder.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.