
Abstract
Achenbach syndrome (paroxysmal finger hematoma) refers to a condition in which a patient exhibits episodic pain and swelling in one or more digits along with the subsequent appearance of a hematoma on the palmar side of the proximal phalanges. Achenbach syndrome is a benign condition of unknown etiology in which prodromal symptoms, such as pain, tingling, and itching, may occur from minutes to hours before the color change appears. The subdermal bleeding usually stops spontaneously or after local pressure is applied. The color changes usually disappear within a few days, without permanent sequelae. The diagnosis of Achenbach syndrome is based strictly on its clinical features because the results of all routine investigations are usually normal. Physicians should become aware of this condition in order to advise their patients about its benign prognosis and to avoid unnecessary testing.
Continuing medical education (CME) credits and maintenance of certification (MOC) points are available for reading this article. This opportunity is made possible through a joint partnership with University of Virginia School of Medicine (UVASOM). For instructions, please visit the Society for Vascular Medicine’s website at
The University of Virginia School of Medicine (UVASOM) is accredited by the ACCME to provide continuing medical education for physicians. UVASOM designates this journal-based CME activity for a maximum of one AMA PRA Category 1 Credit™. Participants should claim only the credit commensurate with the extent of their participation in the activity. UVASOM, as an accredited provider, awards 1 hour of participation (consistent with the one AMA PRA Category 1 Credit™) to participants who successfully complete this educational activity. Successful completion of this CME activity, which includes participation in the evaluation component, enables the participant to earn up to one MOC II point in the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) program. It is the CME provider’s responsibility to submit participant completion information to ACCME for the purpose of granting ABIM MOC II credit. UVASOM maintains a record of participation for 6 years.
The faculty, staff and planning committee of the University of Virginia Office of Continuing Medical Education have no financial affiliations to disclose. The CME planning committee disclosed the following: Heather Gornik is supported by CVR Global and receives intellectual property rights from Summit Doppler Systems, Inc. and intellectual property rights and stock/ownership from FlexLife Health. Aditya Sharma is supported by National Institute of Health Sciences, AstraZeneca, and Biomet Biologics. Geoff Barnes is supported by Pfizer/Bristol-Myers Squibb (BMS), Blue Cross Blue Shield of Michigan, and the National Heart, Lung, and Blood Institute and serves as a consultant for Pfizer/BMS, Janssen, and Portola. Valerie Clark has no financial affiliations to disclose. The authors disclosed no financial relationship or interest with any proprietary entity producing healthcare goods or services.
Participants are expected to download and read the article, then complete the CME evaluation and MOC post-test questions with an 80% score or higher to receive credit. The post-test is available online from
Introduction
Many different pathological conditions present with color changes in the fingers. Recognizing these conditions is of great medical interest because they can harbor potentially serious underlying diseases. 1 A paroxysmal finger hematoma, which is also described as a spontaneous hematoma or Achenbach syndrome, refers to a condition in which the patient presents with episodic pain and swelling in one or more digits, with the subsequent appearance of a hematoma on the palmar aspect of the proximal phalanges without a history of prior trauma (Figure 1). 2 The first recorded description of this syndrome dates back to 1958 when the German doctor Walter Achenbach reported a condition that he called ‘paroxysmal hand hematoma’ or ‘finger apoplexy’. In his original work, he presented six cases of women who had experienced recurrent attacks of acute onset pain on the palmar side of one or more digits, followed by blue discoloration. 3 This condition has been ignored by most medical textbooks, and fewer than 100 cases have been reported in the medical literature. 4

An 81-year-old woman presented with sudden pain and bruising on the palmar aspect of the third finger of her right hand, which appeared after manually washing clothes. The pain and discoloration resolved spontaneously in the next 3 days. Notice the lack of distal phalanx involvement.
Pathophysiology and clinical characteristics
Achenbach syndrome is a benign condition of unknown etiology. 5 The cause of this spontaneous acute ‘blue finger’ syndrome is unknown, but it has been speculated that the mechanism involves subcutaneous bruising. 6 It is presumed that the bleeding is due to venous as opposed to arterial or arteriolar hemorrhaging. 7 Some arteriographic observations have revealed that the digital blood flow is significantly reduced in these patients. 2 In some cases, a reduction in the capillary resistance is observed using capillaroscopy; however, these changes are unlikely to be the cause, but rather the consequence, of blood infiltrating the tissues. 8
Prodromal symptoms, such as pain, tingling, and itching, may occur from minutes to hours before the color change appears 9 ; however, the subdermal bleeding usually stops spontaneously or after local pressure is applied, and the coloration changes usually disappear within 3–6 days. Interestingly, the lesions usually disappear without going through the typical stages of ecchymosis resorption. 7 Moreover, the distal phalanges and the nail bed are not involved, in contrast to what has been observed previously in ischemic finger diseases. 5 Overall, the course of this condition is benign, and the symptoms usually resolve without permanent sequelae. 10
Summary of previous literature
A summary of previous published literature regarding Achenbach syndrome is shown in Table 1. As part of a study of Raynaud’s phenomenon conducted in three geographic areas of France, 802 patients (548 women) between 18 and 84 years old were queried about symptoms that were suggestive of paroxysmal finger hematomas. 5 This study showed that 71 patients were diagnosed with Achenbach syndrome, with a prevalence of 12.4% and 1.2% among women and men, respectively. The average age at presentation was 48 years old, and the recurrence frequency was 1.2 times per year. The third finger was affected most frequently, followed by the second, but any of the fingers can be affected. The right hand was affected most frequently, with predominant involvement of the volar aspect. Nearly all of the patients reported pain and ecchymosis, and the average symptom duration was 3 days. 6 No relationships have been found with regard to body mass index, educational level, marital status, skilled work, occupational exposure to vibratory tools, or trauma (Table 1). 5
Summary of previous literature.
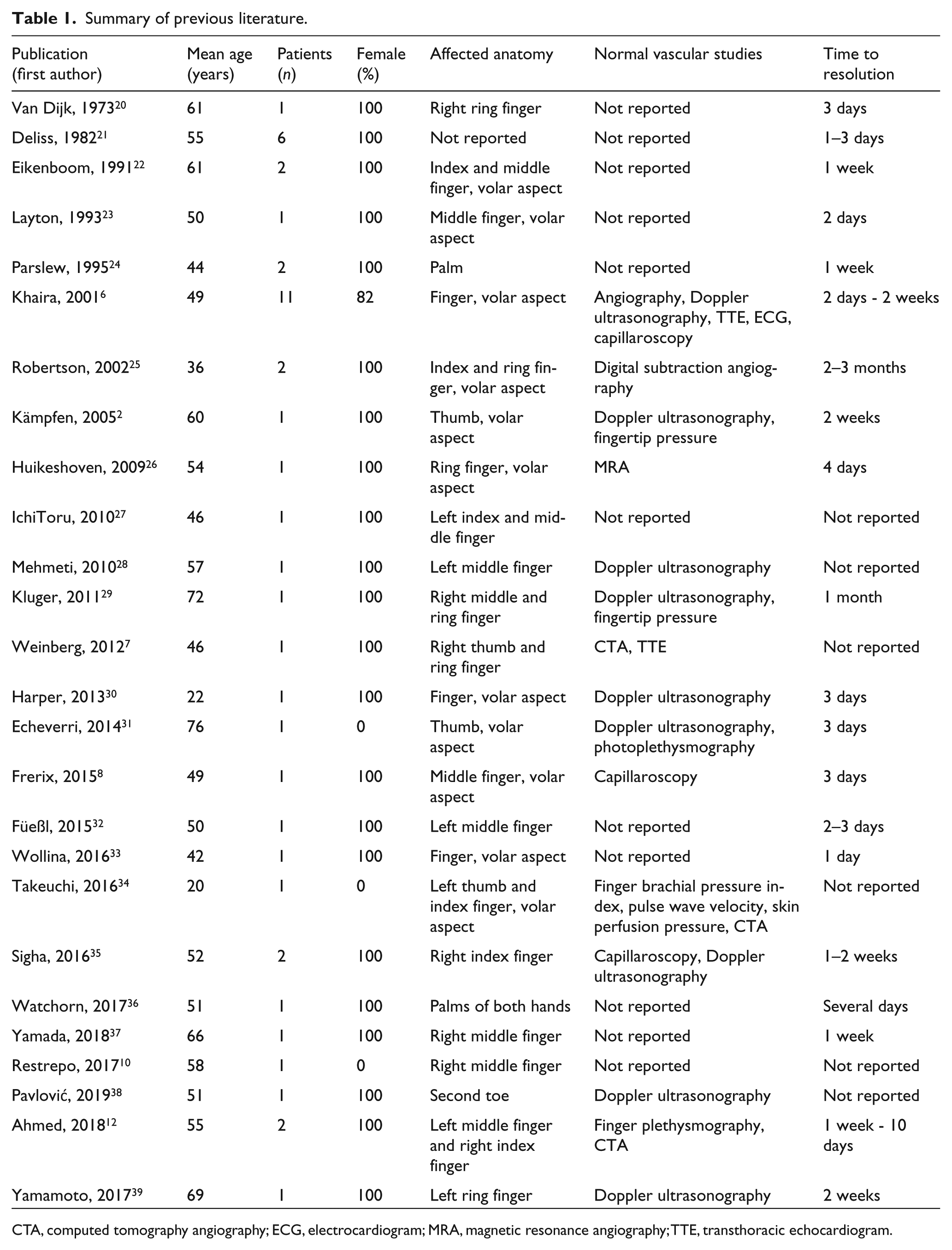
CTA, computed tomography angiography; ECG, electrocardiogram; MRA, magnetic resonance angiography; TTE, transthoracic echocardiogram.
In a systematic review of 46 patients diagnosed with Achenbach syndrome (median age 50 years, 43 females), the hands were the most commonly affected anatomical site, with 38 of the 46 patients reporting symptoms or signs on one or more of their fingers. 10 Pain was the most frequently reported symptom, and color changes were present in 40 of the 46 cases. The diagnostic test results, including Doppler ultrasonography, angiography, capillaroscopy, prothrombin time, thrombin time, C-reactive protein, erythrocyte sedimentation rate (ESR), total leukocyte count, platelet count, complete blood count, and immunological and biochemical profiles, were normal. In the few patients who underwent skin biopsies, the results were normal or they did not provide conclusive information (Table 1). 10
Diagnosis
The diagnosis of Achenbach syndrome is based strictly on the clinical features because the results of all the routine investigations, including Doppler examinations and biochemical studies, are usually normal. 9 Although it is rarely needed, nail bed capillaroscopy can be a useful exclusion test. It shows multiple hemorrhages, without any other alterations in the capillary morphology or blood flow. 4 Typically, the nail bed capillaries are not affected. 11 In 2018, Ahmed et al. reported the cases of two patients with Achenbach syndrome in whom finger plethysmography examinations were performed. As expected, normal finger pressures were documented in both cases. 12
Differential diagnosis
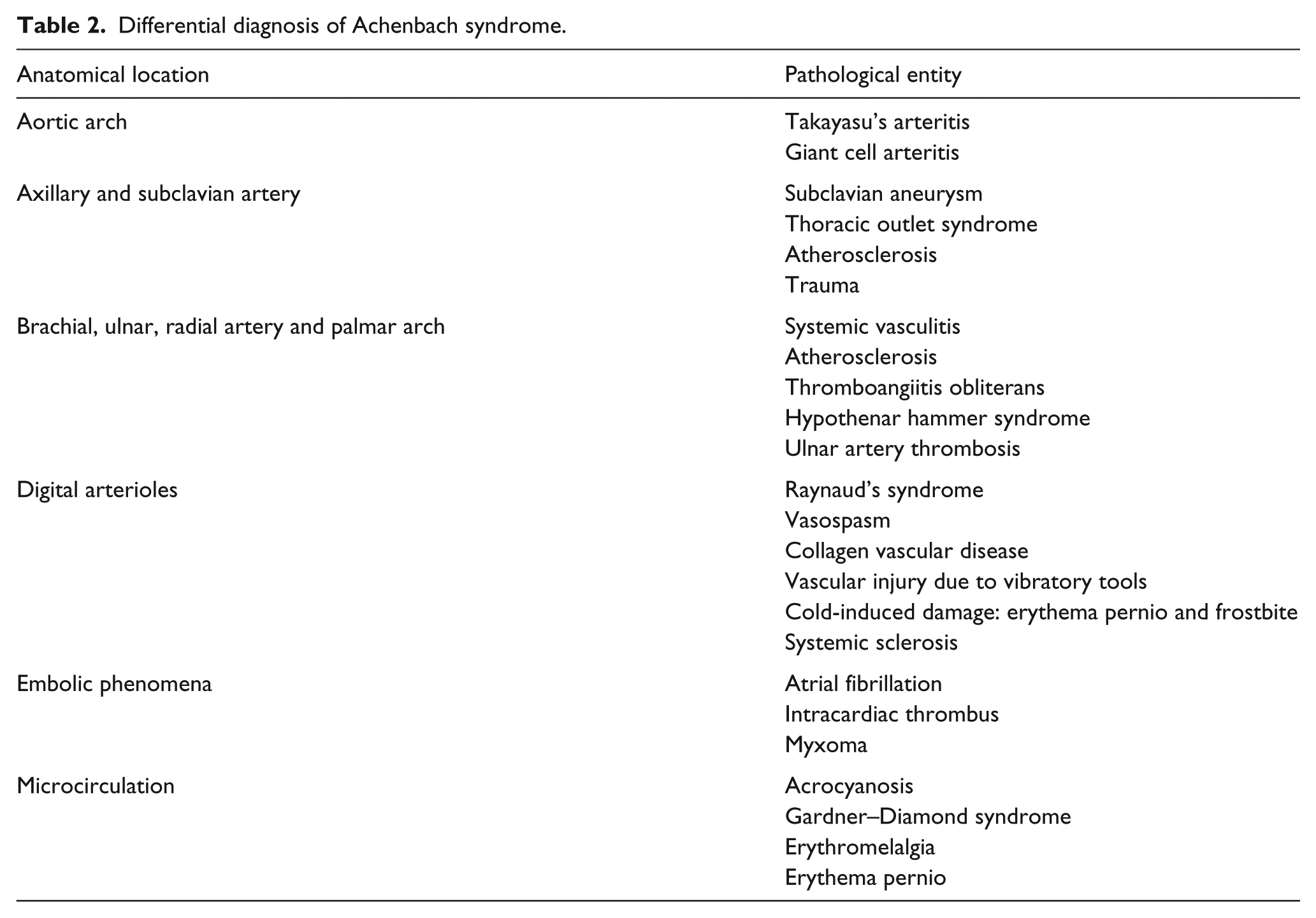
Acute upper extremity ischemia presents with symptoms similar to Achenbach syndrome, such as pain, cyanosis or pallor, paresthesia, and coldness. 13 In Achenbach syndrome, the digit(s) usually has a preserved temperature, and the involvement is predominantly in the volar aspect of the finger, without compromising the distal phalanx (Table 2). The radial and ulnar pulses and the Allen test results are usually normal in Achenbach syndrome cases, and these findings are the basis of a diagnostic algorithm proposed by Kordzadeh et al. 14 (Figure 2).
Differential diagnosis of Achenbach syndrome.
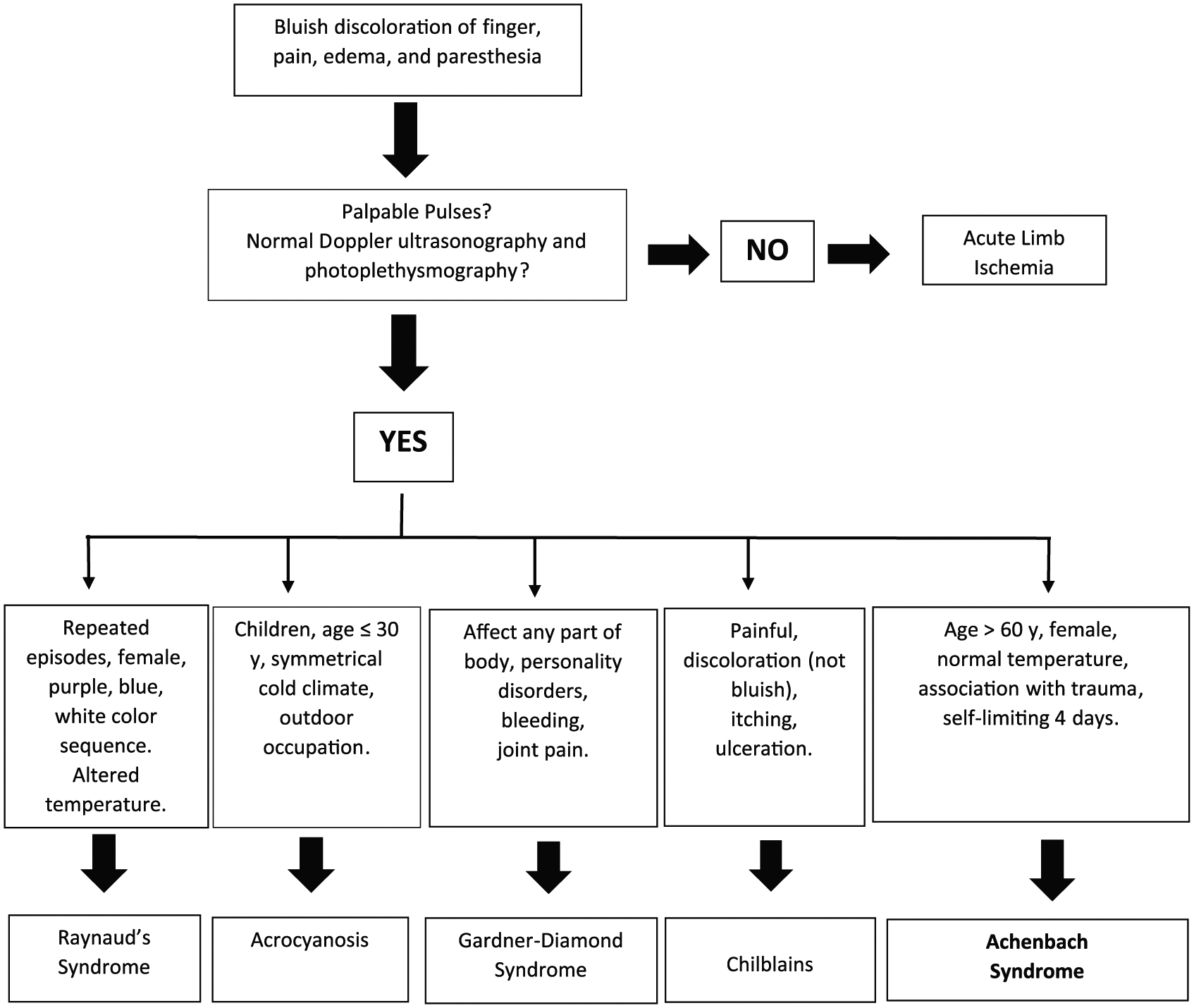
Achenbach syndrome algorithm.
In patients with upper extremity digital thromboses or arterial embolism, diagnostic work-up should include imaging studies to evaluate for the presence of ulcerated plaque in the aorta and subclavian artery or a subclavian artery aneurysm. Patients should be evaluated for underlying atrial fibrillation, and a possible cardiac source of embolization from an intracardiac thrombus or myxoma should also be excluded using echocardiography.
Systemic vasculitis with digital involvement should also be considered in the differential diagnosis. Unlike Achenbach syndrome, in systemic vasculitis there is intense digital pain with acral cyanosis and necrosis. The resolution of symptoms usually takes several weeks or months, and there is predominant involvement of the distal phalanges. Several laboratory features, such as elevated ESR and C-reactive protein levels and positivity for antinuclear antibodies, antineutrophil cytoplasmic antibodies, hepatitis C virus, or cryoglobulins, can be documented. 15
Thromboangiitis obliterans (Buerger’s disease) of the upper limbs is another disease that can simulate Achenbach syndrome. Thromboangiitis obliterans is almost always associated with tobacco exposure, and it results in ulceration and gangrene of the digits of the hands and feet. Some of these patients may present with migratory superficial thrombophlebitis. As in digital emboli, the involvement of the distal phalanges is prominent, with pain and necrosis, and there is marked improvement in the symptoms with tobacco abstention. 16
Primary or secondary Raynaud’s syndrome is another differential diagnosis; however, its presentation is more chronic and episodic. The attacks usually occur in relation to a decrease in the environmental temperature, and there is marked improvement with digital warming. 17 Raynaud’s syndrome involves one or several digits, and the coloration changes can go through several phases, from purple to white. In some patients, signs of immunological disease that may underlie the syndrome may be present (e.g. collagen vascular disease) and, in severe cases, ulceration and necrosis of the fingertips can be observed.
Acrocyanosis is a condition that should also be considered. It affects both sexes equally, including children, with an average onset age of 30 years old. Acrocyanosis is more common during cold weather and in patients with a low body mass index. The cyanosis is symmetrical, and it can involve the hands, fingers, nose, and ears. Usually, there is no pale phase, and it is not associated with ulceration or necrosis of the finger pads. 18
Gardner–Diamond syndrome, which is also called psychogenic purpura, was first described by Frank Gardner in 1955. 19 It is a rare condition characterized by the spontaneous development of painful edematous skin lesions, progressing to ecchymoses over the following 24 hours. Patients with Gardner-Diamond syndrome also present with ecchymotic lesions, pain, and digital edema. It occurs more frequently in women, and the etiology is largely unknown. However, in Gardner–Diamond syndrome, the cutaneous bleeding can affect any part of the body (hands, feet, trunk, and face), and it is often associated with personality disorders, nausea, and syncope. Severe stressors and emotional trauma precede the skin lesions. 19
Erythromelalgia presents with pain and edema in the toes or fingers, the coloration is usually erythematous or erythematous-violaceus, and the temperature is warm to the touch. The episodes are precipitated by limb warming, and pain relief can be observed when the digits are immersed in cold water.
Erythema pernio is an episodic disease related to cold exposure, with erythematous-violaceous papules on the digits, and it is usually accompanied by pruritus, pain, edema, and, occasionally, superficial ulcerations. The symptoms and lesions improve spontaneously or when the environmental temperature gets warmer. 6
Conclusions
Achenbach syndrome, although infrequently described in the literature, can cause a great deal of anxiety to the patient and the healthcare team due to the fear of a more severe condition that endangers the digits. Therefore, physicians should become aware of this condition in order to advise their patients about its benign prognosis and to avoid unnecessary testing.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.