
Abstract

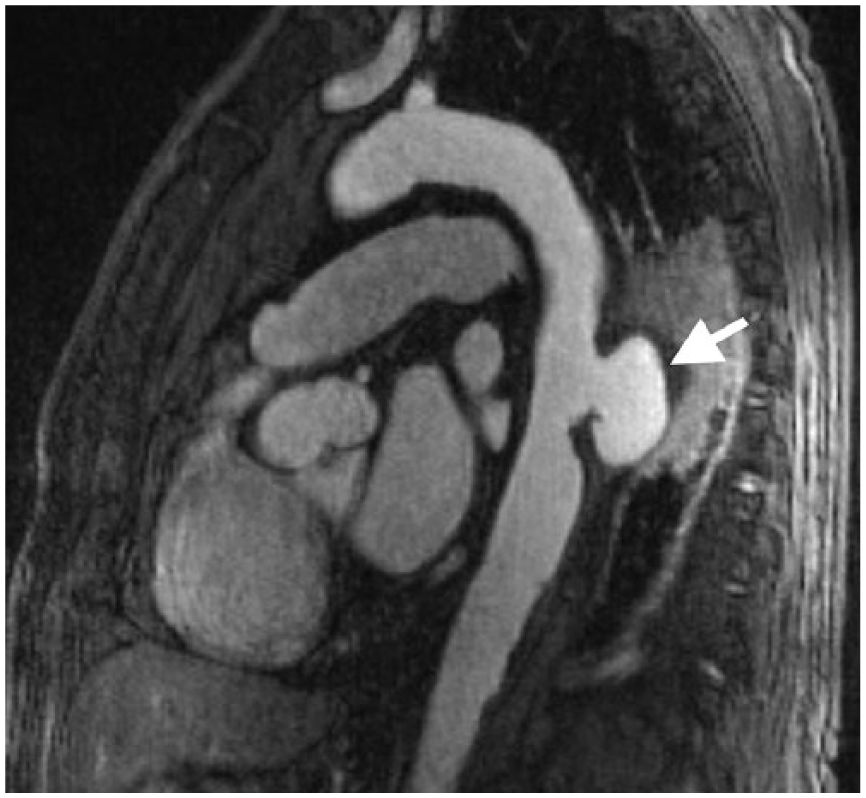
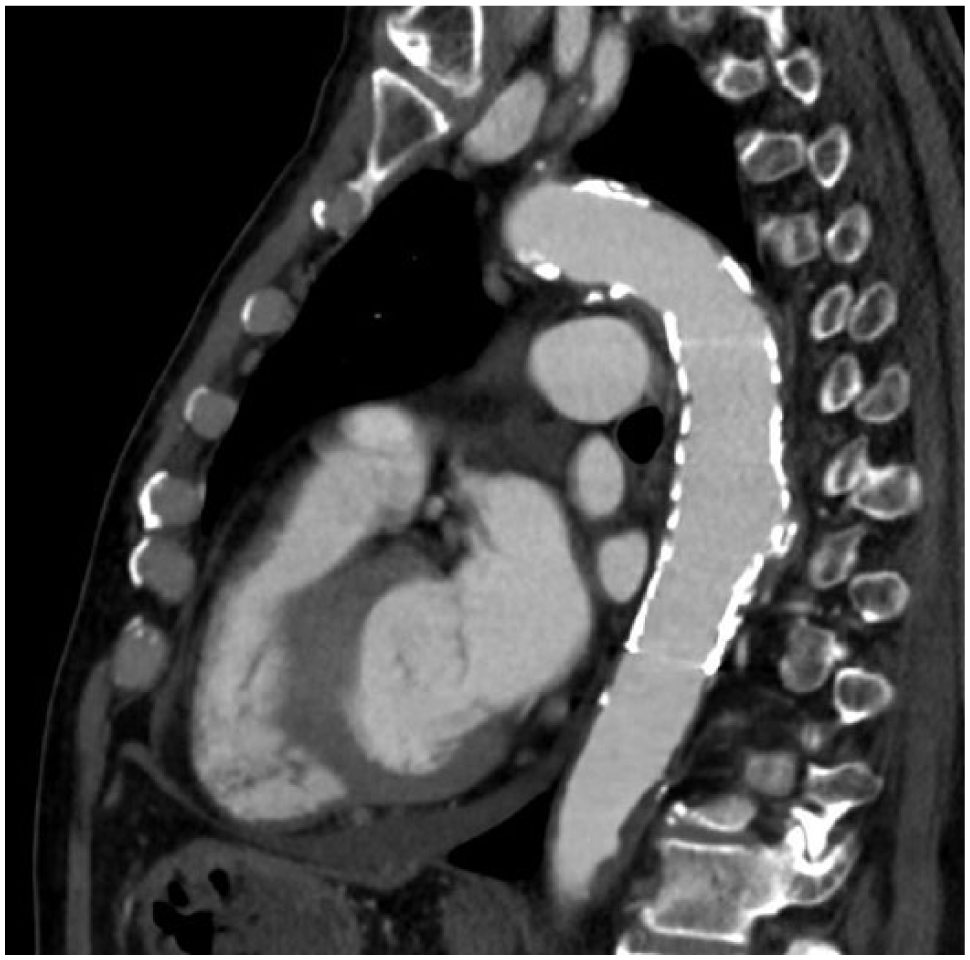
A 79-year-old man presented with chest pain radiating to the back. Acute aortic syndrome was suspected and a thoracic computed tomography angiography (CTA) was performed, demonstrating penetrating aortic ulcer (PAU) in the descending thoracic aorta with adjacent inflammatory tissue (arrow, Panel A). Blood cultures revealed methicillin-sensitive Staphylococcus aureus. Fluorine-18-fluorodeoxyglucose (18F-FDG) positron emission tomography/computed tomography (PET/CT) showed marked tracer uptake in the descending thoracic aortic wall and the adjacent lung parenchymal consolidation (arrow, Panel B). After intravenous antibiotic treatment and establishing the stability of PAU, the patient was transferred to a medical rehabilitation center. After 5 weeks, the patient re-presented with fever, anemia, and altered mental status. Gadolinium-enhanced magnetic resonance angiography (MRA) sagittal fat-saturated T1 images demonstrated an enlarging pseudoaneurysm at the left posterolateral aspect of the descending thoracic aorta with adjacent inflammatory tissue (arrow, Panel C). Given the comorbidities, the patient underwent endovascular repair with a 34 mm thoracic endoprosthesis, rather than open repair. Follow-up CTA with sagittal images confirmed adequacy of the endovascular repair (Panel D).
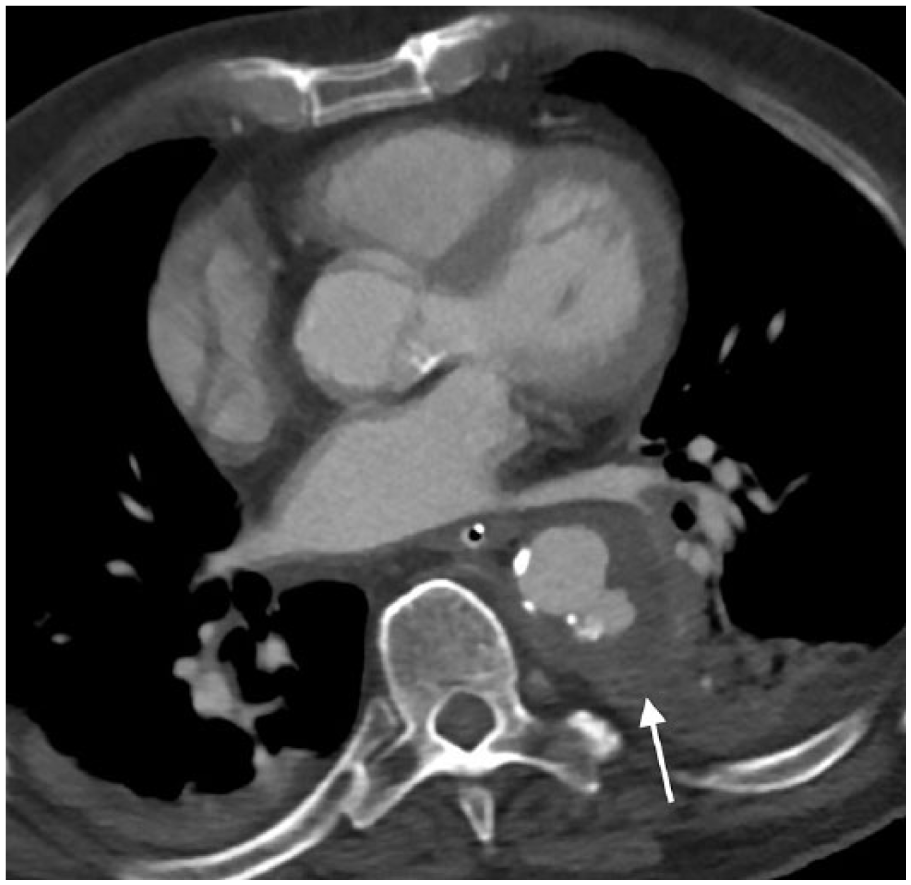
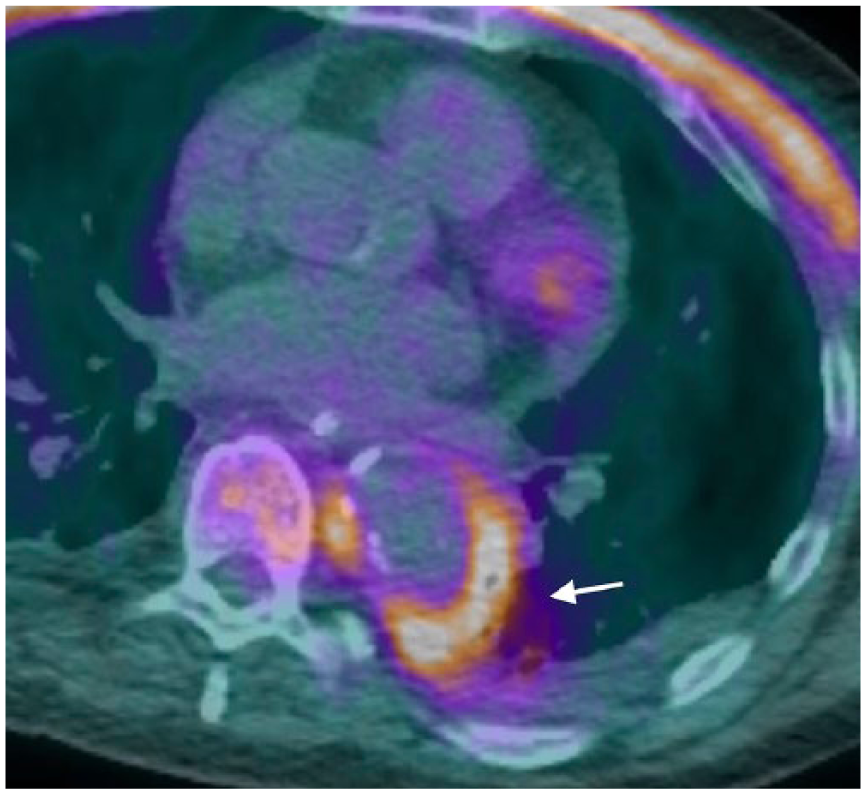
Mycotic aortic aneurysms (MAA) arise due to infection of the aortic wall and comprise only 0.7–2.6% of all aortic aneurysms. 1 Infectious aortitis weakens the vessel wall causing contained rupture and formation of a pseudoaneurysm. 1 MAA have been associated with infective endocarditis, unicuspid or bicuspid aortic valves, and infected prosthetic valves. 2 On cross-sectional imaging these aneurysms typically have a saccular rather than fusiform appearance. 2 A periaortic soft tissue mass is one of the most common imaging features 1 and may be confused with neoplasia, infectious lymphadenopathy or hematoma. 2 The presence of a hypoattenuating concentric rim in the aortic wall helps differentiate from non-infective aneurysms. 2 MAA demonstrate increased tracer uptake on 18F-FDG PET/CT in both the aneurysm wall and surrounding soft tissue. 1 MAA typically do not contain calcium in their walls and can enlarge rapidly over days to weeks. 3
Early diagnosis, delineation of the extent of the aneurysm, and assessment for associated complications are crucial as MAA are associated with high (15–50%) mortality. Treatment strategies consist of prolonged antibiotic therapy and surgical intervention, including extra-anatomic bypass and in situ graft placement. Endovascular stenting is a temporizing measure in critically ill patients. Risk of stent infection, endoleak due to malposition, and rupture remain with endovascular treatment.1,2 Although infrequently encountered, MAA can be rapidly progressive and fatal, highlighting the importance of early recognition.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.