
Abstract
There are limited contemporary data on readmission after revascularization for chronic mesenteric ischemia (CMI). This study aimed to determine the rates, reasons, predictors, and costs of 30-day readmission after endovascular or surgical revascularization for CMI. Patients with CMI discharged after endovascular or surgical revascularization during 2013 to 2014 were identified from the Nationwide Readmissions Database. The rates, reasons, length of stay, and costs of 30-day all-cause, non-elective, readmission were determined using weighted national estimates. Independent predictors of 30-day readmission were determined using hierarchical logistic regression. Among 4671 patients with CMI who underwent mesenteric revascularization, 19.5% were readmitted within 30 days after discharge at a median time of 10 days. More than 25% of readmissions were for cardiovascular or cerebrovascular conditions, most of which were for peripheral or visceral atherosclerosis and congestive heart failure. Independent predictors of 30-day readmission included non-elective index admission, chronic kidney disease (CKD), and discharge to home healthcare or to a skilled nursing facility. Revascularization modality did not independently predict readmission. In a nationwide, retrospective analysis of patients with CMI undergoing revascularization, approximately one in five were readmitted within 30 days. Predictors were largely non-modifiable and included non-elective index admission, CKD, and discharge disposition.
Keywords
Introduction
Mesenteric artery stenosis affects nearly 18% of adults over the age of 65; however, it is often asymptomatic. 1 Among patients who develop symptoms of chronic mesenteric ischemia (CMI), endovascular therapy (percutaneous transluminal angioplasty and stenting) and open surgery (endarterectomy or bypass grafting) carry Class I recommendations in multidisciplinary consensus guidelines. 2 Nevertheless, contemporary data from the United States (US) National Inpatient Sample 3 indicate that endovascular therapy is the dominant revascularization modality, and is associated with fewer in-hospital major adverse cardiovascular events, lower overall complications, shorter length of stay, and lower cost compared with surgery. To our knowledge, there are no published data on readmission following revascularization for CMI. We sought to determine the contemporary rates, reasons, predictors, and costs of 30-day readmissions following endovascular or surgical revascularization for CMI in the US.
Methods
Data source
The study was approved by the Rhode Island Hospital Institutional Review Board. Data were obtained from the 2013–2014 Nationwide Readmissions Database (NRD), collected by the Agency for Healthcare Research and Quality (AHRQ) as part of the Healthcare Cost and Utilization Project (HCUP). The NRD is the largest, publicly available database of all-payer inpatient stays that can be used to obtain national estimates of readmissions. 4 The NRD was created via HCUP’s State Inpatient Databases comprised from multiple states that are geographically dispersed and provides annual information on approximately 17 million unweighted (36 million weighted) discharges. Raw data from the national database are comprised of samples and therefore must be weighted to derive national estimates. Without weights being applied the derivation of data represents sample record counts, not national and/or regional estimates. Based on US Census Bureau data, the NRD accounts for approximately half of the US population and half of US hospitalizations. 4 The NRD utilizes unique patient linkage numbers to associate the same patient across multiple hospitalizations within a given state, while protecting the privacy of individual patients. However, patient linkage numbers do not track patients across calendar years.
Study population
Patients ⩾ 18 years of age with a primary diagnosis of CMI during the index hospitalization were identified using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) code 557.1 (n = 17,403). Patients were excluded if they: (1) were discharged during the month of December (n = 1483); (2) had an unknown discharge destination or left against medical advice (n = 150); (3) did not undergo endovascular or surgical revascularization during the hospitalization (n = 13,126); (4) were treated with both endovascular therapy and surgery during the index hospitalization or underwent a hybrid procedure (n = 50); (5) were diagnosed with acute mesenteric ischemia (n = 398); (6) underwent embolectomy (n = 10) during the index hospitalization; (7) died during the index hospitalization (n = 105); or (8) were readmitted within 30 days of a prior CMI revascularization hospitalization (n = 93). The final analytic cohort was comprised of 1988 (4671 weighted) index CMI hospitalizations (Figure 1).
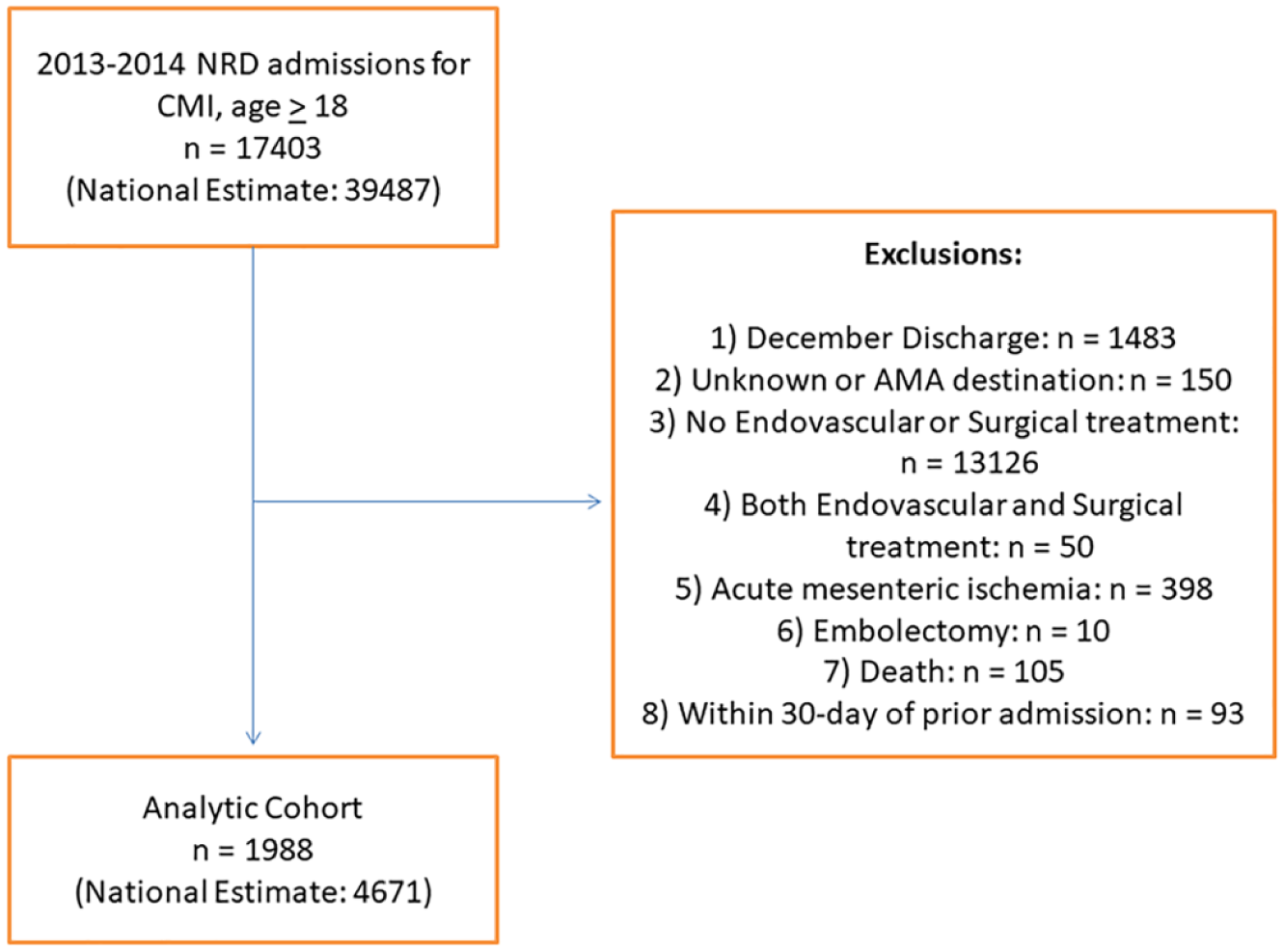
Patient inclusion and exclusion criteria. Flow chart highlighting selection of the study cohort with index CMI hospitalizations.
Patient and hospital characteristics
Data from HCUP variables on age, sex, insurance status, median household income, and associated medical comorbidities were extracted. Elixhauser Comorbidity Software was applied to identify congestive heart failure, valvular heart disease, pulmonary circulation disorders, peripheral vascular disease, chronic pulmonary disease, hypothyroidism, chronic kidney disease (CKD), hypertension, liver disease, non-bleeding peptic ulcers, collagen vascular disorders, coagulopathy, obesity, weight loss, alcohol/drug abuse, psychoses, and depression. ICD-9-CM and Clinical Classifications Software (CCS) coding were utilized to define history of smoking, diabetes mellitus, atrial fibrillation/flutter, coronary artery disease, prior myocardial infarction, and chronic blood loss anemia. ICD-9-CM and CCS codes used to define these variables are listed in Supplemental Table 1. CCS is a diagnosis and procedure categorization scheme that collapses multiple related ICD-9 codes into a smaller number of clinically meaningful classes that have been standardized and widely employed in previous analyses of diagnoses and procedures. 5 The Charlson Comorbidity Index was calculated.6,7
Index hospitalization complications, including acute myocardial infarction (AMI), other postoperative cardiac complications (cardiac complications not elsewhere classified, including cardiac arrest, arrhythmias, and cardiorespiratory or heart failure during and/or resulting from a procedure), stroke, postoperative peripheral vascular complications, and major bleeding (Supplemental Table 1), were included. A composite, index hospitalization major adverse cardiovascular and cerebrovascular events (MACCE), was defined as any of the following: AMI, other postoperative cardiac complications, stroke, postoperative peripheral vascular complications, or major bleeding. Postoperative peripheral vascular complications included venous thromboembolic and arterial complications following a procedure.
Outcomes
The primary outcome of interest was 30-day all-cause, non-elective, readmission. Transfer to another hospital or to a rehabilitation facility were not considered readmissions. The overall rate of and median time to readmission were calculated. If a patient had multiple readmissions within 30 days, only the first was included. The primary diagnosis for readmission was reviewed and used to designate the reason for readmission. Reasons for 30-day readmission were classified into clinically meaningful categories using CCS and ICD-9-CM diagnosis codes (Supplemental Table 2). Owing to the limited specificity of CCS codes 237 (Complication of device; implant or graft) and 238 (Complications of surgical procedures or medical care) as primary causes for readmission, we extracted the primary readmission ICD-9-CM diagnosis code for each patient with CCS code 237 or 238 listed as their primary readmission CCS code. Those patients were then categorized under a composite variable: treatment-related complications. Other outcomes of interest included median readmission length of stay (LOS) and median readmission hospital cost. Costs were adjusted for inflation, with 2017 serving as the index base. 8
Statistical analysis
National estimates were obtained using discharge weights provided by HCUP and using Proc Surveyfreq in SAS (SAS Institute Inc., Cary, NC, USA). Categorical variables are presented as frequencies and percentages and compared with chi-squared tests in unadjusted analyses. Continuous variables are presented as mean ± standard deviation or median with interquartile range (IQR) as appropriate, and compared using Student’s t-tests or Mann–Whitney U tests in unadjusted analyses.
Hierarchical logistic regression models were constructed to identify independent predictors of 30-day readmission. Model covariates included surgical revascularization [reference endovascular], non-elective index admission, female, age (per 10 years), metropolitan area > 1 million, Medicaid [reference private insurance], Medicare [reference private insurance], prior myocardial infarction, coronary artery disease, atrial fibrillation/flutter, congestive heart failure, hypertension, diabetes, CKD, coagulopathy, liver disease, chronic lung disease, smoking, drug abuse, obesity, hypothyroidism, anemia, depression, index hospitalization MACCE, discharge to home healthcare (HHC) [reference home], discharge to skilled nursing facility (SNF) [reference home], and Charlson Comorbidity Index > 2.
SAS 9.3 (SAS Institute Inc.) was used for all statistical analyses. A two-tailed p-value of < 0.05 was considered statistically significant. Odds ratios and 95% confidence intervals are utilized to present results from regression analyses.
Results
Patient and index hospitalization characteristics
Patient demographic and clinical characteristics according to readmission status appear in Table 1. In the overall cohort, the mean age was 71.4 ± 11.1 years and 70.6% were women. Approximately one in five patients overall underwent surgery as the mode of revascularization at index hospitalization. A total of 35% of the overall index hospital admissions were elective. There was a high prevalence of comorbidities, including coronary artery disease, peripheral vascular disease, diabetes, hypertension, atrial fibrillation/flutter, hypothyroidism, CKD, and anemia. In unadjusted analyses, while age and sex were similar among patients who were readmitted and those who were not, readmitted patients were more likely to have Medicare as their primary payer, diabetes, CKD, peripheral vascular disease, atrial fibrillation/flutter, congestive heart failure, liver disease, anemia, coagulopathy, have a higher Charlson score and were more likely to be discharged with home healthcare or to a skilled nursing facility. The rate of bowel resection was similar among endovascular and surgical groups (3% and 3.5%, respectively; p = 0.62). In contrast, readmitted patients were less likely to be smokers. The index hospital MACCE rate among re-admitted patients was higher compared to those not readmitted (17.5% vs 12.1%, p < 0.001), a finding that was driven by higher rates of AMI and postoperative peripheral vascular complications; rates of postoperative cardiac complications, stroke, and major bleeding did not differ between groups.
Baseline characteristics.
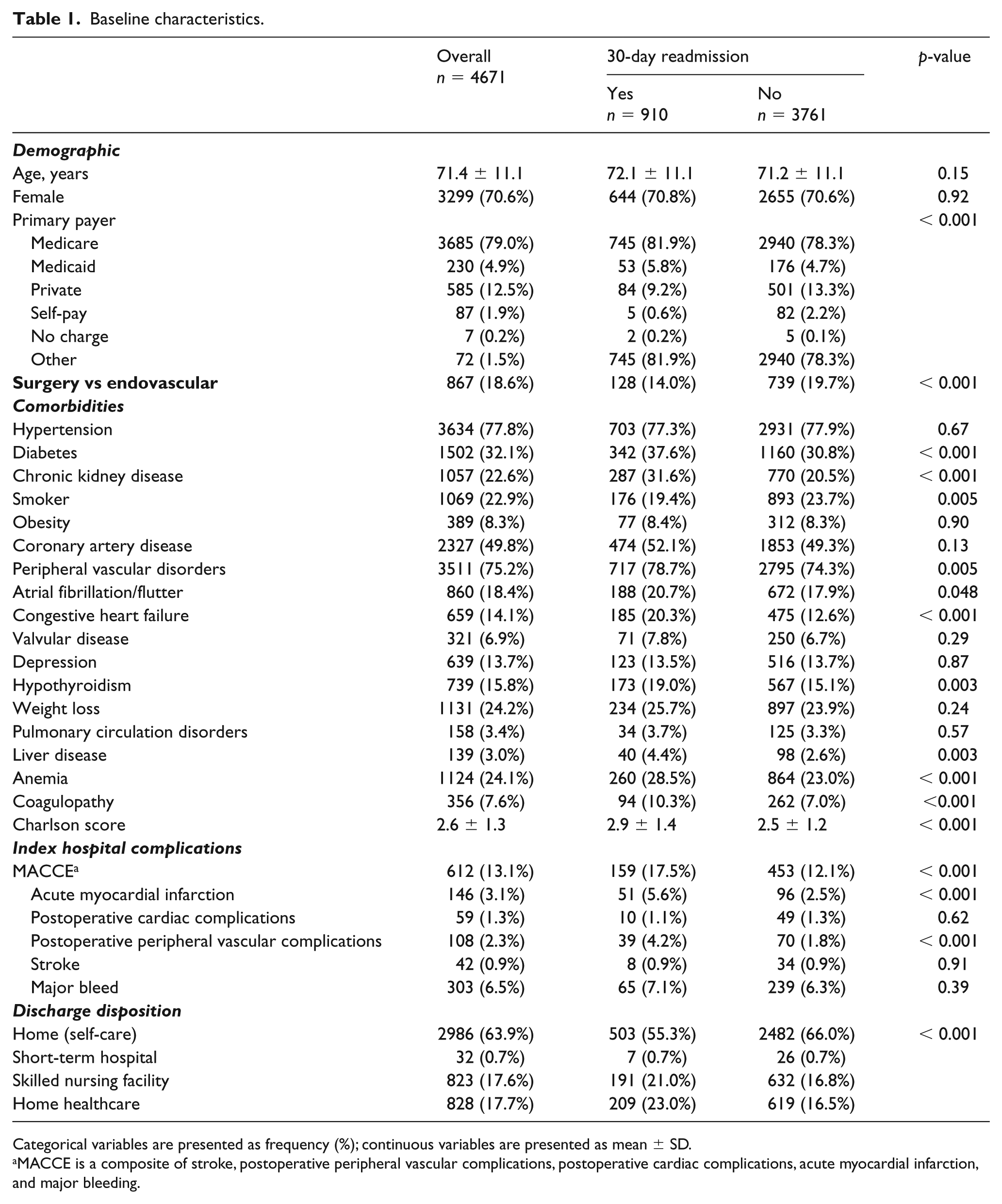
Categorical variables are presented as frequency (%); continuous variables are presented as mean ± SD.
MACCE is a composite of stroke, postoperative peripheral vascular complications, postoperative cardiac complications, acute myocardial infarction, and major bleeding.
Incidence and predictors of 30-day readmission
The overall rate of 30-day readmission was 19.5%. Median time-to-readmission was 10 (IQR 5-17) days. The observed unadjusted readmission rates were higher for the endovascular than surgical group (20.6% vs 14.7%, p < 0.001). Independent predictors of 30-day readmission after revascularization for CMI are shown in Figure 2. In order of greatest to least importance, based on chi-square values, these included non-elective index admission (χ2 = 18.22), CKD (χ2 = 9.81), discharge to HHC (vs home with self-care) (χ2 = 8.73), and discharge to SNF (vs home with self-care) (χ2 = 7.21). Revascularization modality (surgical vs endovascular) did not significantly predict 30-day readmission in the multivariable analysis (OR 0.91 [95% CI 0.63–1.31], χ2 = 0.26, p = 0.61). In multivariable testing, bowel resection was not significantly associated with readmission (p = 0.43). Although LOS may be a marker for complications, it was not independently predictive of readmission when included in a multivariable regression model along with complications (p = 0.194).
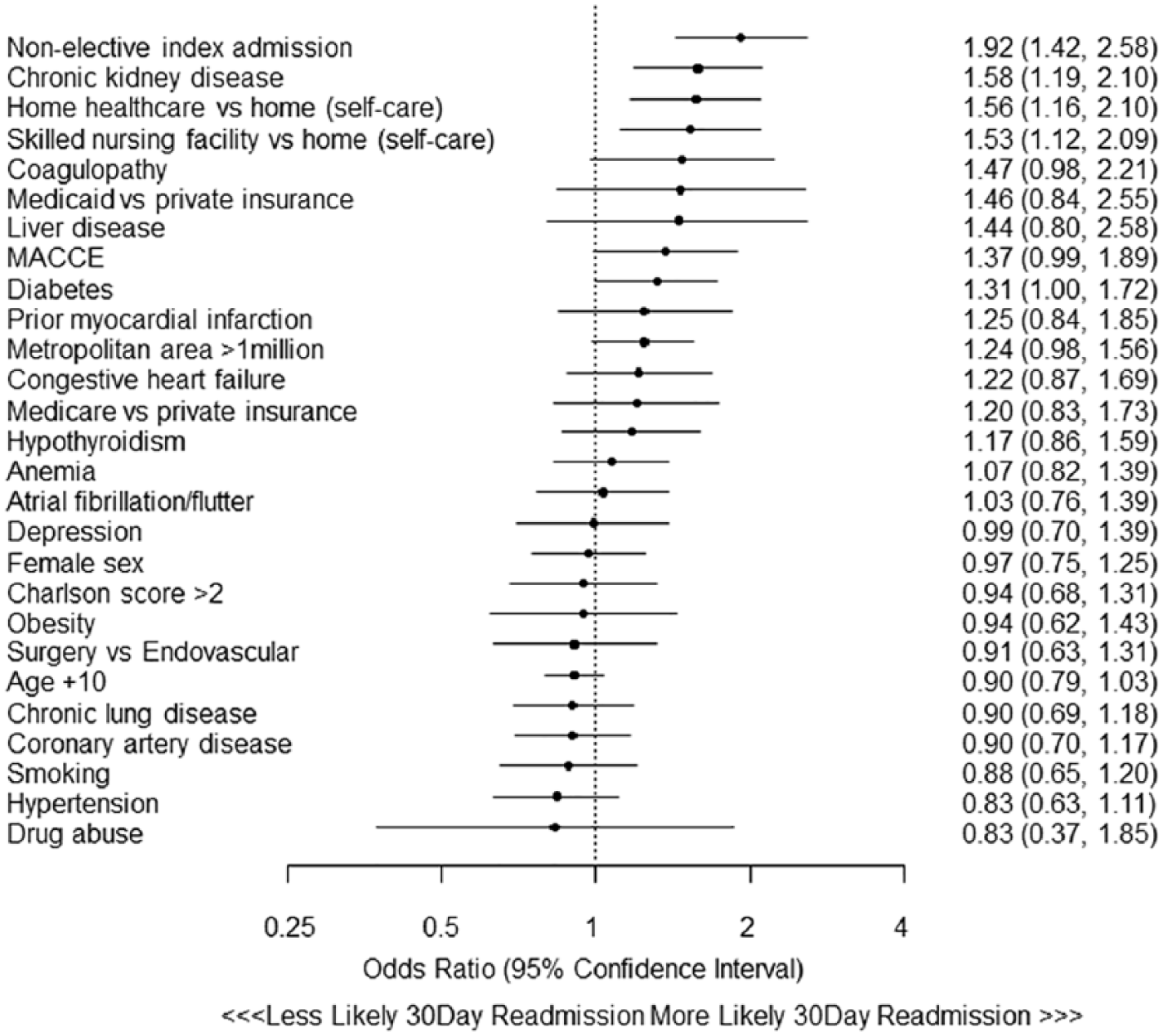
Hierarchical logistic regression model predicting 30-day readmission after endovascular or surgical revascularization for chronic mesenteric ischemia.
Readmission reasons, LOS and costs
The most frequent reasons for 30-day readmissions were cardiovascular and cerebrovascular conditions (27%), non-hemorrhagic gastrointestinal conditions (19%), and treatment-related complications (14%) (Figure 3A). Of readmissions for cardiovascular and cerebrovascular conditions, 10% were for peripheral or visceral atherosclerosis, most of which were for acute or chronic mesenteric ischemia (Supplemental Figure 1); 5% were for congestive heart failure (Figure 3B). Among readmissions for treatment-related complications, the most common that necessitated readmission were complications due to vascular device, implant/graft (20%), postoperative infection (16%), and peripheral vascular complications (12%) (Supplemental Figure 2). A comprehensive list of reasons for readmission is provided in Supplemental Table 2 and Supplemental Figures 1 and 2. Among patients whose index LOS was < 6, 6–11, and 12+, respective readmission rates were 14.8%, 20.2%, and 28.5%.
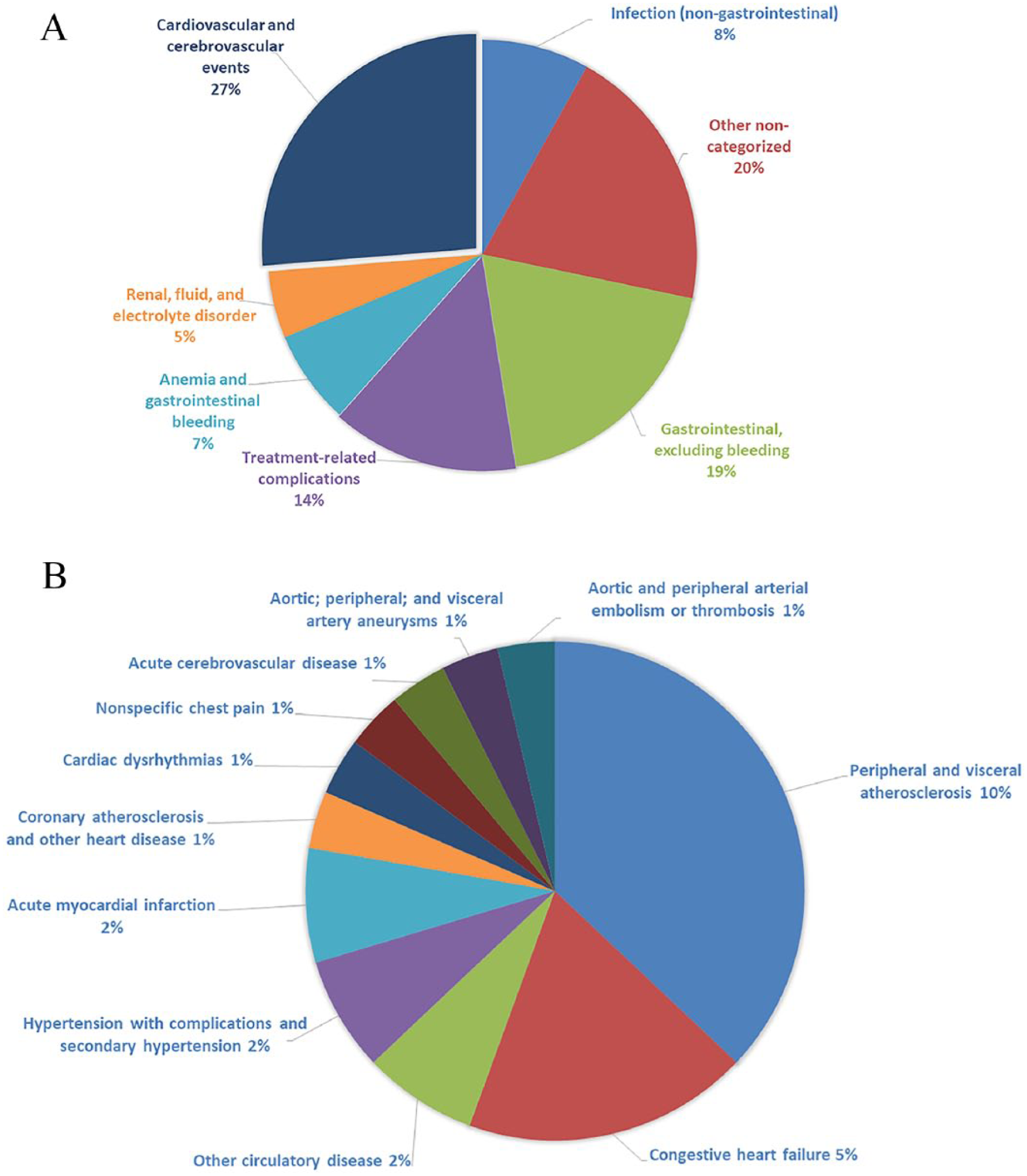
(A) Reasons for 30-day readmissions after endovascular or surgical revascularization for chronic mesenteric ischemia. (B) Cardiovascular and cerebrovascular reasons for 30-day readmission after endovascular or surgical revascularization for chronic mesenteric ischemia.
Overall median LOS during readmission hospitalizations was 5 (IQR 3–9) days. Median overall cost per readmission stay was US $9586 (IQR $5670 – $20,770). The national estimate of aggregate costs for readmission after CMI revascularization was $14,634,678.
Discussion
In a contemporary, nationally representative population of patients with CMI undergoing endovascular or surgical revascularization, nearly one in five patients was readmitted within 30 days of index hospital discharge. Median overall time to readmission was only 10 days and the median overall LOS for readmission was 5 days. More than one in four readmissions were for cardiovascular or cerebrovascular conditions (the majority of which were for peripheral or visceral atherosclerosis and congestive heart failure), one in five were for gastrointestinal issues, and one in seven were for medical or procedural complications. The estimated aggregate cost for all 30-day readmissions was more than $14 million. Independent predictors of readmission at 30 days included non-elective index admission, CKD, discharge with HHC, or discharge to SNF. Interestingly, neither female sex, which accounted for 70% of the overall patient population, nor increasing age, was independently associated with readmission. Previous analyses have observed that female sex and older age are associated with readmission after other cardiovascular procedures.9–11 Although we previously demonstrated in a large nationwide analysis that endovascular revascularization was associated with fewer index hospital complications (including MACCE), lower costs, and shorter lengths of stay compared with surgery, 3 there was no independent association between revascularization strategy and likelihood of readmission.
Multispecialty consensus guidelines provide Class 1 (Level B) recommendations for the diagnostic workup of presumed CMI. 2 Patients who present with abdominal pain and weight loss, especially in the presence of established cardiovascular disease, but without another apparent etiology, should undergo duplex ultrasonography, gadolinium-enhanced magnetic resonance angiography, computed tomography angiography or invasive angiography 2 to rule out mesenteric artery stenosis or occlusion. Generally, patients with symptomatic flow-limiting stenotic lesions in one or more mesenteric vessels, most commonly the celiac or superior mesenteric arteries, should undergo either endovascular or open surgical repair. Since the early 2000s, the endovascular approach has become increasingly more common. It is associated with lower in-hospital mortality, shorter LOS, and fewer bowel resections,3,12,13 but also with a higher rate of restenosis with symptom recurrence, requiring reintervention. 14 It is unlikely that these later events would impact 30-day readmission rates.
Percutaneous and surgical revascularization procedures account for some of the highest 30-day readmission rates nationwide, particularly among the Medicare population. 15 Our study provides the first contemporary, nationwide assessment of 30-day readmission following revascularization for CMI in the US. In a prospective observational study of 31 endovascular and 49 open surgery patients undergoing mesenteric revascularization, the 4-year readmission rate was driven by symptomatic restenosis necessitating repeat revascularization. 16 To our knowledge, ours is the only other study to date which has examined readmission rates in this setting, and the first to examine this endpoint at 30 days. Our observed 30-day readmission rate is substantial, and on par with that seen for other cardiovascular conditions and procedures, including heart failure (24.8%), AMI (19.9%), critical limb ischemia (20.4%) and infrainguinal bypass grafting (15.7%).17–19 In previous work, we17,20 and others 21 observed that index hospitalization complications were significant predictors of readmission after cardiovascular procedures. In the present study, there was a strong trend between index hospitalization MACCE and likelihood of readmission, although this did not reach statistical significance. Nevertheless, these new data should not distract clinicians from implementing interventions aimed at complication screening and management to reduce 30-day readmissions, as described by prior investigators22–24 and should heighten awareness of readmission risk in patients presenting for revascularization from the outset. Others have observed a strong association between index hospitalization discharge to SNF and readmission.21,25 The Interventions to Reduce Acute Care Transfers (INTERACT) II study demonstrated that utilization of specific early interventions by SNF staff, including identifying, assessing, and communicating changes in patients’ status to physicians yielded a 24% reduction in readmission rates from a SNF. 26 Likewise, a systems-based approach with transitions of care teams has been successfully implemented in patients with heart failure, resulting in reduced 30-day readmissions, 27 and similar approaches, if routinely applied, may have reduced readmission rates in our study cohort. Nevertheless, discharge to SNF and HHC is often associated with a higher burden of frailty and comorbid conditions, which, while important predictors, may not be modifiable.28,29
The financial burden of readmission after mesenteric revascularization was appreciable in our study population. After adjusting for inflation, the median cost per readmission in 2017 dollars was nearly $10,000. 8 This represents a national aggregate cost of $14,634,678. Interventions that reduce the likelihood of readmission have the potential for significant healthcare cost reductions.
Thirty-day readmission rates for conditions like heart failure, AMI, and pneumonia have been applied as markers of hospital performance by the Centers for Medicare and Medicaid Services and used to critique hospitals’ quality of care. 30 Since the inception of the Affordable Care Act’s Hospital Readmissions Reduction Program, there have been appreciable nationwide improvements in 30-day readmission rates for these target conditions.31–33 Readmission rates for non-targeted conditions have also shown modest progress.31,33 Although many readmission drivers in our study were nonmodifiable (e.g. CKD and discharge to HHC or SNF), it is plausible that identification of these might prompt more timely or frequent post-discharge surveillance, culminating in reduced readmission rates.
Limitations
Our study has noteworthy limitations. First, this was a retrospective, observational analysis. Consequently, we are unable to rule out residual confounding despite multivariable analysis. Second, the study utilized claims data. ICD-9 coding errors can occur; however, the error rates have been shown to be low 34 and previous studies have shown high specificity and positive predictive value for similar cardiovascular diseases.35–38 Additionally, other published studies have used similar codes when studying this disease state.3,12,13,39 It is, however, not possible to reidentify patients from the NRD in order to conduct an in-hospital audit. Third, laboratory data, vital signs, medications, and anatomical information were not available. Fourth, vital status between index hospitalization discharge and readmission was unavailable. Similarly, the NRD does not provide data on cause of death during readmissions. Fifth, our longitudinal assessment of outcomes only extended to 30 days post-index hospitalization. Other factors may drive readmission at later time points. Sixth, the percentage of patients with CMI who underwent mesenteric revascularization was lower than expected; it is possible that those who underwent stenting did so as an outpatient and, for that reason, did not appear in the NRD, an inpatient database. Finally, CMI may be treated in the outpatient setting and such cases would not have been included in this inpatient database.
Conclusions
In a contemporary, nationwide, cohort of patients undergoing revascularization for CMI, one in five patients was readmitted within 30 days. Non-elective index admission, CKD, and discharge disposition, but not revascularization modality, predicted 30-day readmission. These data provide important insights into the short-term, post-revascularization outcomes for patients with CMI. Efforts to prevent or reduce non-elective admissions may translate into lower rates of readmission.
Supplemental Material
10.1177_1358863X18816816_supplemental_material_tables – Supplemental material for Thirty-day readmission after endovascular or surgical revascularization for chronic mesenteric ischemia: Insights from the Nationwide Readmissions Database
Supplemental material, 10.1177_1358863X18816816_supplemental_material_tables for Thirty-day readmission after endovascular or surgical revascularization for chronic mesenteric ischemia: Insights from the Nationwide Readmissions Database by Fabio V Lima, Dhaval Kolte, David W Louis, Kevin F Kennedy, J Dawn Abbott, Peter A Soukas, Omar N Hyder, Shafiq T Mamdani and Herbert D Aronow in Vascular Medicine
Supplemental Material
10.1177_1358863X18816816_supplementary_material_figure1 – Supplemental material for Thirty-day readmission after endovascular or surgical revascularization for chronic mesenteric ischemia: Insights from the Nationwide Readmissions Database
Supplemental material, 10.1177_1358863X18816816_supplementary_material_figure1 for Thirty-day readmission after endovascular or surgical revascularization for chronic mesenteric ischemia: Insights from the Nationwide Readmissions Database by Fabio V Lima, Dhaval Kolte, David W Louis, Kevin F Kennedy, J Dawn Abbott, Peter A Soukas, Omar N Hyder, Shafiq T Mamdani and Herbert D Aronow in Vascular Medicine
Supplemental Material
10.1177_1358863X18816816_supplementary_material_figure2 – Supplemental material for Thirty-day readmission after endovascular or surgical revascularization for chronic mesenteric ischemia: Insights from the Nationwide Readmissions Database
Supplemental material, 10.1177_1358863X18816816_supplementary_material_figure2 for Thirty-day readmission after endovascular or surgical revascularization for chronic mesenteric ischemia: Insights from the Nationwide Readmissions Database by Fabio V Lima, Dhaval Kolte, David W Louis, Kevin F Kennedy, J Dawn Abbott, Peter A Soukas, Omar N Hyder, Shafiq T Mamdani and Herbert D Aronow in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.