
Abstract

What are the mesenteric arteries?
Arteries are thick-walled, muscular vessels that supply blood and oxygen to the major organs. As shown in Figure 1, the intestines are supplied by three major arteries (called mesenteric arteries): the celiac artery, the superior mesenteric artery, and the inferior mesenteric artery. These arteries provide a rich, overlapping blood supply to the intestines. Although problems with these arteries are not common, issues can arise when these vessels become blocked, abnormally dilated, inflamed, or compressed by other structures in the abdomen.
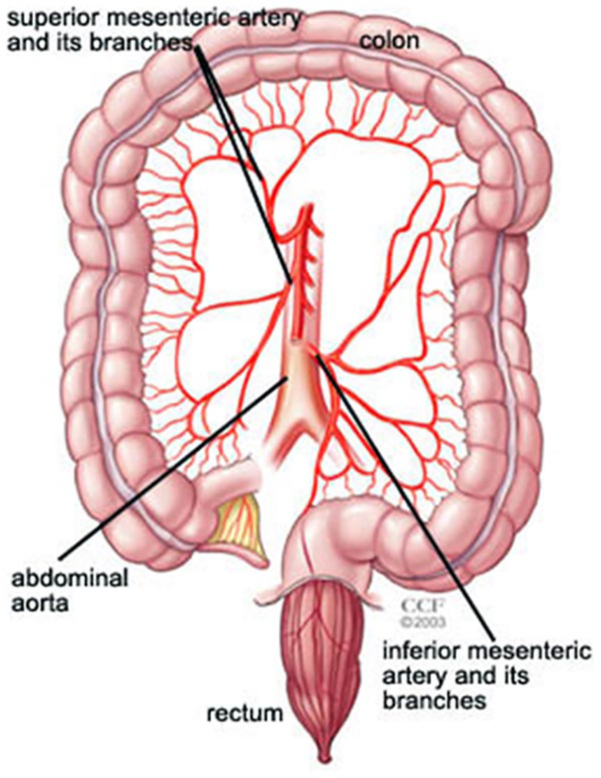
The blood supply to the intestines includes the celiac artery (not shown), the superior mesenteric artery, and the inferior mesenteric artery. Each of these arteries has multiple branches.
What problems can occur with the mesenteric arteries? What is mesenteric ischemia?
Blocked or narrowed arteries are a common reason for mesenteric artery disease. The most common cause of blockage in the intestinal arteries is plaque build-up within the artery walls (also called atherosclerosis; illustrated in Figure 2). This plaque is made of fat, cholesterol, and calcium, and, over time, it can decrease or stop blood flow through the arteries. The risk factors for atherosclerosis include smoking, diabetes, high blood pressure, obesity, kidney disease, and high cholesterol. This blockage or narrowing (also called stenosis) can prevent the intestines or organs in the abdomen from receiving enough blood and oxygen—a condition called mesenteric ischemia.
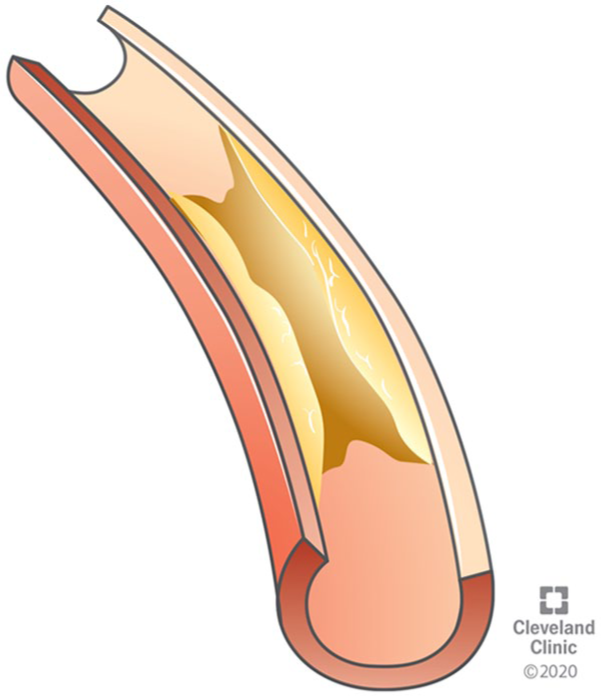
In chronic mesenteric ischemia, an artery is narrowed by atherosclerotic plaque, which limits the blood flow.
Ischemia can occur whenever an essential area is deprived of blood flow. For example, chest pain (‘angina’) occurs when the heart arteries are blocked. With mesenteric artery disease and mesenteric ischemia, abdominal pain (also called ‘intestinal angina’) occurs because the stomach, liver, colon, and/or intestines are affected. To cause symptoms, the blockage is usually severe and involves more than one mesenteric artery. This problem is more common among older people, especially after age 60, but it can occur at any age. Patients who have mesenteric artery blockages often have plaque in other vascular areas as well, such as heart disease or peripheral artery disease (blockages in the arteries that supply the legs).
Mesenteric ischemia is typically described as either ‘chronic’ or ‘acute’. It is called chronic when the decrease in blood flow is gradual over time, and it is called acute when the decrease in blood flow happens suddenly (often from a blood clot). 1 Acute mesenteric ischemia can occur when an irregular heartbeat called atrial fibrillation leads to small clots in the heart, which can then travel into the circulation of the intestines.
Other less common problems with the intestinal arteries include abnormal dilation or out-pouching of the artery wall (aneurysm), leakage of blood between the layers of the artery walls due to a tear (dissection), inflammation of the vessels (vasculitis), or compression of the arteries by other structures in the abdomen. If there is a problem with the pumping function of the heart, blood circulation to the mesenteric arteries can also be limited and cause symptoms. 2
What are the symptoms and complications of mesenteric artery problems?
Abdominal pain is the main symptom of problems with intestinal blood flow. Chronic mesenteric ischemia symptoms may come on gradually. Symptoms can include abdominal pain that starts about 30 to 60 minutes after eating, when the blood flow is not enough to meet the demands of digestion. The pain may get worse for an hour or so, then improve and go away in a few hours. Other symptoms may include unintentional weight loss, fear of eating, feeling full quickly when eating, constipation, or diarrhea.
With acute mesenteric ischemia, the loss of blood flow is sudden, and the abdominal pain is typically sudden and severe. It may also be accompanied by nausea, vomiting, diarrhea, fever, a sense of urgency to have a bowel movement, or bloody stools. Patients with acute mesenteric ischemia may or may not have experienced chronic symptoms beforehand (such as abdominal pain after eating and weight loss). Although the pain in the abdomen may be severe, there may not be tenderness when pressing on the abdomen. Complications of acute mesenteric artery ischemia are more severe and may include bloodstream infection, injury to the lining of the bowel (which may require an operation), or even death.
How is mesenteric artery stenosis diagnosed?
Several tests are available to diagnose mesenteric artery disease and stenosis. These may include an angiogram. An angiogram is a minimally invasive procedure during which a thin flexible tube is introduced into an artery in the groin or arm. Dye is then injected to visualize the blood flow and the amount and location of the blockage.
Vascular ultrasound studies may be helpful in viewing the arteries and blood flow to determine the level of blockage. This specialized test is noninvasive and depends on the vascular lab and technologist to provide the best information. As shown in Figure 3, high blood flow velocities help to diagnose a narrowed blood vessel.
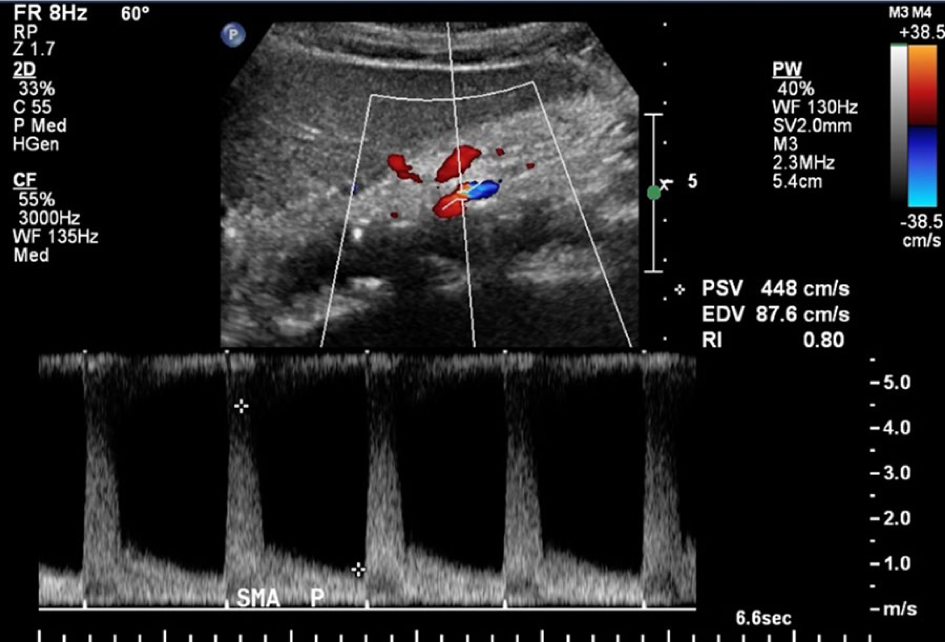
Vascular ultrasound is useful to look for an increase in blood flow velocity and turbulent flow in the blood vessel, which indicate that the artery is narrowed. The image shows stenosis (narrowing) of the superior mesenteric artery (SMA).
Computed tomographic angiography (CTA) and/or magnetic resonance angiography (MRA) are sometimes used as well. These noninvasive radiology tests can show problems with the artery, such as narrowing or tears, and can help guide treatment decisions.
An echocardiogram (ultrasound of the heart) may be recommended to look for a blood clot and to check the heart function. A heart monitor may be needed to look for a heart rhythm abnormality, such as atrial fibrillation.
If there are no symptoms but stenosis is found on an imaging test, is treatment necessary?
Sometimes vessel blockage (stenosis) is found incidentally on images done for other medical problems. Plaque within the arteries (atherosclerosis) is always abnormal, but it may not cause any symptoms. In this situation, medical treatment and lifestyle modification can reduce the risk of heart attack and stroke.
What are the medical (noninvasive) treatment options for symptoms of mesenteric artery stenosis?
Medical treatment of atherosclerosis may include medications, lifestyle changes, such as quitting smoking and altering diet, and risk factor management. 3 Medications used to treat patients at risk of heart attack or stroke from atherosclerosis often include a blood thinner (e.g. aspirin) and a statin to lower cholesterol and stabilize the plaque. To learn more about statins, read the Vascular Disease Patient Information Page on ‘Statins’. 4
Smoking is a strong risk factor for atherosclerosis, and quitting smoking is of the utmost importance. To learn more about quitting smoking, read the Vascular Disease Patient Information Page on ‘Smoking cessation’. 5 Controlling diabetes and high blood pressure with appropriate medications is important, along with exercise and maintaining a normal weight. 6
Eating small meals and avoiding large, fatty meals may help with some of the symptoms of this condition.
When is invasive treatment required?
Acute mesenteric ischemia often requires urgent surgical evaluation and management. Sometimes intravenous blood thinners are used to stabilize the clot in the artery. Special clot-dissolving agents or clot removal devices may be used as well. For chronic mesenteric ischemia, treatment is needed if bothersome symptoms continue, such as unintended weight loss, abdominal pain with eating, or fear of eating.
What are the surgical (invasive) options for treating mesenteric artery disease?
For an acute mesenteric artery blockage, blood flow typically must be restored immediately. This condition is usually considered a surgical emergency. 7 For chronic mesenteric ischemia due to an artery narrowing or blockage, elective surgery to restore circulation can be done if necessary.
In general, the less invasive option for restoring blood flow is balloon angioplasty and stenting, as illustrated in Figures 4A and 4B. Open surgery is a more invasive treatment option in which the blocked artery is bypassed (Figure 5).
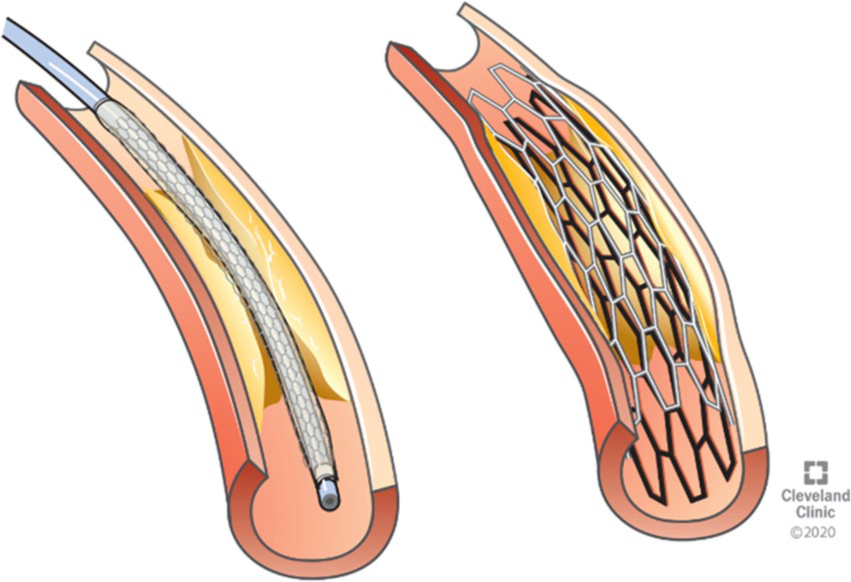
A catheter is threaded through the narrowed area in the blood vessel (left). With angioplasty, a balloon is used to open up the blockage, and then a metal strut (stent) is placed to prop open the narrowed area (right).
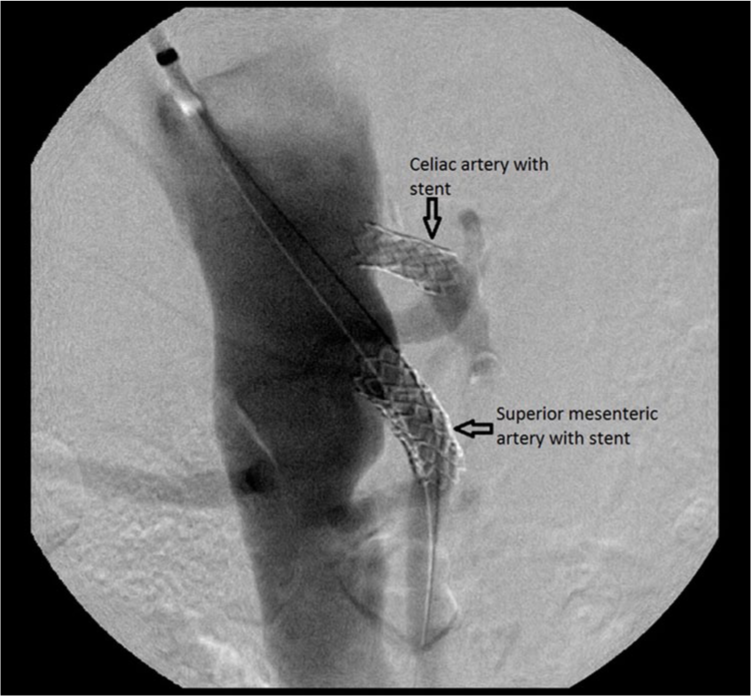
This X-ray image from an angiogram shows the stents (arrows) in the celiac artery and superior mesenteric artery, which were placed to treat chronic mesenteric ischemia.
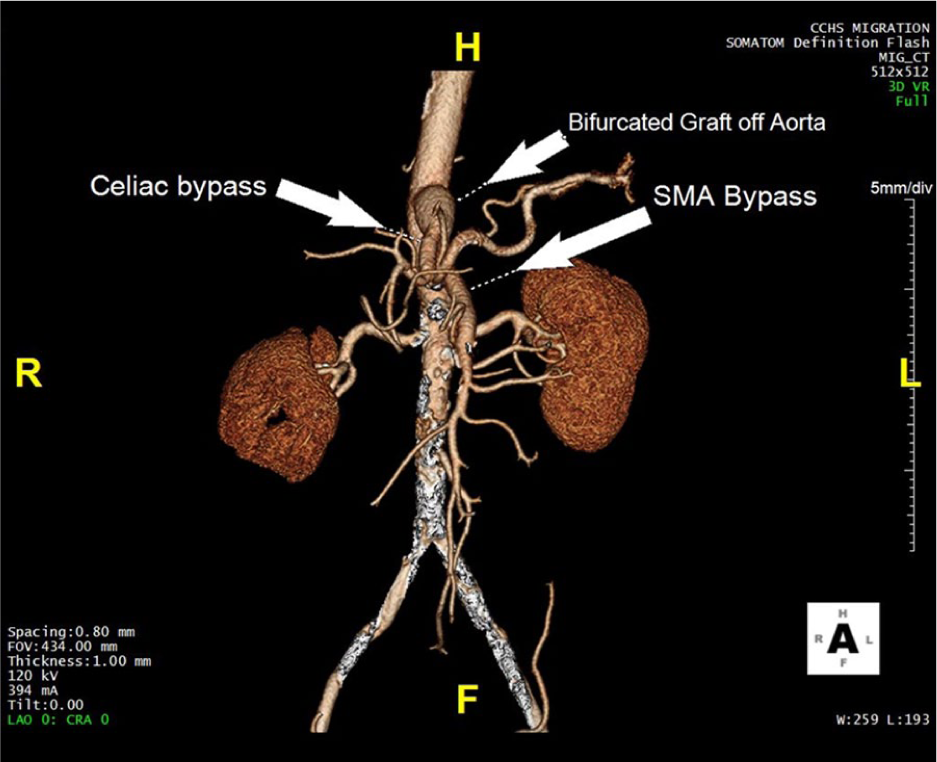
This CTA image shows how surgical bypass for mesenteric artery stenosis can re-route the blood flow.
How can mesenteric artery problems be prevented?
Maintaining a healthy lifestyle with diet and exercise is important to prevent the progression of atherosclerosis. Avoiding tobacco, controlling blood sugars in diabetes, lowering cholesterol levels using statin medications, lowering high blood pressure, and taking blood-thinning medications such as aspirin are all important strategies to reduce blood vessel risk, including in the mesenteric arteries.
Summary
Narrowing (stenosis) of the mesenteric arteries is most commonly caused by atherosclerosis. The symptoms can depend on whether the blockage is acute (sudden) or chronic, and a variety of symptoms including abdominal pain may occur. The diagnosis can be made by several different imaging tests, and treatment strategies include lifestyle modification, risk factor management, and medications. Both surgical procedures and less invasive endovascular procedures are available to bypass or open up blocked arteries to restore blood flow if needed.
The ‘Vascular Disease Patient Information Page’ is a regular feature of Vascular Medicine. All articles in the collection are available for free online at http://journals.sagepub.com/vmjpatientpage.
The Vascular Disease Patient Information Page is provided for educational purposes only and is not a substitute for medical advice.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.