
Abstract

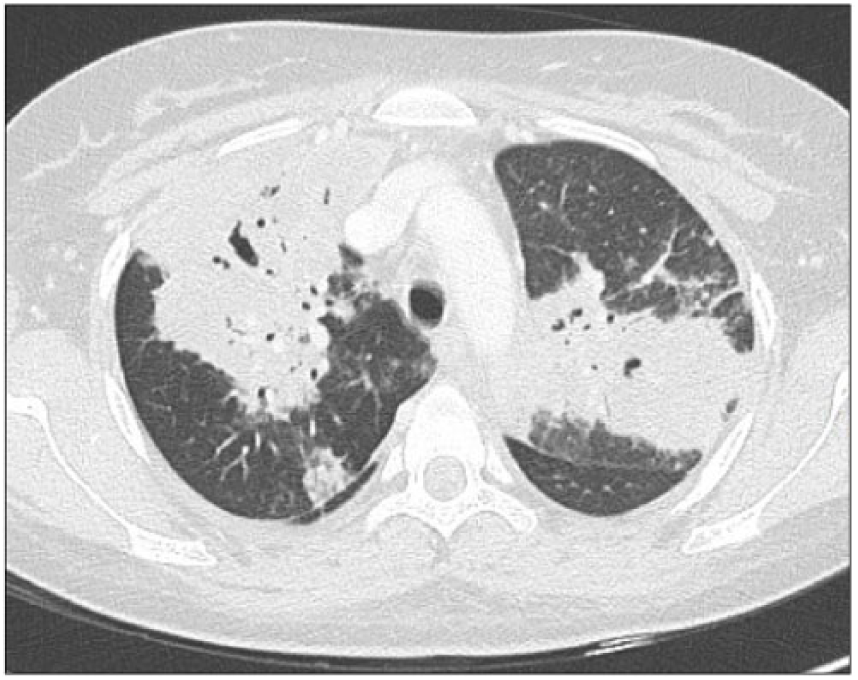
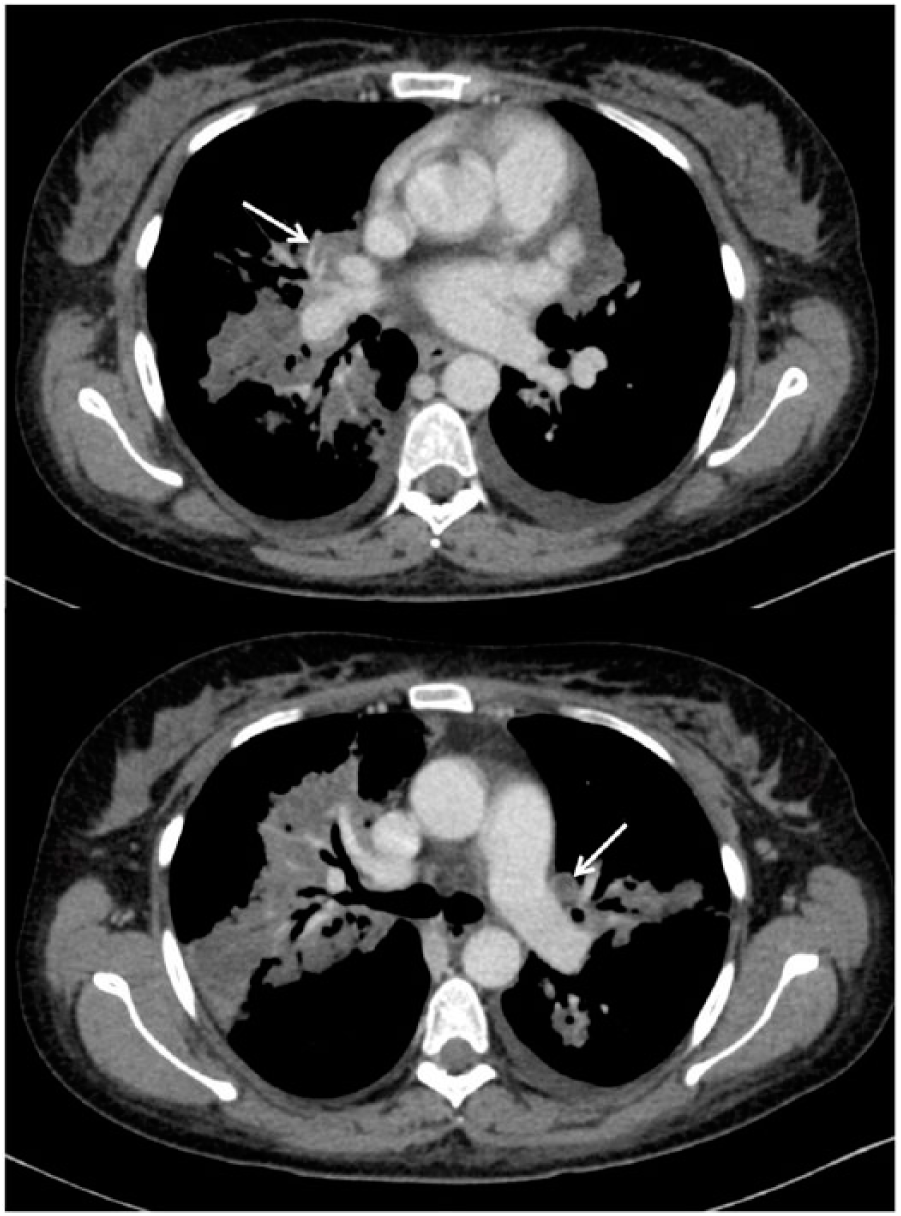
A 30-year-old woman presented with a 3-month history of cough, haemoptysis, sinusitis, and fever during pregnancy. Symptoms worsened 2 months after delivery, with fever and dyspnea despite several antibiotic therapies. On examination, splinter haemorrhages of the nails (Panel A) were noticed. Biological exams revealed hypereosinophilia at 1500/mm3 and suggested renal impairment with mild proteinuria at 0.7 g/g and haematuria via urinary dipstick. Radiological examination showed bilateral excavated lung nodules (Panel B) and splenic infarcts (Panel C). Proteinase 3-antineutrophil cytoplasmic antibodies (ANCA) were positive. Granulomatosis with polyangiitis (GPA) was diagnosed and the patient was treated with a combination of intravenous methylprednisolone followed by prednisone and rituximab leading to rapid improvement in clinical and laboratory findings. Three days after initial therapy, a second computed tomography (CT) scan revealed bilateral pulmonary embolism (PE) (Panel D, arrows). Antiphospholipid antibodies were negative and other causes of venous thrombosis were excluded. An anticoagulant therapy with enoxaparin was introduced then switched to rivaroxaban. Considering the slow regression of lung nodules and the persistence of inflammation attested by biological markers, anticoagulant therapy was continued for 6 months, leading to clinical improvement. The platelet count remained high (892 g/L) and secondary prophylaxis with aspirin 100 mg/day was introduced thereafter.


The pathophysiology of splinter haemorrhages is still not fully understood, although disruption of spiral arteries of the nail bed and local microthrombosis are characteristic. Splinter haemorrhage represents a frequent although not specific clinical finding, mostly reported in infective endocarditis, antiphospholipid syndrome and hypereosinophilic syndrome, 1 but very rarely described in ANCA-associated vasculitis. 2 Treatment is aetiological and consists of controlling the underlying disease. Although splenic infarcts have rarely been reported during GPA, autopsy studies suggest that it might be a common feature. The association of splinter haemorrhages, splenic infarction, and PE is unusual and suggests vasculitis-mediated increased procoagulant activity. Indeed, it was found that 8% and 2.5% of patients with GPA and periarteritis nodosa, respectively, experienced a venous thrombotic event during a mean follow-up of 58.4 months. 3 Events mainly occurred during the active phases of disease. However, the respective role of inflammation, size of involved vessel, and ANCA specificity is unknown and the pathophysiology of thrombosis remains speculative in the context of vasculitis. Unlike Behçet disease, anticoagulant therapy is always initiated when a venous thrombosis occurs in patients with GPA. It was mandatory in our patient who experienced multiple arterial and venous thrombosis.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.