
Abstract
Pain is a common symptom and the major complaint in patients with venous malformations of the extremities, which may lead to joint dysfunction and even walking disabilities. Therefore, this study aimed to investigate determined independent risk factors for pain in these patients. We retrospectively collected data for 168 patients with venous malformations of the extremities from January 16, 2013 to August 13, 2015. They were categorized into painful and painless groups according to the symptom and pain scores. Associations between pain and candidate factors were determined using univariate and multivariate analyses. A total of 125 (74.4%) patients with an average pain score of 4.4 were included in the painful group. In univariate analysis, age, lesion size, tissue involvement, and phleboliths were associated with pain. In the multivariate analysis, only type-II tissue involvement (adjusted odds ratio 4.57; p = 0.001) and phleboliths (adjusted odds ratio 2.44; p = 0.039) were identified as the independent risk factors. In conclusion, this study revealed that prevalence of pain in patients with venous malformations of the extremities was high. Patients who presented with type-II tissue involvement and phleboliths are more likely to suffer from pain.
Introduction
Venous malformations are one of the most common congenital vascular anomalies. The vast majority of venous malformations are sporadic, solitary, light to dark blue colored, and soft lesions that are noted at birth or early in childhood. Approximately half of venous malformations occur in the head and neck regions, whereas the remainder are distributed predominantly on the extremities and, less frequently, on the trunk.1,2 Thus, the extremities constitute the second most common region.
Venous malformations can occur in any tissue and are associated with various clinical presentations. Craniofacial venous malformations may cause disfigurement, skeletal deformity, and even upper airway obstruction. 1 Venous malformations of the extremities can lead to swelling, pain, functional impairment, and localized intravascular coagulation.3–5 Of these symptoms, pain is most commonly reported among patients with venous malformations of the extremities.3,6 Mautner and Sussman 7 reported that frequent pain associated with limb venous malformations could progress to walking pain and eventually lead to functional impairment. A previous study demonstrated that patients with limb venous malformations who suffered from chronic pain had higher risk for joint dysfunction. 8 Pain was also identified as having the greatest impact on quality of life in a questionnaire, including pain, physical, social, and psychological dimensions. 9 The aim of this retrospective study was, therefore, to investigate independent risk factors for pain in patients with venous malformations of the extremities.
Materials and methods
Study design
After approval from the local institutional review board, a total of 168 patients with pure venous malformations of the extremities who sought care at our vascular anomaly center between January 16, 2013 and August 13, 2015 were included in this study. Patients with capillary venous malformations, lymphatic venous malformations, or Klippel-Trenaunay syndrome were excluded from the study. The diagnosis of venous malformation was based on clinical and radiologic examinations. 10 The clinical criterion was early presentation of a lesion with progressive growth with age and regurgitation of blood on direct puncture of the lesion. The radiologic criterion was a mass presenting high signal on T2-weighted (T2-W) suppression sequences, with wide venous pools confirmed by contrast-enhanced magnetic resonance imaging (MRI).
Patient data collected comprised demographic characteristics, clinical presentations, and imaging results. Patients were categorized into two groups: painful and painless. Patients who suffered from pain were considered for inclusion in the painful group. In addition, pain intensity was assessed using a verbal numeric rating scale (NRS) and reported as a score between 0 and 10 (0 = no pain, 10 = worst pain imaginable) at a patient’s first visit. 11 It has been demonstrated that the parent’s score was highly consistent with the child’s score when both of them were asked to assess the child’s pain using a NRS. 12 If a young patient is unable to assess his/her pain, then the assessment of the parent would be sought. Imaging results were reviewed by three radiologists blinded to patients’ symptoms. Candidate factors for investigation based on the existing literature were as follows:
1) Sex
2) Age (⩽ 16 or > 16 years old); we chose age 16 as the boundary because it was the median age of the 168 patients
3) Lesion location (upper or lower extremities)
4) Lesion size (maximum cross-sectional area on the MRI: ⩽ 10 cm2 or > 10 cm2) 5
5) Tissue involvement (type I: only skin and subcutaneous tissue involved; type II: muscle, bone or joint involved with or without skin and subcutaneous lesions). The appearance of tissue involvement by MRI was categorized into the two types according to the Birmingham classification 13
6) Phleboliths (yes or no). These presented as granular, high density on X-ray or a hypo-intense signal on T1-W as well as T2-W sequences of MRI without enhancement. 14
Statistical analysis
All analyses are based on the 168 patients. Continuous and normally distributed variables are presented as the mean ± SD. Categorical variables are presented as numbers (percentages).
Associations between pain and candidate factors were determined using univariate and multivariate statistical analyses. In the univariate analysis, variable frequencies were compared between the painful and painless groups using χ2 tests. In the multivariate analysis, variables significantly associated with pain in the univariate analysis were entered into logistic regression models. For all the statistical analyses, p < 0.05 was considered statistically significant. Statistical analyses were performed with SPSS Statistics, Version 23.0 (IBM Corp., Armonk, NY, USA).
Results
Among the 168 patients, the sample consisted of 65 males and 103 females with ages ranging from 3 to 61 years and a mean age ± SD of 21.5 ± 11.8 years. The median age of 168 patients was 16 years old. Figures 1–4 present typical patients in the two groups. None of the 168 patients presented skin ulceration or bleeding. A total of 80 patients had received previous treatment, including surgery, sclerotherapy, radiotherapy, copper needles, and cryotherapy. Among them, 49.60% (62/125) patients were in the painful group and 41.86% (18/43) were in the painless group.
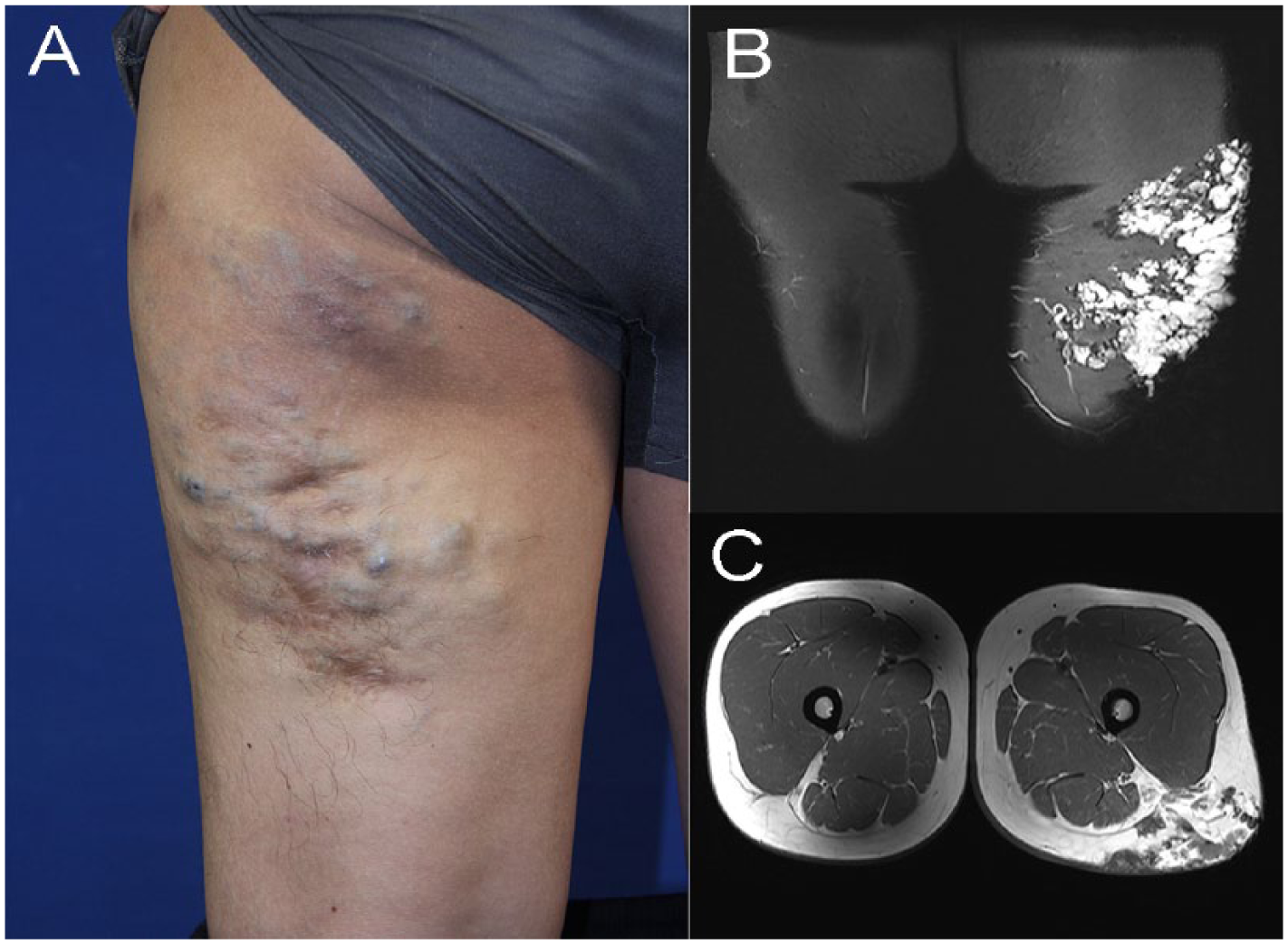
A 29-year-old male presented with a 10-year history of a gradually enlarging, light to dark blue lesion on his left thigh. He denied any pain in daily life. (A) Physical examination revealed the lesion was compressive. (B and C) Coronal and axial MR images, respectively, presented a diffuse venous malformation within cutaneous and subcutaneous tissue of the left thigh that indicated type-I tissue involvement.
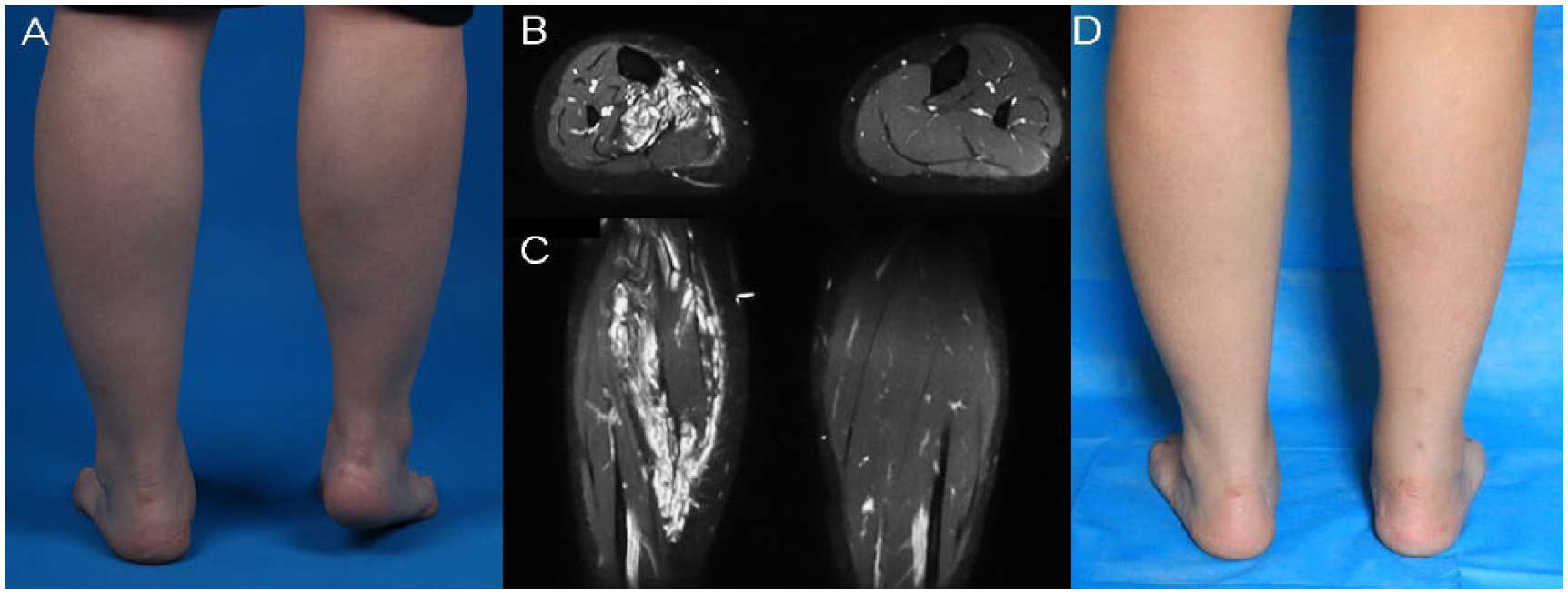
A 24-year-old female with a painful venous malformation (NRS score = 5) in the right calf. She suffered from pain occasionally since 17 years old, which was greatest during running and disappeared spontaneously within a few days. She experienced total relief from pain (NRS score = 0) after two sessions of sclerotherapy, and received an Achilles tendon lengthening. (A) Physical examination revealed an equinus due to the short Achilles tendon. (B and C) Axial and coronal MR images, respectively, showed type-II tissue involvement. (D) Six months after Achilles tendon lengthening.
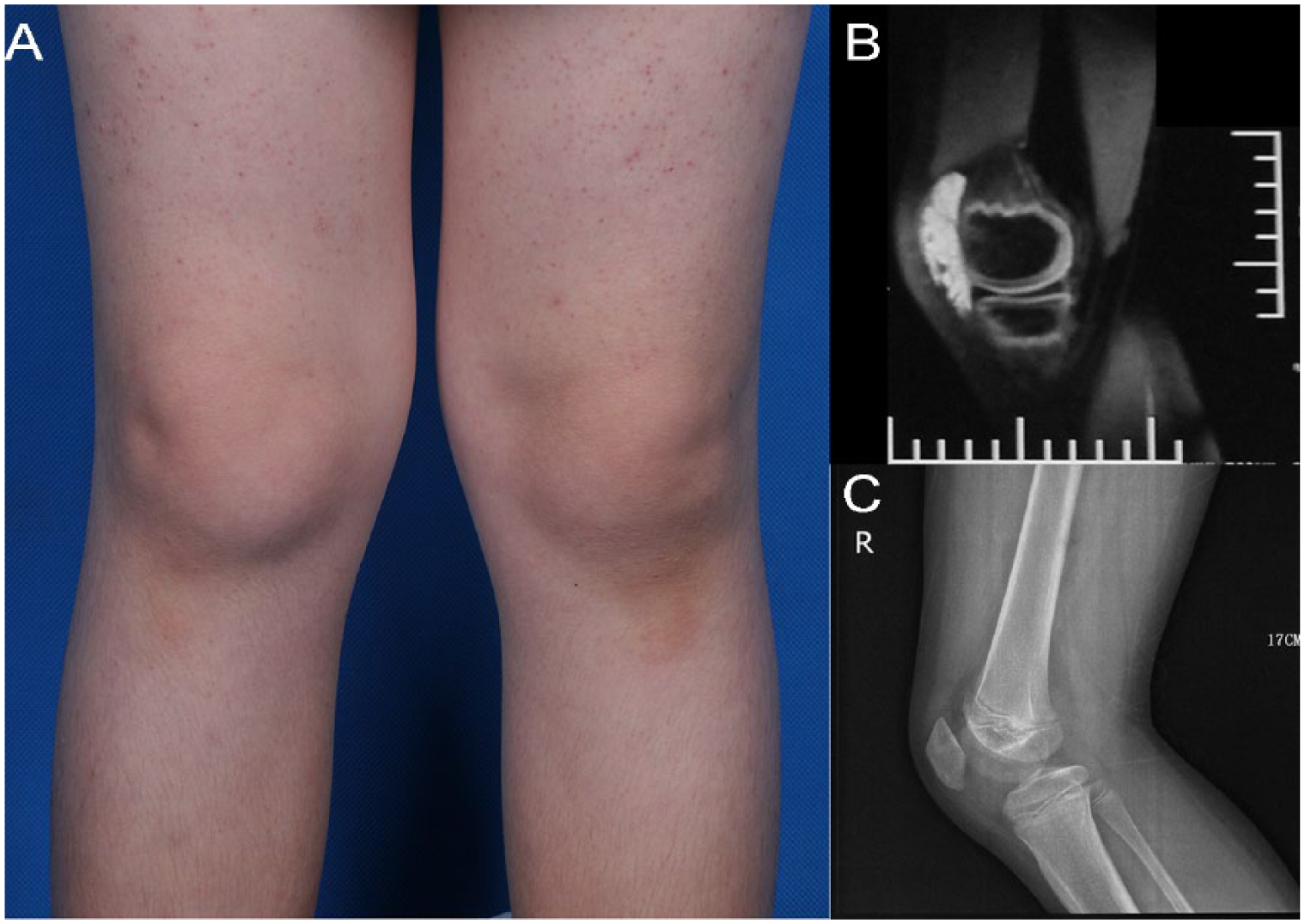
A 15-year-old male presented with a 1-month history of swelling of the right knee. The patient reported the swelling had improved over the last few days without receiving any treatment. (A) Physical examination revealed swelling of the right knee without symptoms of altered sensation, pain, or walking disabilities. (B) MRI demonstrated a well-defined vascular lesion around the joint, which was diagnosed as a venous malformation (type-II tissue involvement). (C) No phlebolith was found on the right knee X-ray.
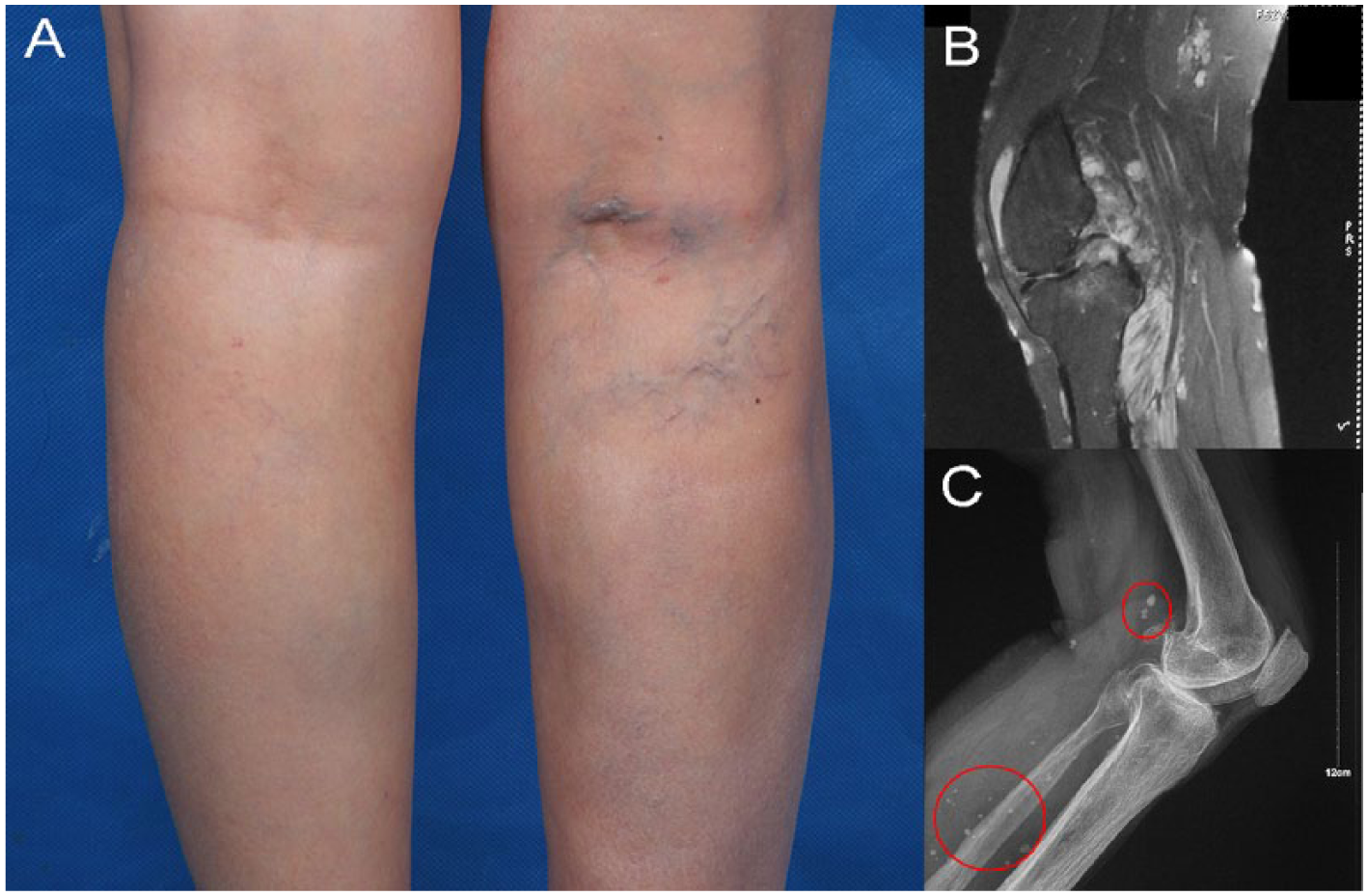
A 51-year-old female presented with a 20-year history of right popliteal swelling and pain. She underwent partial resection at a local hospital almost 15 years ago, without obvious benefit. The patient did not attach importance to the symptom until 2 years ago because of increased pain. The pain NRS score decreased from 5 to 2 after one session of sclerotherapy. (A) Physical examination revealed tenderness, swelling, and a dilated vein in the right popliteal space. (B) MRI showed an infiltrating venous lesion in the right knee and calf, suggesting type-II tissue involvement. (C) X-ray revealed multiple phleboliths (red circles) in the right popliteal and calf.
Clinical characteristics of patients in the painful group
A total of 125 (74.4%) patients who suffered from pain were included in the painful group. In our study, the pain intensity of four children (patient numbers 87, 97, 134, and 141) was evaluated by their parents. The median NRS score for pain reported by these patients was 4.0, with a mean score of 4.4 ± 2.0. The painful group included 76 females and 49 males with a mean age of 21.1 ± 12.2 years. The median age of these 125 patients was 20 years old. Overall, 37.6% and 62.4% of the lesions were located on the upper and lower extremities, respectively. The median value of the maximum cross-sectional area by MRI was 18.75 cm2. Type-I and type-II tissue involvement was identified by MRI in 9.6% and 90.4% of the 125 patients, respectively. Phleboliths were observed in 101 (80.8%) patients.
Risk factors for pain in venous malformations of the extremities
1) Sex: no sex difference was observed between the painful and painless groups (p = 0.817) (Table 1).
Univariate analysis between the painful and painless groups.
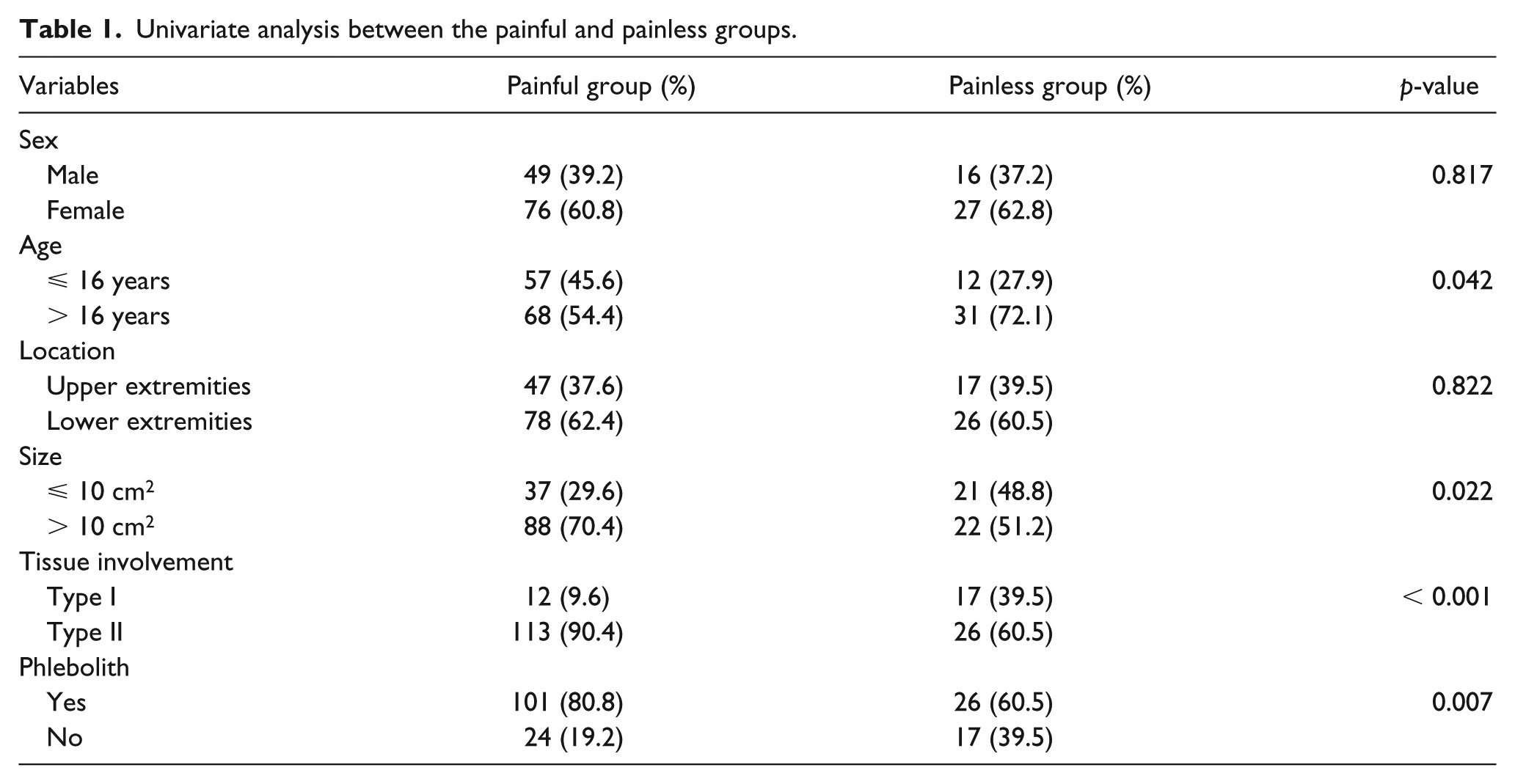
2) Age: univariate analysis revealed that pain was significantly associated with younger age; specifically, of the patients aged ⩽ 16 years, 57 were in the painful group and 12 were in the painless group (p = 0.042) (Table 1). However, we found that age did not remain significantly associated with pain in the multivariate analysis (p = 0.143) (Table 2).
Multivariate analysis performed in the two groups.
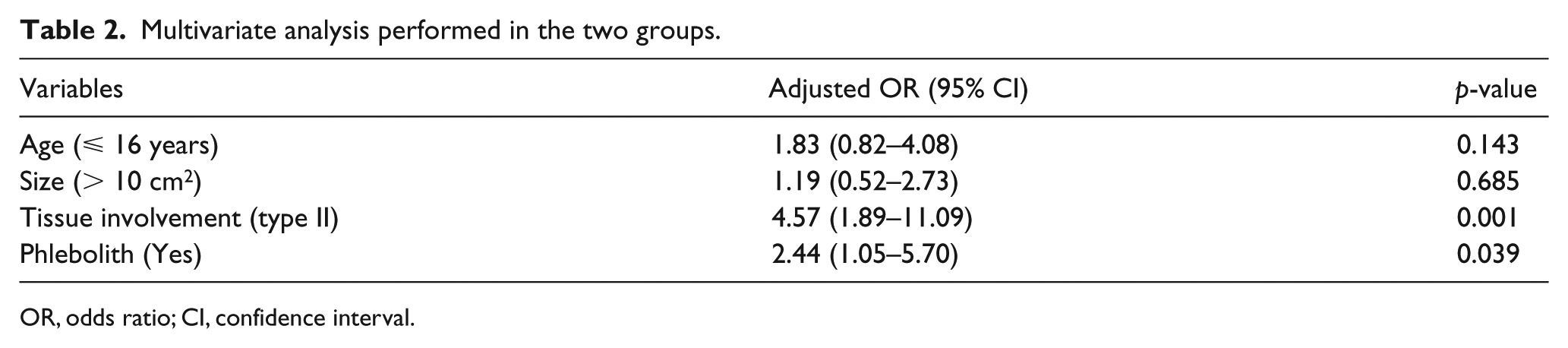
OR, odds ratio; CI, confidence interval.
3) Lesion location: there was no significant difference between the two groups (p = 0.822) (Table 1).
4) Lesion size: patients with lesions sized greater than 10 cm2 were significantly more likely to be in the painful group than in the painless group (p = 0.022) (Table 1). However, when adjusted for other risk factors, lesion size was not significantly associated with pain in the multivariate analysis (p = 0.685) (Table 2).
5) Tissue involvement: in the painful group, type-II (90.4%) tissue involvement was identified significantly more frequently than type-I (9.6%) tissue involvement (p < 0.001) (Table 1). When adjusted for other risk factors, the odds of pain were 4.57 times higher in patients with type-II than type-I tissue involvement (adjusted odds ratio (OR) = 4.57; 95% CI: 1.89–11.09; p = 0.001) (Table 2).
6) Phleboliths: pain was significantly more prevalent in patients presenting with phleboliths (p = 0.007) (Table 1). Furthermore, logistic regression analysis revealed that phleboliths were an independent risk factor associated with pain in patients with venous malformations of the extremities (adjusted OR = 2.44; 95% CI: 1.05–5.70; p = 0.039) (Table 2). Thus, patients with venous malformations of the extremities who presented with phleboliths had 2.4 times greater odds of pain.
Discussion
Pain caused by venous malformations is a common symptom. A previous study reported that 92% of 118 patients with venous malformations of the extremities and trunk experienced local pain. 15 In this study, we found that almost three-quarters of the 168 patients with limb venous malformations complained of pain, and then two risk factors independently associated with pain were identified: type-II tissue involvement and phleboliths.
Type-II tissue involvement
Type-II tissue involvement was defined as lesions involving muscle, bone or joint, with or without skin and subcutaneous involvement (see Supplemental Figure 1, which shows representative MRI slides of type-II tissue involvement).
First, intramuscular venous malformations have been found to be frequently associated with characteristic symptoms, and particularly pain upon exertion. 16 Hein et al. 17 reported that 20% of patients with intramuscular venous malformations experienced exertional pain. This type of pain is likely due to lesion engorgement resulting from venous pooling of blood during exercise. Shallow et al. 18 concluded that lesions located in long narrow muscles are more frequently associated with pain induction than lesions in wide, flat muscles, which provided greater room for expansion (as for the patient shown in Figure 2). Treatment of this type of pain usually starts with external compression of the venous malformations. It has been proven that polidocanol sclerotherapy is safe and efficacious in providing pain relief for patients with small venous malformations. 10 Another study showed that 93.5% (58/62) of patients with venous malformations reported pain improvement after sclerotherapy using absolute ethanol and bleomycin A5. 19 In future studies, the efficacy of different sclerosants can be compared in the pain relief for intramuscular lesions. The decision of whether to proceed with sclerotherapy is determined after careful consideration of symptom severity.
Second, intraosseous vascular malformations are slow-growing, benign abnormalities that account for less than 1% of all osseous ‘tumors’. 20 Bone changes, including shape, size, and density, are identified in approximately one-third of vascular malformations and found to often occur in long bones. 21 Intraosseous venous malformations of the extremities are frequently associated with demineralization and hypoplasia that can lead to structural weakening of the bone, deformity, and chronic pain.3,21 In addition, pain may result from the ability of these lesions to cause significant hemorrhage after relatively minor injury and subsequent subperiosteal hematoma. Treatment of intraosseous venous malformations of the extremities still remains a challenge for surgeons.
Third, accurate diagnosis of intra-articular venous malformations is often delayed as circumscribed forms of lesions are frequently mistaken for tumors or monoarthritis. 22 Among intra-articular venous malformations, knee venous malformations have been the most frequently reported in the literatures and patients can present with pain, swelling, motion impairment, and hemarthrosis.22–25 When associated with acute pain and swelling in the knee, these venous malformations are usually secondary to intralesional hemarthrosis caused by synovial involvement, whereas chronic pain can be caused by compromised muscle function and joint degeneration. 23 Regarding the treatment of knee venous malformations, it was suggested that early surgical excision of the lesions and synovectomy could be effective in protecting cartilage from further erosion. 22 A prospective study should be performed to investigate the long-term outcome of joint function postoperation.
Phleboliths
Phleboliths were another independent risk factor associated with painful venous malformations of the extremities. Dompmartin et al. 5 found that palpable phleboliths were presented in 61% of venous malformations; however, they considered the incidence of phleboliths to be likely underestimated because deep phleboliths were only observed upon radiological examinations. In our study, phleboliths were observed in 127 (75.6%) patients based on images. Remarkably, phleboliths in venous malformations of the head and neck have been found to occur less frequently (28.6%) and cause less pain compared with venous malformations of the extremities in a previous study. 14 Phleboliths could be removed through surgery if these contribute to the aggravation of pain.
Unlike exertional pain related to muscle involvement, the pain associated with phleboliths was often present when waking up in the morning. 15 A favored hypothesis suggests that slow blood flow predisposes to intralesional thrombosis, leading to phlebolith formation with subsequent stimulation of the pain pathways. 26 Phleboliths have also been demonstrated to be independently associated with localized intravascular coagulation. 5 Mazoyer et al. reported that patients with localized intravascular coagulation complained of more significant and prolonged episodes of pain and low-molecular-weight heparin was proven to be effective in reducing pain while decreasing D-dimer levels and restoring normal fibrinogen levels. 15 In addition, aspirin therapy was also demonstrated to be helpful in diminishing pain and swelling with limited complications. 27 We speculated that the treatment of localized intravascular coagulation associated with venous malformations of the extremities might be able to prevent the formation and progression of phleboliths. It would be necessary to conduct another prospective study to verify this theory.
Strengths and limitations
First, we had a large sample size of patients with venous malformations of the extremities in this study.3,13,15 Second, the blinding of assessors to symptoms and candidate risk factors can also be considered a strength of this study.
Limitations included that this study was retrospective in nature. In addition, statistical power was limited due to unbalanced sample sizes between the two groups.
Conclusions
This study indicated that the prevalence of pain in patients with venous malformation of the extremities was high. Type-II tissue involvement and phleboliths were demonstrated to be the two independent risk factors associated with pain. In future studies we aim to focus more on pain relief and we believe that recognition of the risk factors will help in choosing more precise and effective treatment for these patients.
Supplemental Material
10.1177_1358863X18802007_Supplementary_Material – Supplemental material for Risk factors associated with pain in patients with venous malformations of the extremities
Supplemental material, 10.1177_1358863X18802007_Supplementary_Material for Risk factors associated with pain in patients with venous malformations of the extremities by Li Hu, Hui Chen, Xi Yang, Yongying Wang, Hao Gu, Ming Liu and Xiaoxi Lin in Vascular Medicine
Footnotes
Acknowledgements
We would like to thank Dr Jingyan Yang from the Department of Epidemiology, Mailman School of Public Health, Columbia University, for her advice during the planning stages of the study, and Dr Ziming Zhang and colleagues from the Department of Radiology, Shanghai Ninth People’s Hospital, for assistance with the imaging review.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this study has received funding from the Clinical Research Plan of Shanghai Hospital Development Center (16CR1007A) and the Clinical Research Program of the Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine (JYLJ001).
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.