
Abstract
Impaired microvascular endothelial function may be implicated in the etiology of cognitive decline. Yet, current data on this association are inconsistent. Our objective is to investigate the relation of microvascular endothelial function to cognitive performance in the ELSA-Brasil cohort study. A total of 1521 participants from ELSA-Brasil free of dementia underwent peripheral arterial tonometry (PAT) to quantify microvascular endothelial function (PAT-ratio and mean baseline pulse amplitude (BPA)) and cognitive tests that covered the domains of memory, verbal fluency, and executive function at baseline. Cognitive tests in participants aged 55 years old and above were repeated during the second examination (mean follow-up: 3.5 (0.3) years). Linear regression and generalized linear models were used to evaluate the association between endothelial function, global cognitive performance, and performance on specific cognitive domains. In unadjusted cross-sectional analyses, we found that BPA and PAT-ratio were associated with worse global cognitive performance (mean difference for BPA: –0.07, 95% CI: –0.11; –0.03, p<0.01; mean difference for PAT-ratio: 0.11, 95% CI: 0.01; 0.20, p=0.02), worse performance on learning, recall, and word recognition tests (BPA: –0.87, 95% CI: –1.21; –0.52, p<0.01; PAT-ratio: 1.58, 95% CI: 0.80; 2.36, p<0.01), and only BPA was associated with worse performance in verbal fluency tests (−0.70, 95% CI: –1.19; –0.21, p<0.01). Adjustments for age, sex, and level of education rendered the associations statistically non-significant. Longitudinally, there was no association between microvascular endothelial and cognitive functions. The associations between microvascular endothelial function and cognition are explained by age, sex, and educational level. Measures of microvascular endothelial function may be of limited value with regard to preclinical cognitive deficits.
Introduction
Dementia is a huge burden to modern healthcare. 1 A key aspect of dementia is the long subclinical period prior to its clinical manifestation.2,3 Cognitive decline is a result of the progression of preclinical dementia and other non-normative aging processes that are not captured by chronological age. 4 Therefore, the assessment of cognition domains, such as memory, attention, and executive function, provides sensitive tools to identify the very earliest stages of dementia. 5 Within the multi-factorial etiology of cognitive decline and dementia, a role for vascular disease, specifically atherosclerosis, is increasingly being recognized, even in individuals without previous stroke.6–8
Endothelial dysfunction reflects vascular damage in an early stage of atherosclerosis, when the process of vascular damage is still potentially reversible. 9 An impaired endothelial function is characterized by decreased nitric oxide bioavailability, resulting in a vascular phenotype prone to inflammation, constriction and thrombosis.9–11 The relation of endothelial function with cognition could unravel important etiological insights that may contribute to the development of preventive interventions for neurodegenerative brain diseases.
Endothelial function has been extensively studied non-invasively by measuring the flow-mediated dilation of the brachial artery (FMD) due to reactive hyperemia. Reactive hyperemia is a response to ischemia due to an arterial occlusion that leads to hyperemic flow, which increases shear stress on the vascular wall and the subsequent release of nitric oxide. 9 Recently, the relationship between FMD and cognition in individuals without cerebrovascular disease was systematically reviewed. 12 Although the authors concluded that impaired FMD is associated with worse cognitive function, particularly executive, this association was not consistent across studies. 12
Another established method to assess endothelial function is peripheral arterial tonometry (PAT).9,10 PAT measures the response to reactive hyperemia in the microvasculature of the digits, has good reproducibility and is easier to implement in clinical practice.10,13 An impaired PAT response correlates with a greater burden of cardiovascular risk factors, particularly metabolically,11,14,15 and predicts cardiovascular events.16,17
Important questions regarding the association between endothelial function and cognitive performance remain unanswered. 12 First, the results of studies investigating this relationship are generally based on small samples, precluding the possibility to adequately model whether the results are independent of demographic and cardiovascular risk factors. 12 Second, most studies have been performed in selected patients with either known cardiovascular disease or cognitive complaints. Data from a population-based perspective remains scarce and inconclusive.18,19
Therefore, in a large sample of dementia-free, community-dwelling individuals from the ELSA-Brasil cohort study, we investigated the relationship between microvascular endothelial function and cognitive performance.
Participants and methods
Setting
This study is embedded within the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil), a multi-center cohort of 15,105 civil servants designed to investigate the determinants of cardiovascular diseases (CVDs) and diabetes.20,21 Eligibility criteria included active or retired employees of five universities and one research center, aged 35–74 years, who volunteered to participate. Exclusion criteria were: pregnancy, intention to quit work at the institution in the near future, severe cognitive or communication impairment, and, if retired, residence outside the center’s corresponding metropolitan area. The current study sample derived from the 3115 participants enrolled at the Minas Gerais Investigation Center, where peripheral arterial tonometry (PAT) data acquisition began partway through the baseline visit (2008–2010). From the 1695 participants who were eligible for PAT exams, 1535 participants had valid data. 11 At the baseline visit, participants also undertook cognitive tests. For the current study, we excluded participants with prior stroke (n = 14) given the influence on cognition, and our final sample size for cross-sectional analysis consisted of 1521 participants. A repeated assessment of cognitive performance in participants aged 55 years and above was done during the second examination (2012–2014) to assess change in cognitive performance (mean follow-up: 3.5 (0.3) years). As such, 752 participants were included in the longitudinal analysis. The Universidade Federal de Minas Gerais Ethics Committee approved the study and all participants provided written informed consent.
Assessment of endothelial function
Microvascular endothelial function was assessed at baseline using an automated device (EndoPAT2000; Itamar Medical, Israel). The reproducibility of PAT is comparable to other non-invasive methods used for endothelial function assessment. 13 The protocol used has been described elsewhere.11,13 In short, the cuff was placed on the participant’s non-dominant arm and PAT probes were placed on the index finger of both hands. Mean baseline pulse amplitude (BPA) was measured for 5 minutes. Next, arterial flow was interrupted on one side for 5 minutes by inflating the cuff to supra-systolic pressure. Then, the cuff was deflated to induce reactive hyperemia and the PAT signal was recorded. The contralateral finger was used to control for systemic changes. The PAT-ratio is calculated as the ratio of the post-deflation pulse amplitude 90–120 seconds after cuff release to the BPA. This result is divided by the corresponding ratio from the control finger and transformed to its natural logarithm. 11 BPA reflects the basal vascular tone and the PAT-ratio measures the vascular response to reactive hyperemia.10,11 A higher BPA and lower PAT-ratio are related to vascular disease phenotypes.11,14,15,22
Assessment of cognitive performance
Participants underwent cognitive tests from the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) to assess cognitive function. 23 The tests included word learning, recall and recognition tests, a test on retrieval from verbal memory, and recognition of verbal memory. The semantic (animal category at baseline and vegetables at follow-up visit) and phonemic (letter F at baseline and letter A at follow-up visit) verbal fluency tests were used to evaluate the efficiency of searching in long-term memory and language. 24 The trail-making test B was used to evaluate executive function. 25 The baseline results of cognitive performance in the ELSA-Brasil cohort study have already been published. 26 The reliability of these tests varied from moderate, for the learning and word recall test (kappa = 0.56; 95% CI 0.33–0.79), to very good, for the trail-making test B (kappa = 0.91; 95% CI 0.87–0.95). 27 For all tests except the trail-making test B, a higher score represents a better cognitive performance. To allow direct comparisons, we inverted the trail-making test B scores. We calculated a general cognitive factor (g-factor) using a principal component analysis incorporating all tests. For tests with multiple subtasks, we chose only one subtask in order to prevent highly correlated tasks from distorting the factor loadings. Principal component analysis was performed on the complete case data of 1483 persons. The g-factor was identified as the first unrotated component of the principal component analysis and explained 57% in the baseline and 60% in the follow-up visit of all variance in the cognitive tests – a typical amount of variance for the g-factor. 28
Assessment of other covariates in ELSA-Brasil
All the covariates included in the analysis were assessed at baseline and were self-reported through standardized questionnaires, obtained through clinical procedures, or laboratory measurements.20,21 Level of education was the highest qualification attained and categorized as graduate school or more, complete high school, and complete and incomplete elementary school. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared. Systolic and diastolic blood pressures were measured three times in a sitting position after 5 minutes of rest. The average of the second and third measurements was used in the analyses. Blood samples were collected in the fasting state and 2 hours after oral administration of 75g of glucose. Diabetes was defined as a fasting glucose ≥ 126 mg/dL, glucose ≥ 200 mg/dL after a tolerance test, hemoglobin A1c ≥ 6.5%, and self-reported diabetes or treatment with insulin or a hypoglycemic agent. Serum total cholesterol and high-density lipoprotein (HDL)-cholesterol were measured using an enzymatic colorimetric assay (ADVIA Chemistry, Munich, Germany). Smoking was categorized as never, former and current smoking. Self-reported alcohol intake was categorized in never or former user, and moderate and heavy consumption. Prevalent cardiovascular disease was defined as the self-reported presence of previous myocardial infarction/revascularization and heart failure. Medication use in the last 12 months of neuroleptics and/or anticonvulsants and/or anticholinesterase and/or antiparkinsonian was recorded by interview and grouped as ‘yes’ and ‘no’.
Statistical analyses
Characteristics of the study population are presented as unadjusted means with standard deviations or medians with interquartile ranges for continuous variables, and as percentages for categorical variables. To investigate the association between endothelial function and cognitive performance, we used multiple linear regressions for global cognition, learning and recall word recognition tests, and semantic and phonemic verbal fluency tests. For the analyses of the seconds taken to complete the trail-making B test, we used a generalized linear model (GLM) with logarithmic link and gamma distribution because of the variables’ skewed distribution. 29 We performed unadjusted analysis between the measures of endothelial function (PAT-ratio and BPA) with global cognition and each cognitive function test separately (model 1). Thereafter, associations were adjusted for sex, age and educational attainment (model 2). Finally, we additionally adjusted for BMI, systolic blood pressure, use of anti-hypertensive medication, diabetes mellitus, total/HDL cholesterol ratio, smoking, alcohol intake, prevalent cardiovascular disease, and use of neuroleptics (model 3). We repeated the analyses of Model 3, using PAT measures in tertiles to assess non-linear associations between PAT measures and outcomes. As a secondary analysis, we evaluated the associations between PAT measures and cognition stratified by sex and age <64 or ≥65 years. For longitudinal analyses, we considered the cognitive tests’ results of the follow-up visit as outcome and adjusted the models for the specific test score at baseline. We adjusted the models as described above, and additionally for the time interval between the tests. Two-sided p-values <0.05 were considered statistically significant. Analyses were conducted using Stata 13.0 software (StataCorp LP, College Station, TX, USA).
Results
Table 1 demonstrates the characteristics of the study population. The mean age was 51.9 (± 8.5) years at baseline and 61.9 (± 5.4) years in the follow-up visit, 44% were women and most participants had a high level of education (64%). Table 2 shows the cross-sectional associations between endothelial function measurements and performance in the cognitive function tests. We found that BPA and PAT-ratio were associated with worse global cognitive performance in the unadjusted model (model 1) (mean difference: –0.07, 95% CI: –0.11; –0.03). After adjusting for age, sex, and level of education (model 2), the associations were no longer statistically significant (mean difference: 0.02, 95% CI: –0.02; 0.05).
Characteristics of participants (n=1521).
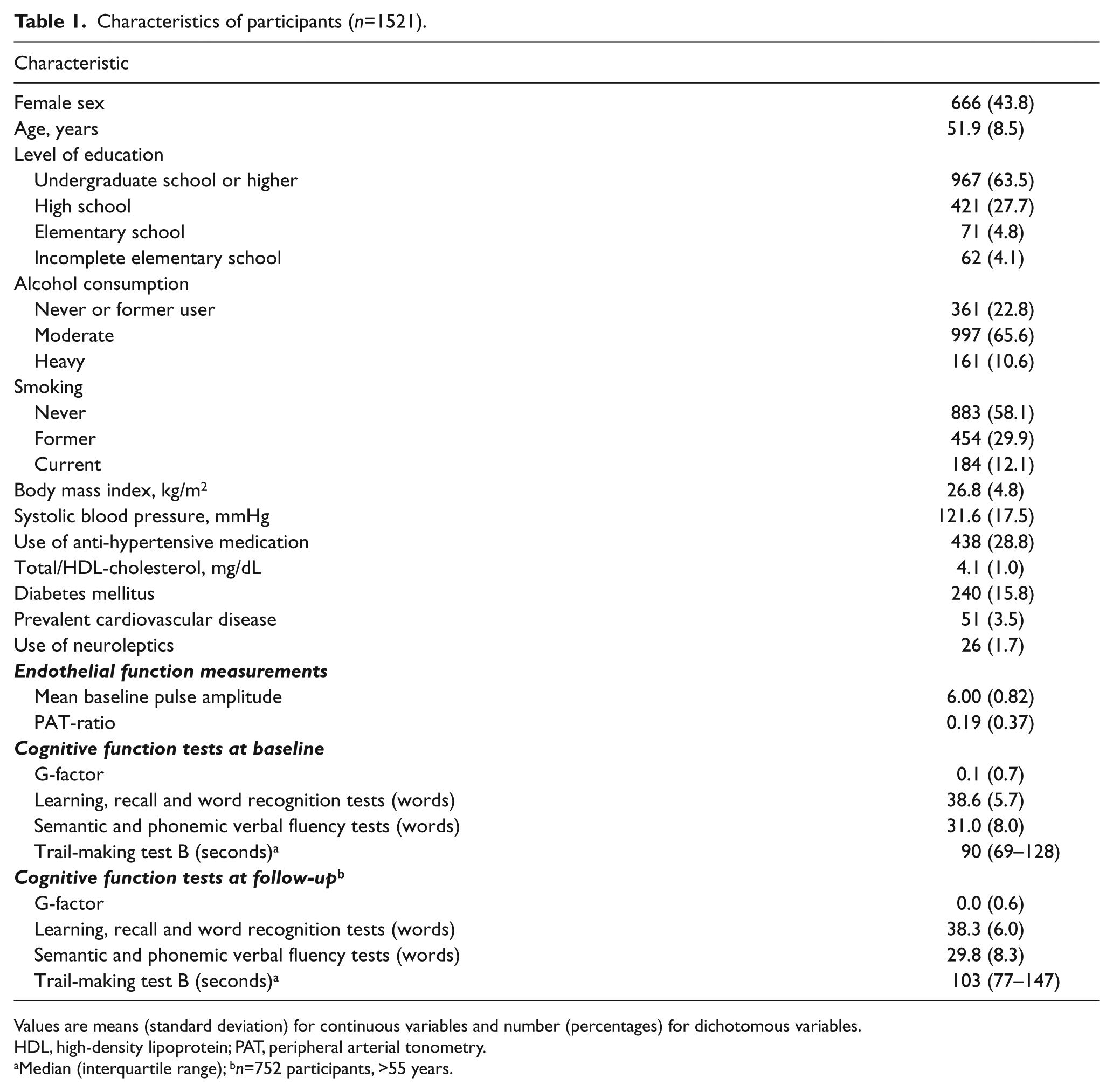
Values are means (standard deviation) for continuous variables and number (percentages) for dichotomous variables.
HDL, high-density lipoprotein; PAT, peripheral arterial tonometry.
Median (interquartile range); bn=752 participants, >55 years.
Cross-sectional association between endothelial function and cognitive performance.
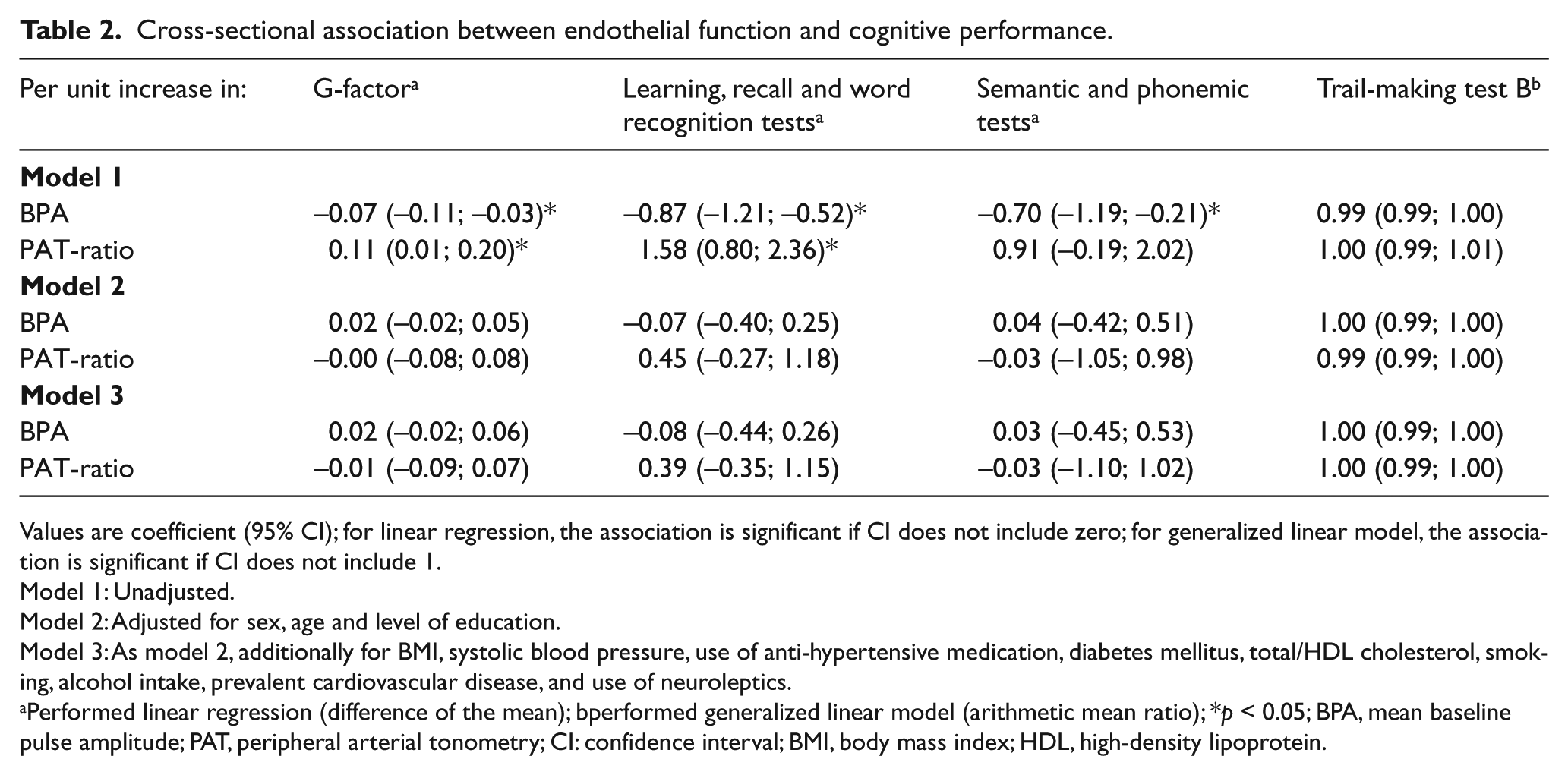
Values are coefficient (95% CI); for linear regression, the association is significant if CI does not include zero; for generalized linear model, the association is significant if CI does not include 1.
Model 1: Unadjusted.
Model 2: Adjusted for sex, age and level of education.
Model 3: As model 2, additionally for BMI, systolic blood pressure, use of anti-hypertensive medication, diabetes mellitus, total/HDL cholesterol, smoking, alcohol intake, prevalent cardiovascular disease, and use of neuroleptics.
Performed linear regression (difference of the mean); bperformed generalized linear model (arithmetic mean ratio); *p < 0.05; BPA, mean baseline pulse amplitude; PAT, peripheral arterial tonometry; CI: confidence interval; BMI, body mass index; HDL, high-density lipoprotein.
When investigating the specific cognitive tests, we found that BPA and PAT-ratio were associated with worse cognitive performance on learning, recall and word recognition tests (BPA: –0.87, 95% CI: –1.21; –0.52; PAT-ratio: 1.58, 95% CI: 0.80; 2.36), and only BPA was associated with semantic and phonemic fluency tests (mean difference: –0.70, 95% CI: –1.19; –0.21). However, adjustments for sex, age, and educational level (model 2) made the associations become statistically non-significant. Additional adjustment for cardiovascular risk factors (model 3) using BPA and PAT-ratio in tertiles (Supplementary Table 1) and stratifying by age and sex (data not shown) did not provide novel insights. In the longitudinal analysis, endothelial function measurements were not associated with global cognition or with any cognitive domain (Table 3).
Longitudinal association between endothelial function and cognitive performance.
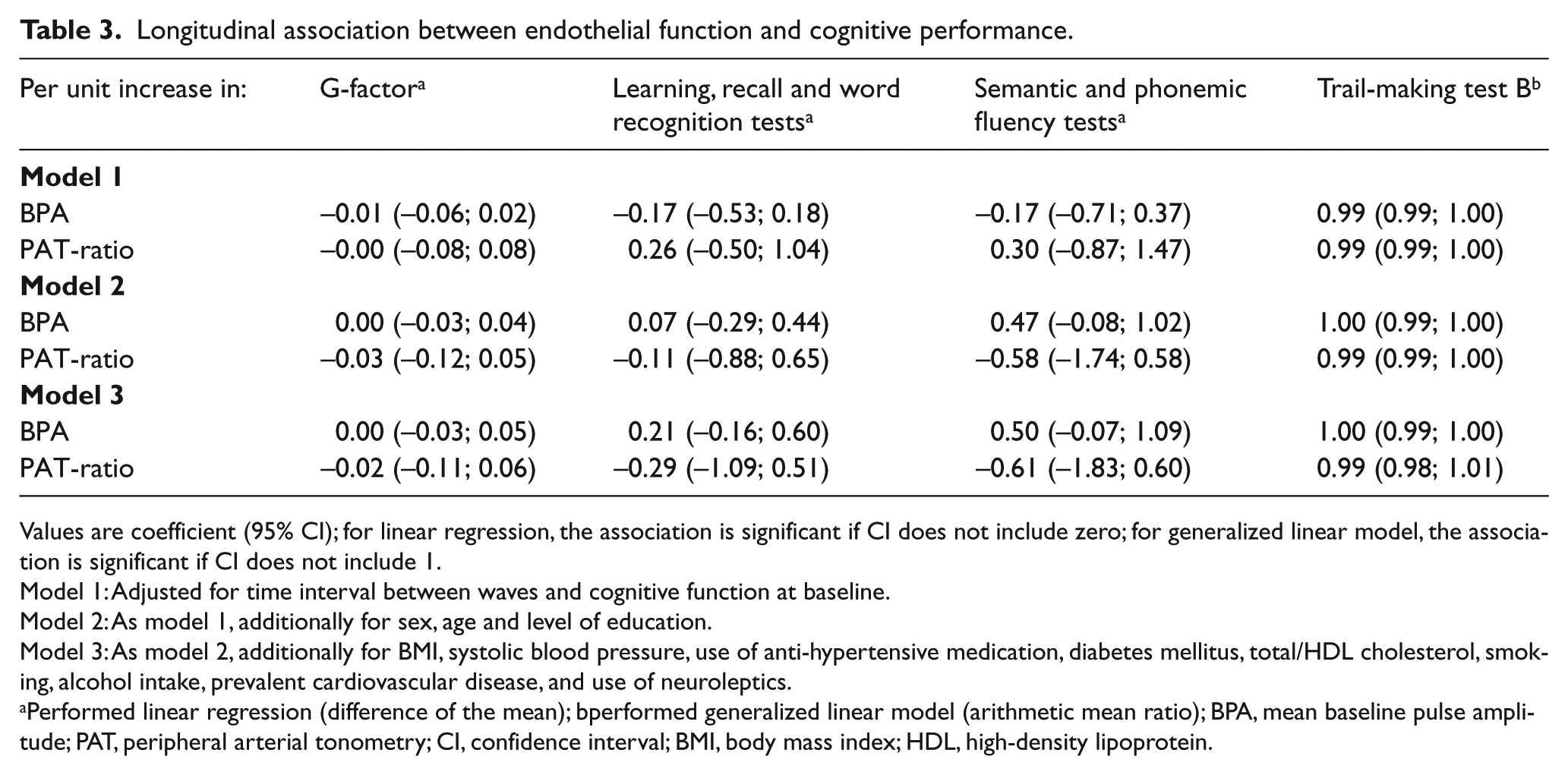
Values are coefficient (95% CI); for linear regression, the association is significant if CI does not include zero; for generalized linear model, the association is significant if CI does not include 1.
Model 1: Adjusted for time interval between waves and cognitive function at baseline.
Model 2: As model 1, additionally for sex, age and level of education.
Model 3: As model 2, additionally for BMI, systolic blood pressure, use of anti-hypertensive medication, diabetes mellitus, total/HDL cholesterol, smoking, alcohol intake, prevalent cardiovascular disease, and use of neuroleptics.
Performed linear regression (difference of the mean); bperformed generalized linear model (arithmetic mean ratio); BPA, mean baseline pulse amplitude; PAT, peripheral arterial tonometry; CI, confidence interval; BMI, body mass index; HDL, high-density lipoprotein.
Discussion
In this large population-based sample of individuals free of dementia, we found that both impaired BPA and PAT-ratio are only cross-sectionally associated with worse performance on global cognitive function, memory, and phonemic fluency in the crude analysis. However, these associations lost significance after adjustment for age, sex, and level of education. Considering the early manifestation of endothelial dysfunction in atherosclerosis, we then stratified the PAT results in tertiles to investigate non-linear associations between endothelial function and cognition; however, this analysis provided no further insights.
There are plausible mechanisms for the association of endothelial dysfunction with cognitive decline. 30 Neurovascular dysfunction, resulting from oxidative stress and inflammation, increases the chance of brain injury, mainly by causing alterations in the regulation of cerebral blood flow. 30 However, prior studies that have described the association of endothelial and cognitive functions in patients without cerebrovascular disease demonstrated conflicting results. 12 In the Framingham Offspring Study, 1587 stroke and dementia-free participants were evaluated and the authors concluded that there was no significant relationship between endothelial measures and brain structure or executive function. 18 Conversely, in a systematic review recently published (n=2791), the authors state that there are links between vascular function and cognition – particularly for executive tasks. 12
Our results add to the controversy, as we demonstrated that in a large community-based population free of dementia or prior stroke, microvascular endothelial function was not related to cognitive performance, even longitudinally. This finding suggests that vascular damage associated with cognitive impairment might not be mediated by endothelial dysfunction, or endothelial dysfunction may be a too early marker of atherosclerosis and thus precede the changes in cognitive function. We hypothesized that the significant associations previously described in other small studies12,19 may be explained by the selected samples or by the effect of confounders. In fact, the associations of PAT measurements to global cognition, memory, and phonemic tests that we found in the crude models seemed to be driven by sex, age and level of education.
Alternatively, it may be that endothelial function evaluated in the microvasculature is not related to cognitive performance in a young population or even in a short time of follow-up. Most studies published so far in this topic evaluated endothelial function by flow-mediated dilation of the brachial artery – a conduit vessel, while PAT evaluates responses in the microvasculature of the digits. Previous work shows that the evaluation of vascular function in different beds may provide distinct information,15,31 and data from large cohort studies demonstrated that brachial and digital measures of vascular function have different relations with cardiovascular risk factors. While an impaired FMD is more strongly related to advancing age and hypertension, an impaired PAT response is related to metabolic risk factors, such as obesity and diabetes.15,31
We hypothesized that impaired PAT measurements would be related to worse cognitive performance because alterations of the brain microvasculature is related to neurocognitive decline. 30 Indeed, pathologic studies of the brain have demonstrated atherosclerosis of microvessels in regions with white matter hyperintensity diagnosed by MRI – a known factor predisposing to dementia.30,32 Moreover, impaired PAT responses are consistently associated with metabolic risk factors, as already cited, and cardiovascular outcomes,16,17 both related to cognitive impairment.
A second explanation for our negative findings is that microvascular function measured in a different site, such as the digits, may not reflect the vascular injury of the brain microvasculature, even though it is known that endothelial dysfunction is a systemic process. 9 Future studies evaluating vascular function in the cerebral bed using neuroimaging may help to elucidate whether local vascular dysfunction has a role in cognitive decline.
Strengths and limitations
Strengths of our study include the large population-based sample, the standardized assessment of endothelial function with a method that is linked to vascular disease, and the possibility to adjust for a broad spectrum of cardiovascular risk factors. However, some limitations should be addressed. First, the cross-sectional design of the current study prevents inferences on causality. Second, the mean age of the population is relatively low and the level of education high, resulting in an overall relatively good cognitive performance. This fact may have reduced the ability of finding statistically significant associations, as the variability of the cognitive test results was low. Third, the short follow-up time might have been too short to capture changes in cognitive performance. Lastly, the moderate reproducibility of PAT 13 and some of the cognitive tests 26 may have attenuated the associations towards the null hypothesis, although we believe we still had power to study the associations.
Conclusion
Impaired endothelial function evaluated in the microvasculature is only cross-sectionally associated with worse performance on global cognition, memory, and phonemic domains. However, the major proportion of the associations cited is explained by sex, age, and educational level. Measures of microvascular endothelial function may therefore be of limited value in the evaluation of cognition.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The ELSA-Brasil baseline study was supported by the Brazilian Ministries of Health and of Science and Technology (grants 01060010.00RS, 01060212.00BA, 01060300.00ES, 01060278.00MG, 01060115.00SP, and 01060071.00RJ). This ancillary study was supported by FAPEMIG (Minas Gerais, Brazil). ALPR and SMB are recipients of an award for established researchers from Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq). ALPR is also supported by a research grant (Pesquisador Mineiro) from Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG), the research agency of the State of Minas Gerais, Brazil. DB is supported by a grant from the Royal Netherlands Academy of Arts and Sciences (Van Leersum grant, 2015). LFA received a doctoral scholarship from FAPEMIG and was a research fellow of Coordenação de Aperfeiçoamento de Pessoal de NívelSuperior (CAPES), grant no. 99999.002279/2014-02, as a visiting scholar at Erasmus University Medical Center in Rotterdam, The Netherlands. LFA received a postdoctoral scholarship from CNPq (grant no. 150248/2015-6).
None of the funders had any role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.