
Abstract
Thrombosis of the inferior vena cava and iliac veins, known as iliocaval thrombosis, is a common cause of significant morbidity. Patients with chronic iliocaval obstruction often present with life-limiting occlusive symptoms secondary to recurrent lower extremity deep venous thrombosis, swelling, pain, venous stasis ulcers, or phlegmasia. Endovascular iliocaval reconstruction is a technically successful procedure that results in favorable clinical outcomes and stent patency rates with few complications and is often able to relieve debilitating symptoms in affected patients. This review presents an approach to endovascular iliocaval stent reconstruction in patients suffering from chronic iliocaval thrombosis, including background, patient selection, timing of intervention, procedural steps, technical considerations, patient follow-up, and a brief review of outcomes. Schematic illustrations and clinical cases outlining iliocaval stent reconstruction and crossing chronic venous occlusions have been provided.
Keywords
Introduction
Chronic thrombosis of the inferior vena cava (IVC) and iliac veins, known as chronic iliocaval thrombosis, is a common cause of significant morbidity.1–9 Patients with iliocaval obstruction often present with life-limiting occlusive symptoms secondary to recurrent lower extremity deep venous thrombosis, swelling, pain, venous stasis ulcers, or, in rare instances, phlegmasia.1–9 Reconstruction of the iliocaval venous system by recanalization, angioplasty, stent placement, and restoration of in-line flow may provide significant symptomatic relief with minimal patient morbidity.1–9
Preprocedural considerations
Clinical evaluation
Gathering relevant patient history, performing a focused clinical and physical examination, and closely reviewing imaging studies are all necessary steps to guide clinical decision making with respect to iliocaval stent reconstruction. While obtaining a history, the interventionalist should elicit the time course of symptoms (days, weeks, or months), any functional impairment related to the suspected venous occlusion, comorbidities that may affect anesthesia or treatment options, anticoagulation history, and review any prior interventions performed on the patient that may complicate iliocaval stent reconstruction (e.g. IVC filter placement, surgical history complicating vascular access, and personal or family history of thrombophilia).2,5 Physical examination may reveal the extent of venous disease and provide some objective evidence of functional status. A set of laboratory investigations should be obtained prior to the reconstruction procedure, including a complete blood count, standard anticoagulation studies (platelets and international normalized ratio), and a basic metabolic panel to assess hydration and renal function. Additionally, documentation of a physician generated measurement tool (including the clinical, etiology, anatomy, pathophysiology (CEAP) classification; the Venous Severity Scoring system; the 36-Item Short Form Health Survey; or the Nottingham Health profile) is important to document on initial presentation. These measurements allow documentation of clinical changes over time.
Imaging
A thorough review of all imaging studies is paramount in determining the extent of venous disease, presence of anatomic anomalies, and assists in preprocedural planning. Ultrasonography may demonstrate femoral vein and peripheral lower extremity thrombosis, whether acute or chronic. Computed tomography venography (CTV) or magnetic resonance venography (MRV) may demonstrate central iliocaval thrombosis and may play a critical role in preprocedural planning. CTV or MRV are particularly important if sharp recanalization procedures are anticipated.
Indications
Iliocaval reconstruction should be performed in patients with chronic iliocaval occlusion who have recurrent deep venous thrombosis, severe post-thrombotic syndrome, or related symptoms that restrict normal activity or significantly reduce quality of life. Ideally, treatment of iliocaval thrombosis should be initiated within 2 weeks of onset in the acute setting or after 4 months for chronic occlusion. 2 While chronic thrombosis is defined as being older than 2 weeks, the occlusion at this time is still large and bulky, and may limit balloon dilation and stent placement. Thus, treating the patient medically with compression stockings, anticoagulation, and frequent ambulation until the thrombus matures and scars down the vein, at approximately 4 months, may allow for easier recanalization and reconstruction. While this time frame should guide intervention, it is not rigid, and clinical judgment should guide the interventionalist as to whether patients may be medically managed if they present outside of the ideal treatment window. There is no occlusion too old to contraindicate recanalization and reconstruction.
Anticoagulation
Often, patients with chronic iliocaval thrombosis present while on anticoagulation. Owing to the theoretical risk for creation of false passages during guidewire manipulation and recanalization, and consequently risk for hemorrhage, the authors hold anticoagulation prior to iliocaval reconstruction. Aside from aspirin, it is the authors’ practice to hold all anticoagulation and antiplatelet agents prior to iliocaval reconstruction, if possible. Specifically, the authors hold clopidogrel and warfarin for 5 days prior to intervention; fondaparinux, rivaroxaban, and apixaban for 3 days prior to intervention; enoxaparin for 24 hours; and heparin infusion for 2 hours prior to the procedure.
Equipment
The preferred equipment for iliocaval stent reconstruction includes standard micropuncture sets for bilateral great saphenous vein or common femoral vein and internal jugular vein accesses, 6-French and 8-French sheaths, vertebral tip (angled) and flush catheters, hydrophilic guidewires such as the Glidewire (Terumo Corporation, Shibuya, Japan), high-pressure balloons, and possibly a loop snare device to begin recanalization. When sharp recanalization is required, a variety of devices including BRK transseptal (St Jude Medical, Saint Paul, MN, USA), Chiba (Cook Medical, Bloomington, IN, USA), and Rösch-Uchida (Cook Medical, Bloomington, IN, USA) needles may be considered. Additionally, intravascular ultrasound may be useful for detecting residual mural thrombus, proximity to adjacent critical structures, and for determining stent sizes.2,10
Regarding stenting, there are currently no Food and Drug Administration approved stents, and all stents are used off-label. Large diameter, self-expanding stents, however, are needed for the iliocaval system (12–24 mm) and thus the Wallstent (Boston Scientific, Marlborough, MD, USA) is favored by many endovascular experts. 11 Larger sheath sizes may be required to accommodate some self-expanding stents, though most interventions may be performed with a 10-French sheath, which may accommodate up to a 20 mm Wallstent. A 12-French sheath, however, may be needed in rare instances to place 24 mm Wallstents. For closure, manual compression, a pressure assisted closure device, or suture are effective options.
Procedural steps
Anesthesia
While both conscious sedation or general anesthesia are appropriate for recanalization of chronic iliocaval thrombosis, general anesthesia is often preferred as pain from balloon dilation of stenosed vein segments may be severe. If conscious sedation is used, care should be taken by the anesthesia staff to maintain a level of sedation sufficient for patient comfort while maintaining the patient’s ability to follow commands, as breath holds improve the quality of diagnostic venography.
Vascular access
Following induction of conscious sedation or general anesthesia, the preferred route of access is via the right internal jugular vein and bilateral common femoral veins under ultrasound guidance. Great saphenous vein access is an alternative to common femoral vein access. The authors prefer bilateral great saphenous vein access as the more superficial location may theoretically promote shorter hemostasis times in the setting of anticoagulation, although this has not been published. Though great saphenous vein access may be considered an atypical approach, the authors have utilized great saphenous access using sheath sizes ranging from 3- to 16-French, without complication. Popliteal access may also be obtained when more caudal access is required; however, full anticoagulation is a crucial step immediately following reconstruction, and hemostasis is often more difficult to achieve post-procedurally with deeper puncture sites. However, all of these access sites are viable options for iliocaval reconstruction.
Recanalization
Following common femoral vein or great saphenous vein and internal jugular vein access, a 6-French sheath should be advanced into the common femoral vein or great saphenous vein followed by a vertebral catheter and hydrophilic guidewire (the authors prefer the straight, stiff Glidewire). Following successful access, contrast digital subtraction angiography images are acquired to determine the extent of occlusion and the pathway for iliocaval recanalization. It is advantageous to perform recanalization in a peripheral to central fashion so that subsequent contrast injections will enhance an often-present thin iliocaval conduit and guidewire advancement. Identification of this channel may be difficult to identify among the many collateral vessels. 2
Recanalization may be a tedious process that is fraught with trial and error. Advancement of the guidewire through the apparently correct pathway may terminate prematurely. At this point the catheter and guidewire should be retracted and re-directed in an attempt to cannulate an alternative route. Exploring multiple routes may require alternating between left and right common femoral vein or great saphenous vein accesses.
There are several techniques that may be employed in the recanalization of venous occlusions. The simplest technique is blunt recanalization using a guidewire and catheter to probe through the occlusion until both proximal and distal wires meet head-on in a similar lumen (Figure 1A). At this point, no complex manipulation is required and through-and-through access of the lumen may be attempted with a loop snare device (Figure 1B). Additionally, hydrophilic crossing catheters such as vertebral tip (angled), Navicross (Terumo, Shibuya, Japan), or Quick-Cross catheters (Spectranetics, Colorado Springs, CO, USA) may be effective at navigating through chronic obstructions by advancing the sheath, catheter, and wire serially in a sequential fashion.
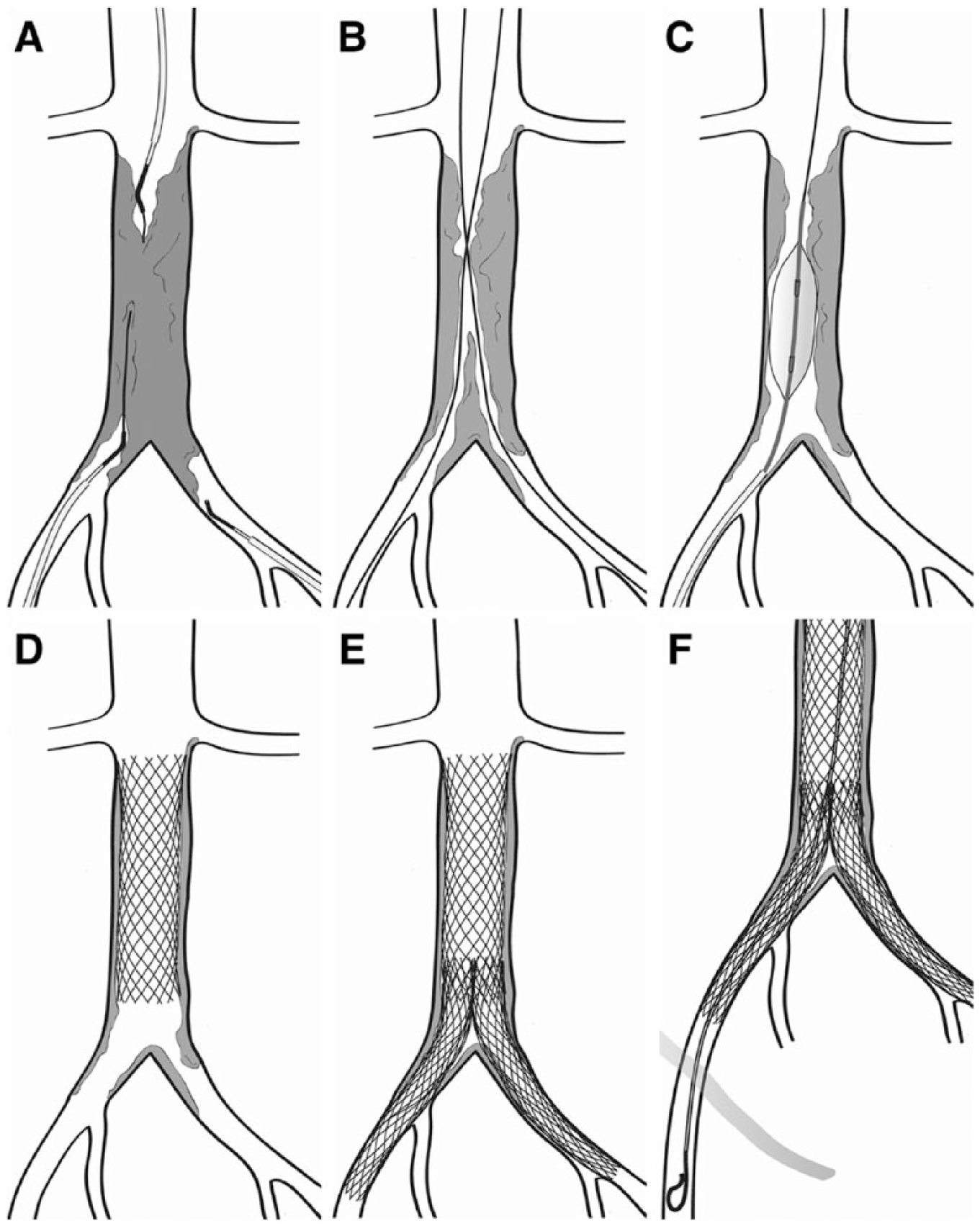
Schematic illustration depicting the basic steps of iliocaval recanalization and stenting. Complete chronic occlusion of the infrarenal inferior vena cava is present. (A) Bilateral saphenous vein access with Glidewire (Terumo Corporation, Shibuya, Japan) recanalization through the occluded segment. (B) Through-and-through access from the internal jugular vein through both femoral veins. (C) Balloon venoplasty. (D) Wallstent (Boston Scientific, Marlborough, MD, USA) placement in the inferior vena cava. (E) Wallstents in bilateral common iliac veins. (F) Completion venogram with flush catheter in the common femoral vein to evaluate inflow.
A more challenging scenario is when the proximal and distal wires are in proximity, but their paths do not communicate. If encountered, there are several options available to the interventionalist to allow for successful recanalization. Sharp recanalization of the obstruction separating the proximal and distal wires using a loop snare and recanalization needle or re-entry device may be attempted (Figure 2A–C). Alternatively, side-by-side dilation using an 8–10 mm diameter balloon in the IVC or 6 mm diameter balloon in the iliofemoral segment may be attempted to create a common channel between the proximal and distal wires, after which a loop snare device may be used to pull a wire across the obstruction.
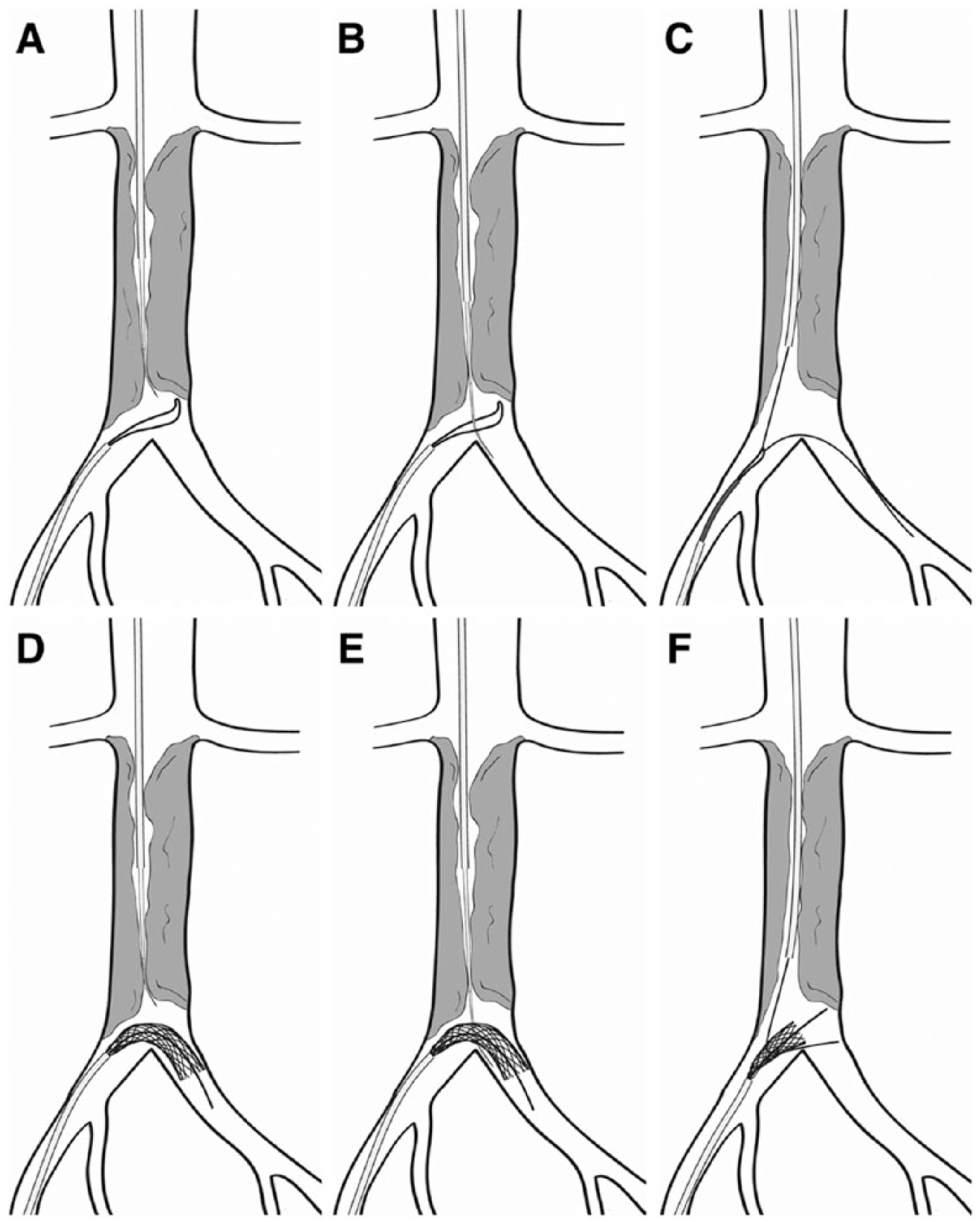
Schematic illustration depicting sharp recanalization and three-dimensional targeting. Complete chronic occlusion of the infrarenal inferior vena cava is present. (A) Sharp recanalization with a BRK needle (St. Jude Medical, Saint Paul, MN, USA) advanced through the obstructed segment of the caudal inferior vena cava. (B) The BRK needle is successfully advanced through a loop snare. (C) The wire through the loop snare device is captured, thereby achieving through-and-through access. (D). Sharp recanalization with a BRK needle advanced through the obstruction. A Wallstent (Boston Scientific, Marlborough, MD, USA) is partially deployed in the caudal inferior vena cava across the bifurcation in order to provide a larger target for sharp recanalization. (E) The BRK needle is advanced through the partially deployed Wallstent. (F). The wire is advanced through the Wallstent and is then recaptured and removed, thereby achieving through-and-through access.
If the chronic venous occlusion cannot be traversed using either blunt or sharp recanalization, three-dimensional targeting of a Wallstent Endoprosthesis (Boston Scientific) or AMPLATZER Vascular Plug (St Jude Medical) may be attempted as described by Khaja et al. 12 In this technique, rather than targeting a loop snare device with a transseptal needle, a Wallstent Endoprosthesis or AMPLATZER Vascular Plug may be partially deployed within a patent portion of the occlusion opposite the transseptal needle, which also expands the target segment (Figure 2D). Using rotational fluoroscopy, the partially deployed device may be targeted and punctured (Figure 2E). At this point, a 0.018-inch V-18 guidewire may be advanced through the interstices of the device before retracting the transseptal needle and retracting the device deployment sheath (Figure 2F). This creates through-and-through access after the device is pulled through the access sheath. 12
Thrombectomy devices
If there is acute or subacute thrombus present, or thrombus develops intraprocedurally, a variety of ancillary catheter-based pharmacomechanical and mechanical thrombectomy devices are available. Pulse-spray or overnight catheter-directed thrombolysis with tissue plasminogen activator (Alteplase; Genentech, San Francisco, CA, USA) can be performed using the EkoSonic ultrasound-enhanced thrombolysis system (EKOS / BTG, London, UK) or standard infusion catheters such as the UniFuse (Angiodynamics, Latham, NY, USA) and Cragg-McNamara (Covidien Ltd, Dublin, Ireland) multi-sidehole infusion catheters. Pharmacomechanical thrombectomy can be performed using the AngioJet Rheolytic Thrombectomy System (Boston Scientific) and the Trellis device (Covidien; previously discontinued). Pure mechanical thrombectomy devices include the Arrow-Trerotola Percutaneous Thrombectomy Device (Teleflex Inc., Wayne, PA, USA), Cleaner 15 and Cleaner XT (Argon Medical, Plano, TX, USA), the Indigo System (Penumbra, Alameda, CA, USA), and the AngioVac Aspiration Thrombectomy Device (Angiodynamics); however, this requires large sheaths (17-Fr and 22-Fr) and may require coordination with a perfusion team. This device may work well for the removal of large volume caval thrombus. However, any of these devices may assist with acute or subacute thrombus removal. 13
Restoration of the lumen
Following recanalization of the obstructing thrombus or scarred vein, the tract must be interrogated prior to balloon angioplasty and stenting to ensure the tract does not communicate with nearby arteries or terminate within the retroperitoneal space. Contrast injections, carbon dioxide injections, or intravascular ultrasound are all appropriate methods for evaluation. Once integrity of the tract has been confirmed, advancement of an 8-French sheath will be required for subsequent large balloon dilation (Figure 1C). If the tract will not accommodate an 8-French sheath, pre-dilation with a 4–6 mm high-pressure balloon may facilitate advancement of the sheath. At this point the IVC may be sequentially dilated to 18–20 mm, the common iliac vein to 16 mm, and the iliofemoral segment to 14 mm. If the recanalized lumen contains residual thrombus there should be a low threshold for stenting to prevent re-thrombosis. Self-expanding stents are preferred. The authors prefer to stent the caudal IVC with a buttressing stent with subsequent iliocaval stenting in a ‘kissing’ fashion (Figures 1D and 1E). Residual thrombus may be visualized directly by intravascular ultrasound or outlined by contrast. See the case examples in Figures 3, 4, and 5.
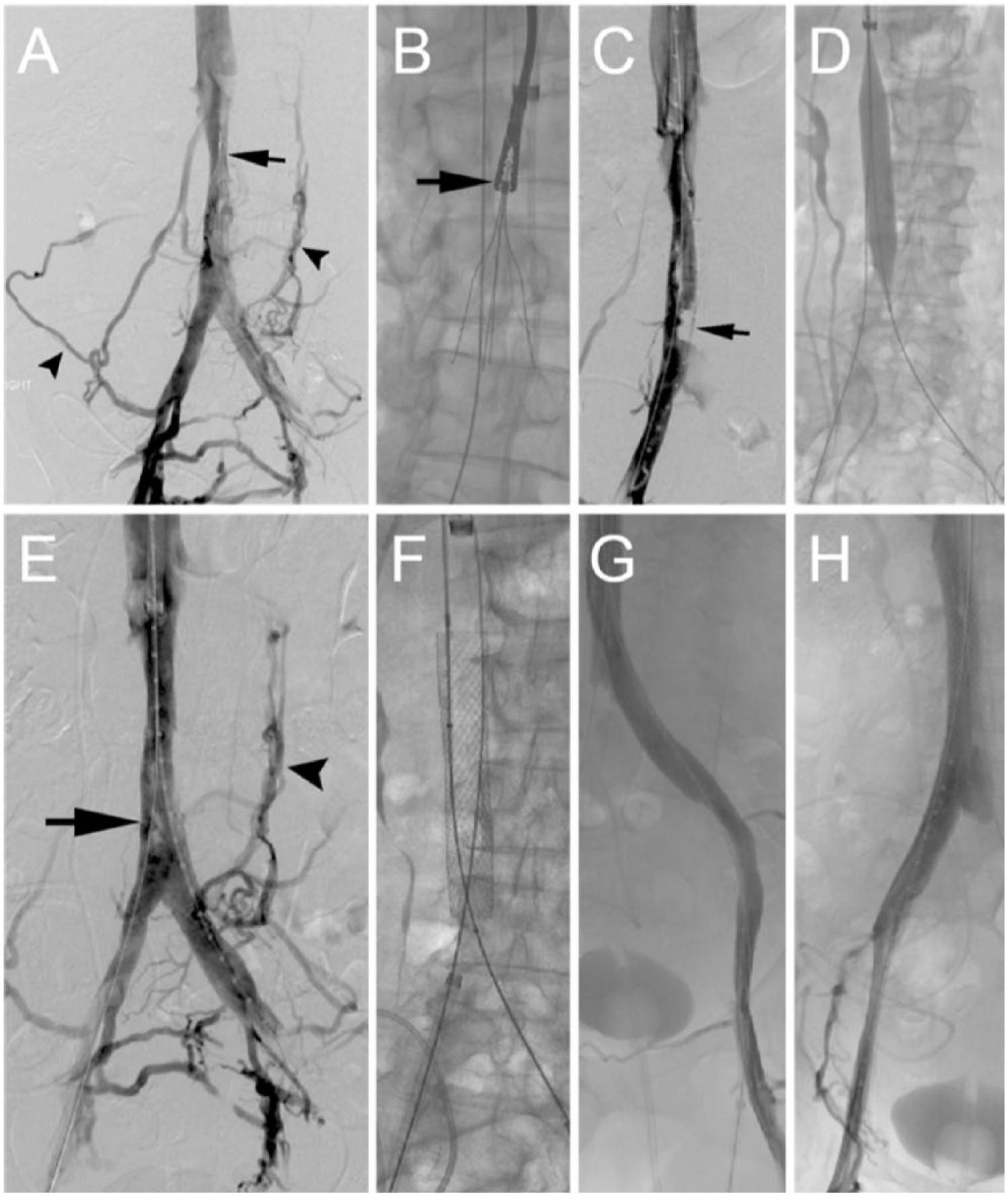
Chronic filter-bearing iliocaval thrombosis with subsequent iliocaval recanalization and reconstruction. (A) Digital subtraction venography demonstrating an inferior vena cava filter within the inferior vena cava (arrow) with associated chronic thrombus and narrowing with associated collateral vessel formation (arrowheads). (B) 3-mm endobronchial forceps (arrow) are used to grasp the apex of the inferior vena cava filter from an internal jugular vein approach through a 16-French introducer sheath. (C) Following filter extraction, there is significant narrowing of the inferior vena cava with chronic thrombus; through-and-through access across the obstruction was successfully achieved (arrow). (D) Balloon venoplasty of the occluded segment is performed. (E) Digital subtraction venography after venoplasty demonstrates persistent collateral vessel formation (arrowhead) with chronic thrombus within the caudal IVC (arrow). (F) Bilateral through-and-through wire access is noted; a Wallstent (Boston Scientific, Marlborough, MD, USA) is deployed in the caudal inferior vena cava for caval recanalization. Completion venography from the left (G) and right (H) common femoral vein demonstrating the widely patent iliocaval system bilaterally.
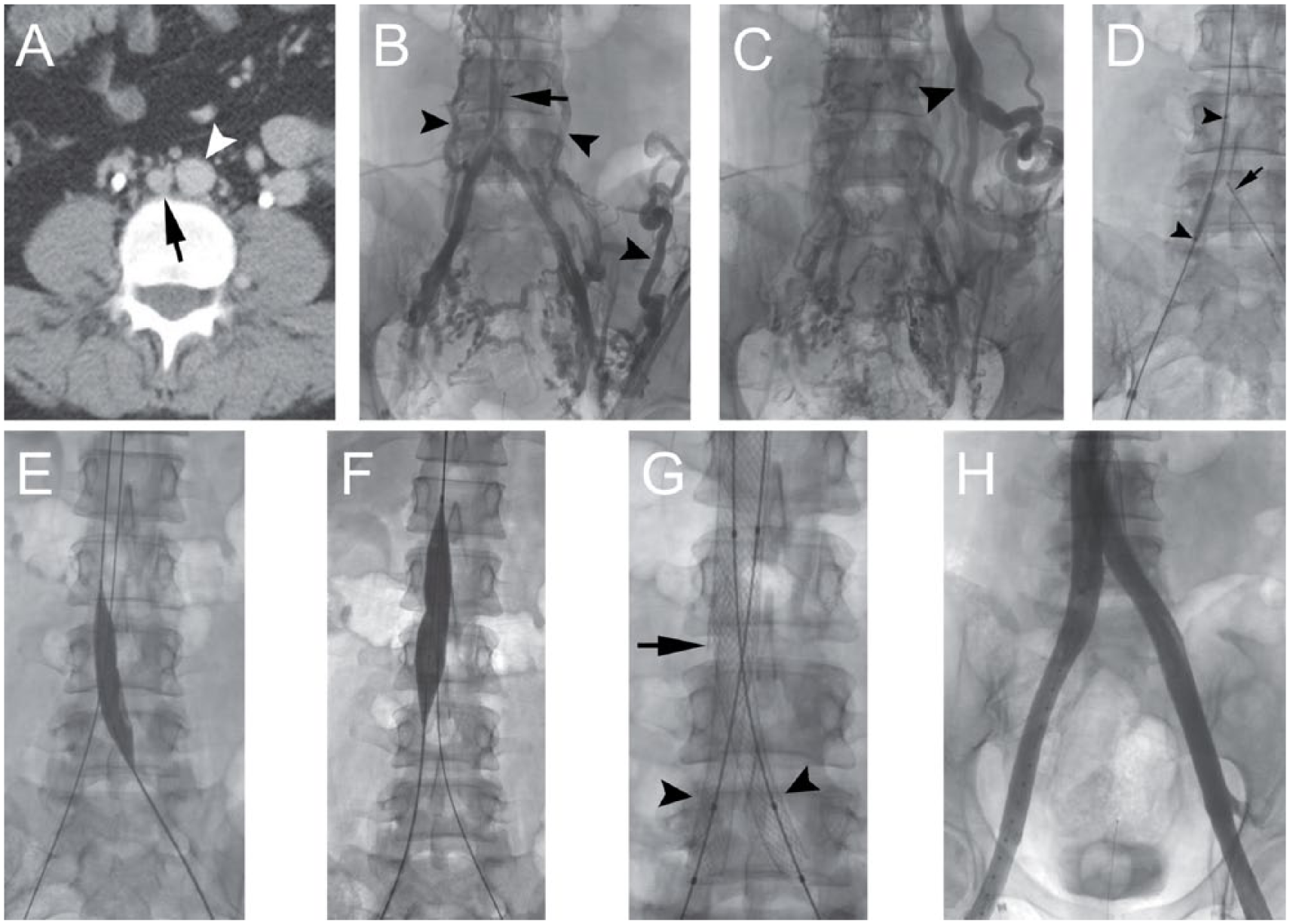
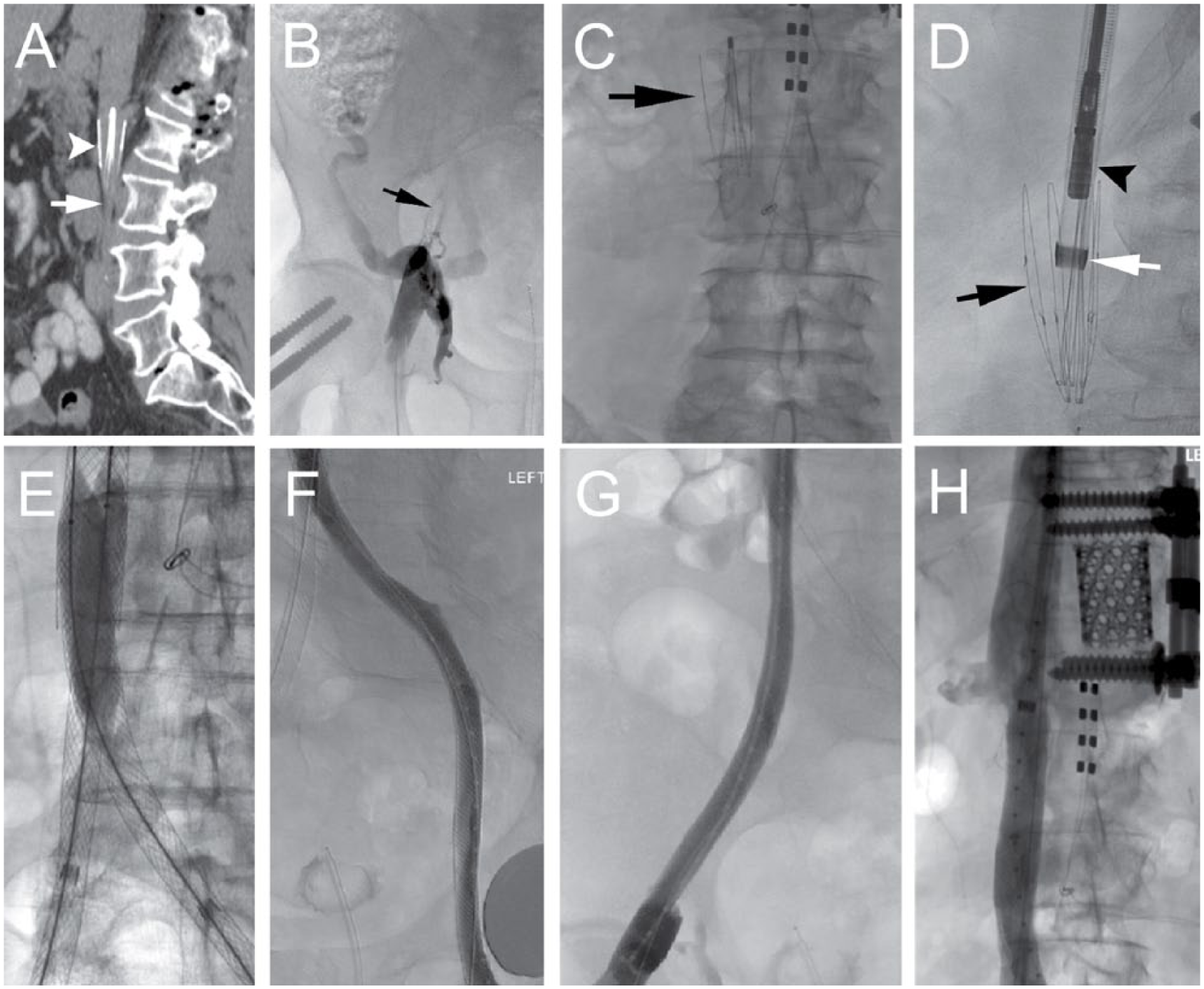
Inferior vena cava agenesis with subsequent iliocaval reconstruction with sharp recanalization. (A) A small diameter venous remnant is noted anterior to the spine (arrow) adjacent to the aorta (arrowhead). (B) Iliocaval venography demonstrating complete agenesis of the inferior vena cava (arrow) with robust collateral vessel formation (arrowheads). (C) A large retroperitoneal collateral vessel is seen in the left hemi-abdomen (arrowhead) with significant pelvic venous collaterals also seen. (D) Balloon angioplasty of the right iliocaval system (arrowheads) prior to stent placement; balloon targeting with a Rösch-Uchida needle (Cook Medical, Bloomington, IN, USA) for sharp recanalization (arrow) of the left iliocaval system. (E) Balloon angioplasty of the left iliocaval system followed by the inferior vena cava (F). (G) Stent reconstruction of the inferior vena cava (arrow) and the bilateral common iliac veins (arrowheads). (H) Completion venography demonstrating widely patent iliocaval stent reconstruction with free flow through the inferior vena cava (not pictured).
Chronic occlusion of the inferior vena cava from a permanent inferior vena cava filter (VenaTech LP; B. Braun, Melsungen, Germany). (A) Sagittal computed tomography image of the abdomen demonstrating a permanent inferior vena cava filter (arrowhead) within the infrarenal inferior vena cava (arrow). (B) Venography from the right femoral vein demonstrating complete occlusion of the iliac vein (arrow) with collateral vessel formation. (C) A permanent VenaTech LP filter (arrow) within the inferior vena cava. (D) A VenaTech LP filter (black arrow) is removed from an internal jugular vein approach using a 16-French introducer sheath (white arrow) and 3-mm endobronchial forceps (arrowhead). Following iliocaval recanalization and balloon angioplasty, stent reconstruction of the inferior vena cava was performed. (E) Kissing Wallstent (Boston Scientific, Marlborough, MD, USA) reconstruction of the common iliac veins and inferior vena cava with balloon angioplasty of indwelling stents. Final venography of the left (F) and right (G) iliac venous system and the inferior vena cava (H) demonstrating free flow through the iliac veins and inferior vena cava.
Following iliocaval reconstruction, inflow is evaluated with specific attention to the common femoral, femoral, profunda femoris and popliteal veins. If prompted by venography, these veins may require additional angioplasty and stenting to maintain adequate inflow into the reconstructed cava, as this is critical for maintaining long-term patency. Additionally, many of these patients have chronic thrombus extending down to the origin of the common femoral vein, and stenting in this area may be required. Attempts should be made to preserve the inflow of the profunda femoris vein as it may serve as primary or secondary drainage of the lower extremity following iliocaval reconstruction. To perform venography on the common femoral veins, a flush catheter should be advanced from the internal jugular access down to the mid-thigh and beyond any stents placed in the iliofemoral segment (Figure 1F). Contrast should be used to visualize the iliocaval recanalization in its entirety. If there is preferential flow through collaterals, there may be a proximal obstruction, and additional venoplasty and stenting of the common femoral and femoral vein segments may be necessary.
Technical considerations
Attempts at recanalizing an obstruction may lead to inadvertent passage of a guidewire or recanalization needle outside the vessel lumen. Short segments of extravascular passage have not been a problem. If a major venous tear is encountered, self-expanding stent-grafts may be placed across the lesion such as the Viabahn (Gore Medical, Flagstaff, AZ, USA) or TAG (Gore Medical). The authors choose to administer procedural anticoagulation only after recanalization and safety of the pathway has been validated, in order to facilitate thrombosis of false passages during attempted recanalization. Some operators may choose to perform recanalization while the patient remains therapeutically anticoagulated. After successful recanalization, the authors administer intravenous heparin titrated to an activated clotting time of 200–300 seconds until the end of the procedure.
Recanalization near the left proximal common iliac vein and the mid-IVC does present an increased risk of arterial injury to the right common iliac artery and renal arteries, respectively. In these regions, intravascular ultrasound may assist in localizing these arteries and aid in safe passage of the guidewire. Also, placing an arterial line and intermittently injecting contrast may further assist in avoiding arterial injury. If the ureter is in close proximity to the area of occlusion and sharp recanalization is required, a nephroureteral stent should be placed preprocedurally to ensure that the ureter is not traversed.
Patients with IVC filter-associated iliocaval thrombosis present an additional challenge for recanalization. Filter retrieval should be attempted; however, a stent may also be placed across the filter to exclude it from the reconstructed lumen.14,15 Self-expanding 18–24 mm stents may be used to exclude an IVC filter. 14 Moreover, there are data to suggest no significant difference in long-term patency rates between filter retrieval or exclusion techniques. 14 Thus, the safest, most feasible method should be pursued.
Complications
The most common complication following iliocaval reconstruction is a self-limiting access site hematoma or bleeding, which may usually be managed with manual compression or assisted pressure devices.2–5,7–9 In rare cases, an access site hematoma or retroperitoneal hematoma secondary to venous perforation or arterial injury may become hemodynamically significant. In such cases, hemoglobin concentration should be monitored serially while holding anticoagulation temporarily. Additionally, computed tomography arteriography should be considered. If bleeding persists, antiplatelet agents such as aspirin and clopidogrel should be held or reduced. Other complications include stent migration or misplacement. This may often be avoided with meticulous preprocedural planning and measurement. If stent migration does occur, an additional stent may be placed to ‘bridge the gap’ between the migrated and appropriately placed stents to prevent interstent thrombosis or restenosis.2–5,7–9,16
Postprocedural care
There are no specific recommendations regarding anticoagulation after iliocaval stent reconstruction, primarily due to a lack of prospective and randomized studies. In general, the approach includes multiple antithrombotic agents in the short term, followed by fewer agents in the chronic phase. Some operators (including the authors) advocate that patients should be anticoagulated with enoxaparin 1 mg/kg twice daily, clopidogrel 75 mg daily, and aspirin 81 mg daily prior to discharge. Enoxaparin is chosen to ensure reliable anticoagulation (unlike warfarin) with a rapid onset and the potential for anti-inflammatory properties. 17 Given the use of multiple antithrombotic agents, clopidogrel is preferable to other P2Y12 inhibitor antiplatelet medications, such as prasugrel or ticagrelor. Other providers use anticoagulants acutely only for patients within 6 months of a diagnosed venous thromboembolism or known thrombophilia. 18 In the absence of these findings, those authors use dual antiplatelet therapy.
Patients should then be seen in clinic within 2 weeks after the intervention, where they may be transitioned to warfarin or a direct oral anticoagulant. For long-term treatment, some advocate aspirin should be continued indefinitely and clopidogrel may be discontinued after 2–3 months. The authors routinely continue anticoagulation for at least 6 months before considering discontinuation; however, others (as noted above) limit the use of anticoagulation in lower-risk patients. 18 Patients with thrombophilia or recurrent venous thromboembolism should be anticoagulated indefinitely and managed by a hematologist or vascular medicine specialist. Routine screening for thrombophilias, however, is not recommended. 19
Clinical follow-up to assess symptoms and compliance with antithrombotic regimens are important. Venography or CTV may be performed at 6, 12, and 24 months to monitor patency, although there are limited data available on post-procedural follow-up.
Outcomes
Several studies by multiple groups have reported favorable technical success rates of iliocaval reconstruction with high patency. A study on 159 patients with chronic venous occlusion by Neglén and Raju revealed an 83% technical success rate in patients with iliac vein occlusions and a 98% success rate in patients with IVC filter-associated IVC thrombosis. 5 Four-year primary and secondary patency rates were 35% and 72%, respectively, for iliac vein recanalization and 40% and 80%, respectively, for IVC recanalization. 5 In a European study of 89 patients, primary, assisted-primary and secondary patency rates were 83%, 89% and 93%, respectively, at 3 and 10 years. 7 Additionally, Chick et al. conducted a study of 120 patients with IVC filter-associated iliocaval thrombosis and reported technical success in all patients, and 2-year primary-assisted and secondary patency rates of 90% and 94%, respectively. 14
Conclusion
Iliocaval stent reconstruction for life-limiting iliocaval thrombosis is often a technically successful procedure in experienced hands that results in favorable clinical outcomes, stent patency, and low complication rates. Further research is needed in devising optimal anticoagulation and antiplatelet regimens, as well as basic science study on the biological interaction between the stent and the venous system.
Footnotes
Declaration of conflicting interests
Geoff Barnes is supported by research grants from Pfizer/BMS and the NHLBI, and consulting for Pfizer/BMS, Janssen, and Portola. The other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed no financial support for the research, authorship, and/or publication of this article.