
Abstract
Mortality associated with high-risk pulmonary embolism (PE) remains high. Extra-corporeal membrane oxygenation (ECMO) allows for acute hemodynamic stabilization and potentially for administration of other disease process altering therapies. We sought to compare two eras: pre-ECMO and post-ECMO in relation to high-risk PE treatment and mortality. A single-center retrospective chart review was conducted of high-risk PE patients. High-risk PE was defined as acute PE and cardiac arrest or shock. A total of 60 patients were identified, 31 in the pre-ECMO era and 29 in the post-ECMO era. Mean age was 56.1±21.1 years and 51.7% were women. More patients in the post-ECMO era were identified with computed tomography (82.8% vs 51.6%, p=0.011) and more patients in the post-ECMO era had right ventricular dysfunction on echocardiography (96.4% vs 78.3%, p=0.045). No other differences were noted in baseline characteristics or clinical, laboratory and imaging data between the two groups. In total, ECMO was used in 13 (44.8%) patients in the post-ECMO era. There was greater utilization of catheter-directed therapies in the post-ECMO era compared to the pre-ECMO era (n = 7 (24.1%) vs n = 1 (3.2%), p=0.024). Thirty-day survival increased from 17.2% in patients who presented in the pre-ECMO era to 41.4% in the post-ECMO era (p=0.043). While more work is necessary to better identify those PE patients who stand to benefit from mechanical circulatory support, our findings have important implications for the management of such patients.
Introduction
The mortality associated with high-risk pulmonary embolism (PE) has been reported to be as high as 70%. 1 This high mortality is a result of acute hemodynamic decompensation, which is primarily caused by an acutely failing right ventricle. 2 Current treatment standards for high-risk PE may include thrombolytic therapy (either systemic or catheter based), various catheter based clot-retrieval techniques, emergent embolectomy and hemodynamic support. 3 As hemodynamic improvement is not often immediate after treatment for high-risk PE, extra-corporeal membrane oxygenation (ECMO) has been suggested for cardiopulmonary support either as a bridge to therapy or as support after therapy.4–12 Through bypass of the failing right ventricle and lungs, ECMO maintains cardiac output and mitigates end-organ damage while definitive PE treatment is undertaken. Utilization of ECMO may allow for aggressive treatment of high-risk PE – including administration of thrombolytic medications, catheter-directed interventions, and surgical embolectomy.
Emerging but limited data suggest that aggressive management of high-risk PE, including the institution of ECMO, may improve morbidity and mortality in massive PE.4–12 Thus, ECMO has been employed in our institution with the aim of improving hemodynamic parameters and clinical outcomes in patients with high-risk PE.
We therefore sought to compare treatment patterns and outcomes of patients with high-risk PE treated at our institution before and after the implementation of ECMO in this high-risk population.
Methods
The institutional review board of Partners Healthcare and Massachusetts General Hospital approved the protocol.
All patients over age 18 years who were admitted to Massachusetts General Hospital from 1 January 1994 through 31 December 2014, and who were assigned International Classification of Diseases-9 codes for PE (415.1 or 416.2) and cardiac arrest (427.5) or PE and shock (785.5), were eligible for inclusion. A medical records database query provided a list of subjects who satisfied these criteria. To ensure selection of a uniform patient population inclusive of only the sickest of PE patients, we defined patients with acute PE and cardiac arrest or shock as ‘high-risk’ and performed manual chart review to verify eligibility for inclusion. Cases of presumed PE and non-thromboembolic pulmonary arterial obstructive processes (e.g. amniotic fluid embolism) were excluded. Detailed review of each medical record was then performed to extract clinical details for analysis (DLA).
Emergent ECMO began to be utilized for acute high-risk PE at our institution around January 2011. We therefore identified two groups of patients with high-risk PE for comparison: those from the pre-ECMO era, from 1994 to 2010, when ECMO was not widely utilized for the management of patients with decompensated PE, and those from the post-ECMO, aggressive era, 2011 until 2014, with 24-hour ECMO availability.
Descriptive statistics were used to report the various variables. Between-group differences in patient characteristics were evaluated by using the chi-squared and Fisher’s exact tests for categorical variables, t-tests and Wilcoxon rank sum tests for continuous variables. A two-sided p-value less than 0.05 was considered statistically significant.
Results
Sixty subjects (31 women, 51.7%) with a mean age of 56.1± 21.1 years were included in the study. Table 1 shows patient demographics and comorbid conditions, and Table 2 shows the clinical, imaging, and laboratory data at the time of presentation. There was a trend towards increased prevalence of coronary artery disease in the pre-ECMO era (16.1% vs 0%, p=0.053). More patients in the post-ECMO era were diagnosed by computed tomography (CT) (82.8% vs 51.6%, p=0.011). Otherwise there were no differences in baseline characteristics between the pre- and post-ECMO groups.
Demographic and comorbid conditions in patients with massive PE.
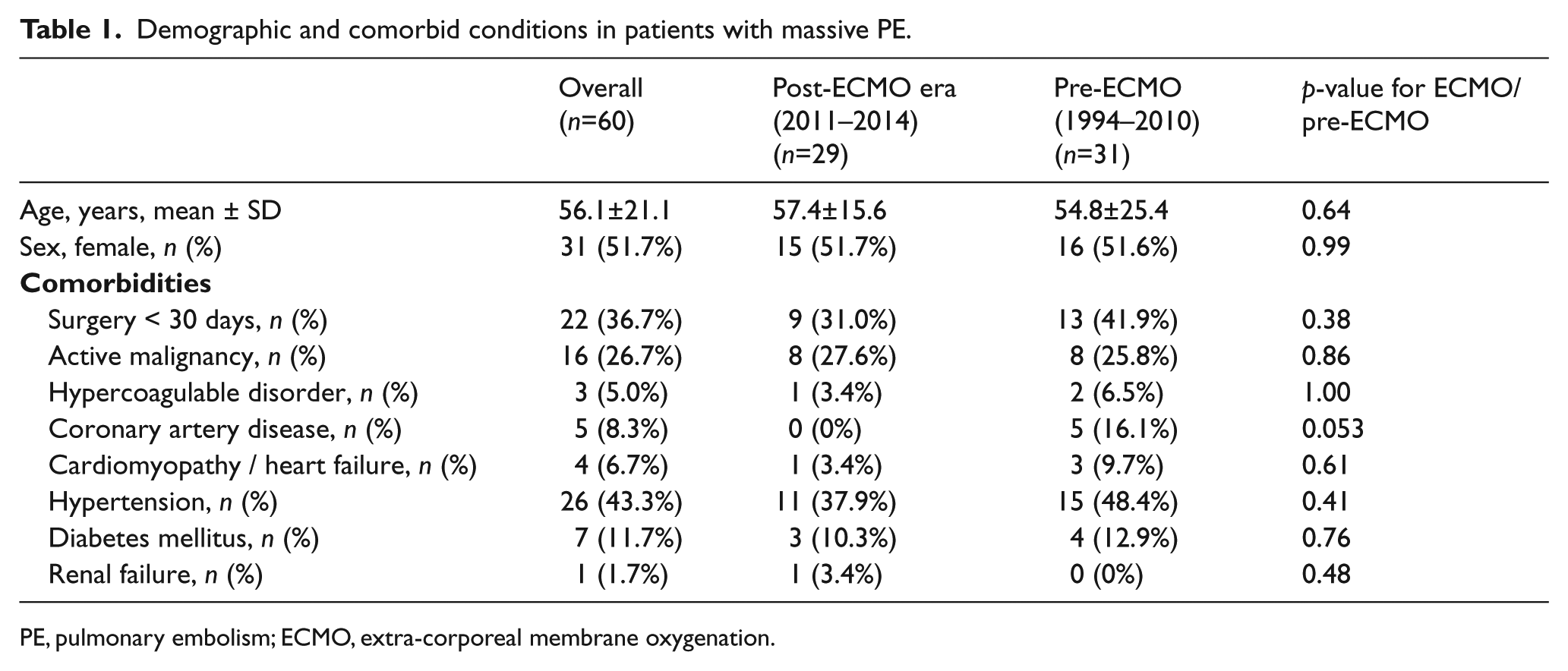
PE, pulmonary embolism; ECMO, extra-corporeal membrane oxygenation.
Clinical, imaging, and laboratory data at the time of presentation in patients with massive PE.
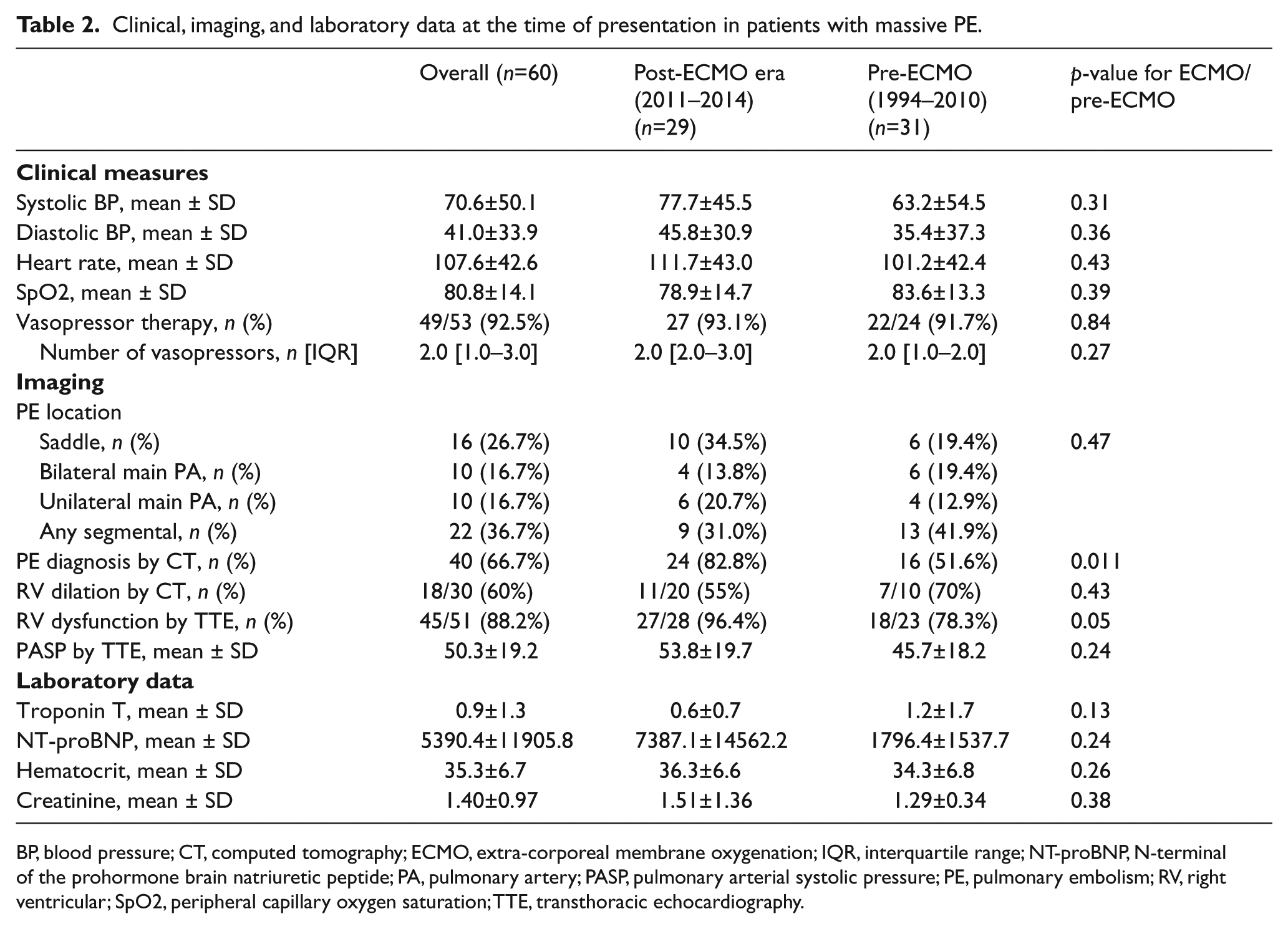
BP, blood pressure; CT, computed tomography; ECMO, extra-corporeal membrane oxygenation; IQR, interquartile range; NT-proBNP, N-terminal of the prohormone brain natriuretic peptide; PA, pulmonary artery; PASP, pulmonary arterial systolic pressure; PE, pulmonary embolism; RV, right ventricular; SpO2, peripheral capillary oxygen saturation; TTE, transthoracic echocardiography.
Overall, 31 subjects with high-risk PE were treated between 1994 and 2010 during the pre-ECMO era, and 29 were treated in the post-ECMO era. The average systolic blood pressure was 70.6 mmHg, the average heart rate was 107.6 beats/min, and the average oxygen saturation was 80.8%. As expected for this patient population, right ventricular (RV) dysfunction was present in 88.2% of patients who were assessed with echocardiography, and blood pressure was supported with vasopressors in 92.5% of patients. More patients in the post-ECMO era had echocardiographic evidence of RV dysfunction (96.4% vs 78.3%, p=0.045). In total, ECMO was employed in 13 (44.8%) patients in the post-ECMO era versus none in the pre-ECMO era. Otherwise, no differences were detected between patients in the two eras.
All patients who received ECMO were cannulated within the first day of presentation; the average time from presentation to cannulation was 6 hours (range 2.4 to 22.3 hours). Seven patients were cannulated in the operating room, one in the cardiac catheterization laboratory, and five in other locations, such as the emergency department or intensive care unit. Nine patients received peripheral veno-arterial ECMO, while four received central veno-arterial support. The average length of ECMO support was 4 days. In nine patients, ECMO was instituted before the definitive therapy. In the remaining four cases, ECMO was started after surgical embolectomy; in each of these cases, ECMO was started in the operating room, immediately following embolectomy.
Table 3 shows the treatment modalities utilized in these patients. All patients who received ECMO also received invasive PE-related treatment, either catheter-directed therapies or surgical embolectomy, and there was overall greater utilization of catheter-directed therapies in the post-ECMO era compared to the pre-ECMO era (n = 7 (24.1%) vs n = 1 (3.2%), p=0.024).
Treatment modalities employed in patients with massive PE.
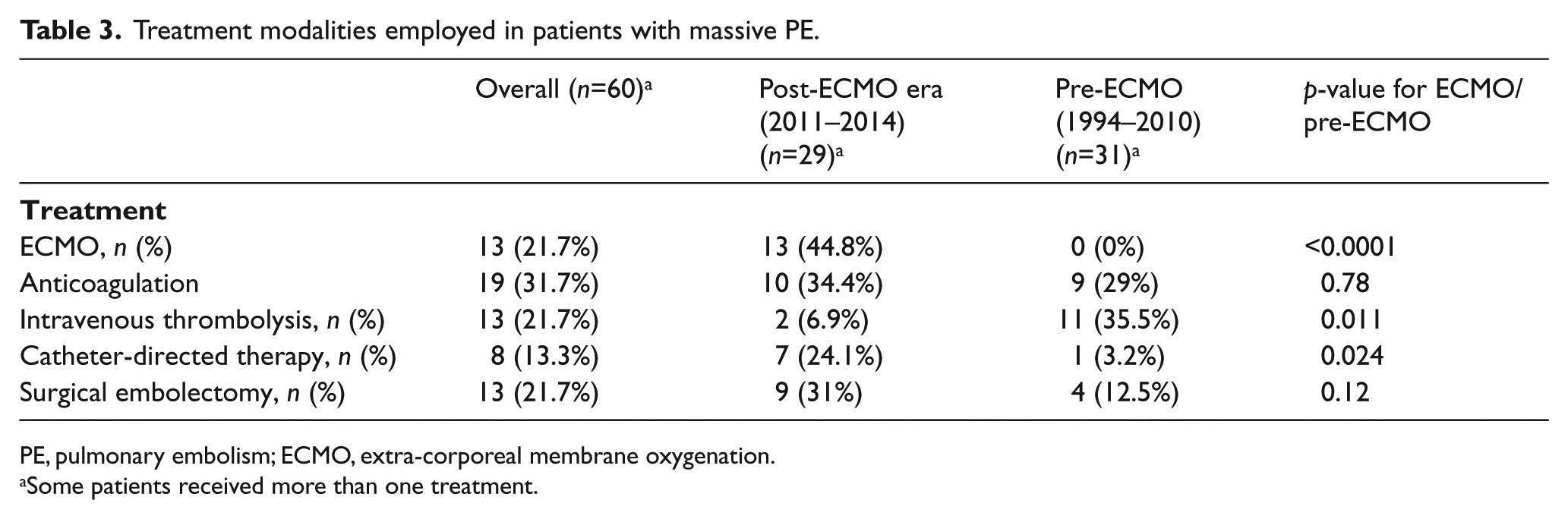
PE, pulmonary embolism; ECMO, extra-corporeal membrane oxygenation.
Some patients received more than one treatment.
Thirty-day survival increased from 17.2% in patients who presented in the pre-ECMO era to 41.4% in the post-ECMO era (p=0.043). Numerically, there was also improved 1-year survival in the post-ECMO era, although this did not achieve statistical significance (30.8% vs 17.2%).
Discussion
These findings suggest that the implementation of a program to aggressively manage patients with PE and shock or cardiac arrest, which includes the 24-hour availability of ECMO, may improve survival. While causality cannot be inferred between the introduction of ECMO and patient outcomes, examination of our results suggests a plausible explanation for the improved survival with the implementation of ECMO for massive PE complicated by shock or cardiac arrest.
By stabilizing hemodynamic parameters and improving oxygenation, ECMO can serve as a bridge to other therapies as well as to recovery. An overall more aggressive approach to high-risk PE was likely permitted by ECMO support. This includes surgical embolectomy and catheter-directed thrombolysis, both of which were utilized more frequently in the post-ECMO era, as well as overall intensive medical care. Thus, perhaps the intervention we examined in the present study is best thought of as ‘ECMO and all subsequent treatment permitted by ECMO’.
As there are many unknowns in the care of PE patients, a team-based approach to these patients has been gaining popularity. Dubbed ‘PERT’ (PE Response Teams), complex patient care is addressed by several relevant specialists including, but not limited to, interventional cardiology, vascular medicine, hematology, radiology, pulmonary and critical care, and cardiothoracic surgery. 13 While these events do not correlate temporally with the advent of ECMO in our institution, they have been utilized to streamline the utilization of resources for the benefit of the most difficult to treat PE patients. 3
Notwithstanding, coincidental with the availability of ECMO, a more aggressive approach to the treatment of PE was undertaken, suggesting that some of these therapies may have been facilitated by ECMO support. Work published over the latter half of the last decade has demonstrated that ECMO has a role as a bridge to percutaneous coronary intervention in patients with acute coronary syndrome and cardiogenic shock, as well as in the treatment of cardiogenic shock itself.14–16 Similarly, in patients with high-risk PE, ECMO can function as an adjunct to anticoagulation or systemic thrombolysis; as a bridge to invasive management, such as surgical embolectomy or catheter-directed therapies; or, as post-procedural support for patients undergoing these therapies.
Supporting our findings, several case reports and small case series have suggested that ECMO may have a role in decreasing mortality in patients with massive PE.4–12 One case series spanning 13 years included 21 patients with massive PE, 13 of whom developed cardiogenic shock and eight that had ongoing cardiac arrest. Thirteen of the 21 patients (62%) survived to 1 year. 10 Another recent series included four patients with massive or submassive PE who had been aggressively managed before the institution of ECMO. Three of these patients died during the index hospitalization. The authors of this case series caution that a reporting bias likely exists in the literature, and suggest that the mortality of patients with PE who are placed on ECMO may be higher in practice than is suggested by case reports. 6
Limitations
Our study is retrospective and limited by a small sample size. However, to date, there have been no published data comparing ECMO as part of the armamentarium for treatment of PE with standard care without ECMO support. Furthermore, in relation to previous publications, our series is comparatively large. While our analysis suggests that ECMO use may be associated with improved mortality in high-risk PE patients, we acknowledge the presence of confounders influencing this association, particularly the more generalized use of more aggressive therapies in our ECMO era. Thus, ECMO was only viewed as part of a more generalized approach to these patients.
Conclusion
In conclusion, our hypothesis-generating study demonstrates an increase in 30-day survival among patients with cardiac arrest or shock resulting from PE who were treated once an aggressive PE treatment program, including ECMO and other invasive therapies, was instituted. While more work is necessary to better identify those patients who stand to benefit from mechanical circulatory support, our findings have important implications for the management of such patients.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jay Giri is a member of the Board of Directors of PERT Consortium, a 501c3 not for profit organization. Michael Jaff is an equity shareholder in Embolitech and a paid consultant to PHILIPS/Volcano. Kenneth Rosenfield serves on advisory boards for Abbott Vascular, Cardinal Health, Surmodics, Inari Medical, Volcano/Philips, and Proteon; receives fees and stock options for serving on advisory boards for Cruzar Systems, Valcare, and Eximo; receives stock options for serving on advisory boards for Capture Vascular, Shockwave, Micell, Endospan, and Silk Road Vascular; receives stock options for serving on the advisory boards of and holding equity positions in Contego, Access Vascular, and MD Insider; holds stock/stock options in Embolitech, Janacare, Primacea, and PQ Bypass; will receive a future payout from a previous equity position in Vortex; and receives grant support paid to his institution from Abbott Vascular, Atrium/Maquet, and Lutonix/Bard. The other authors have no disclosures.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.