
Abstract

Angiographic assessment of type B chronic aortic dissection can be complicated in thoracic endovascular aortic repair (TEVAR) procedures due to a complex flow pattern. The challenge in identifying the true and false lumen and the precise deployment of the endograft in the true lumen are hotspots in endovascular treatment dissections. 1 Parametric color coding (PCC) is a recent tool for measuring flow dynamics in a digital subtraction angiography (DSA) series that provides quantitative information. In a single image, the quantitative DSA (Q-DSA; Syngo iFlow software; Siemens, Forchheim, Germany) displays objective information on the contrast medium through vessels.2,3
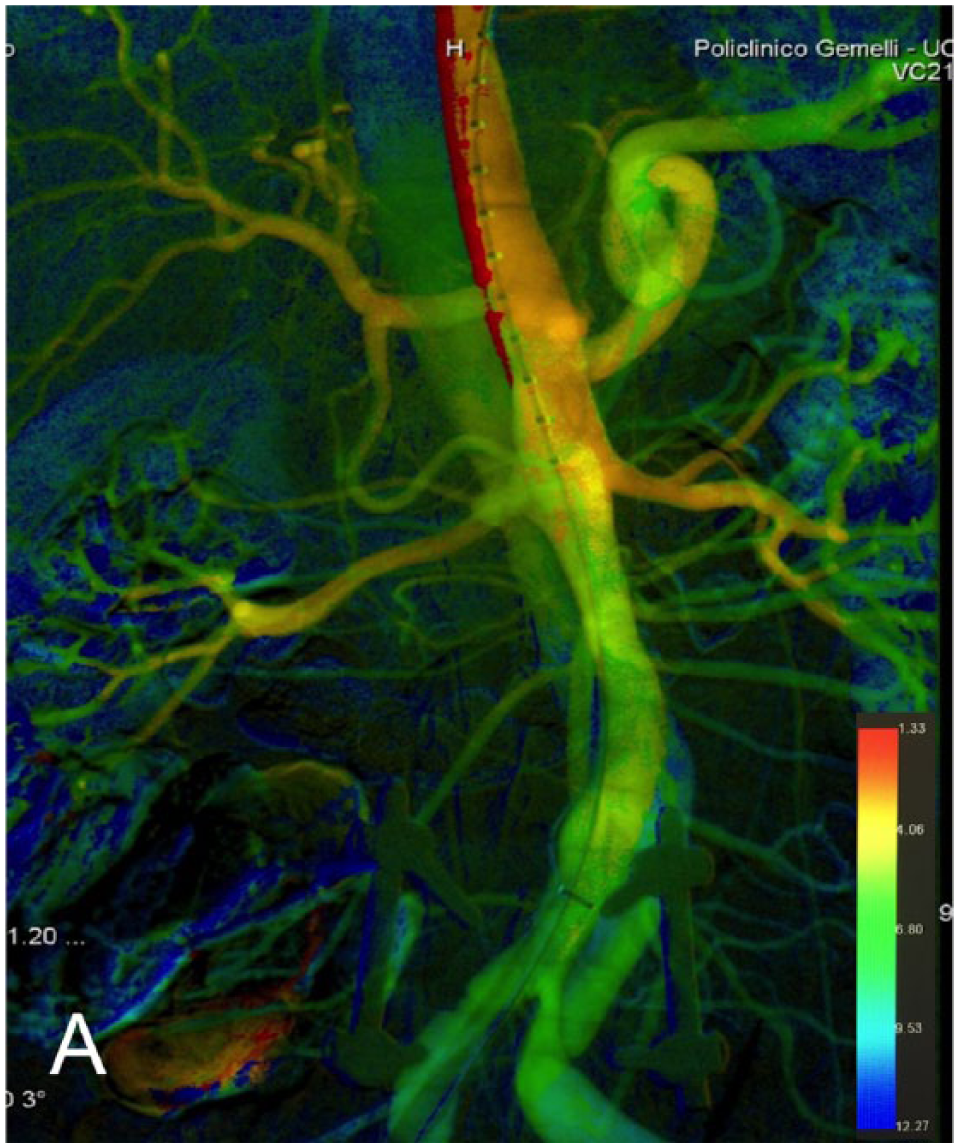
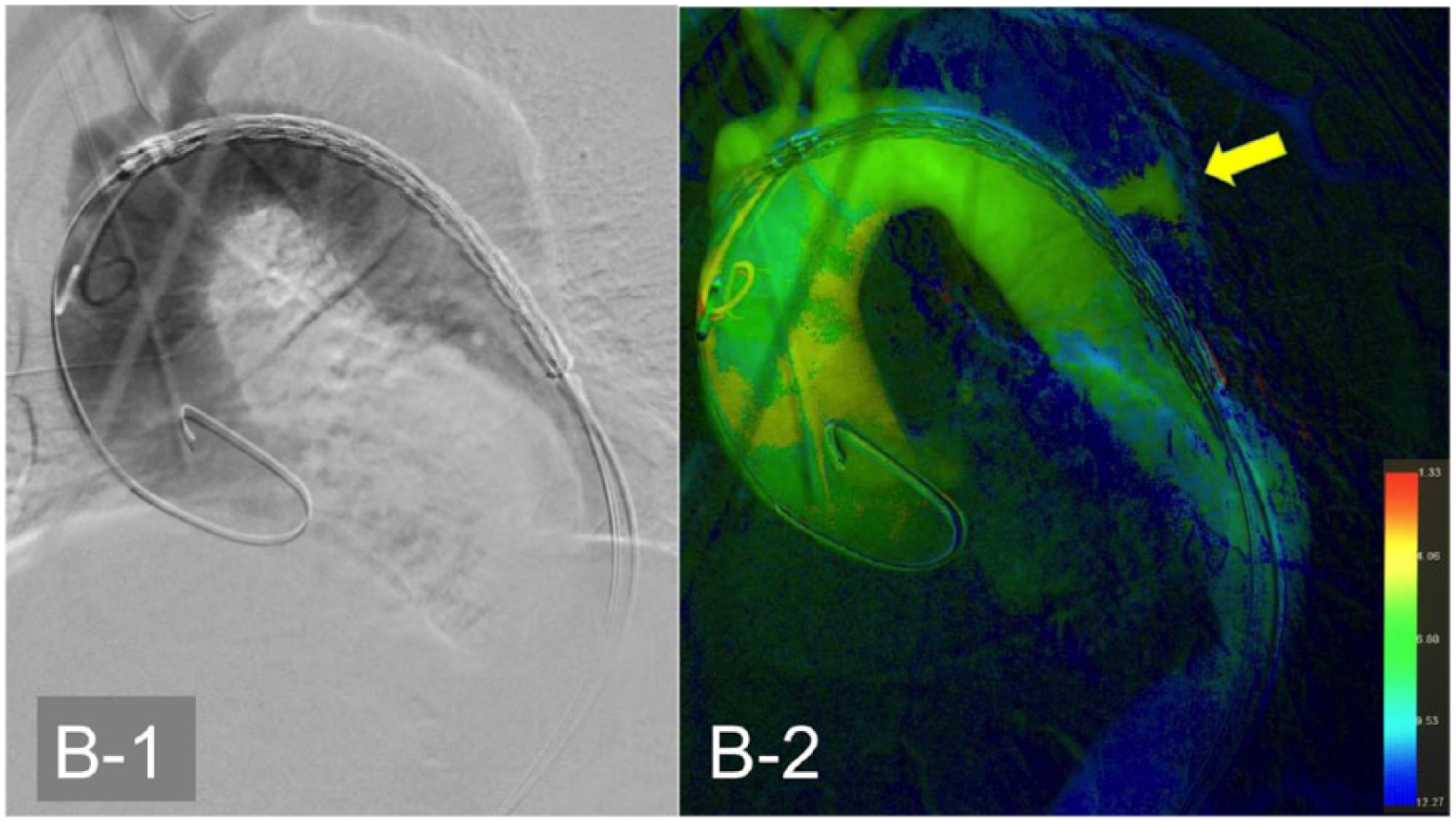
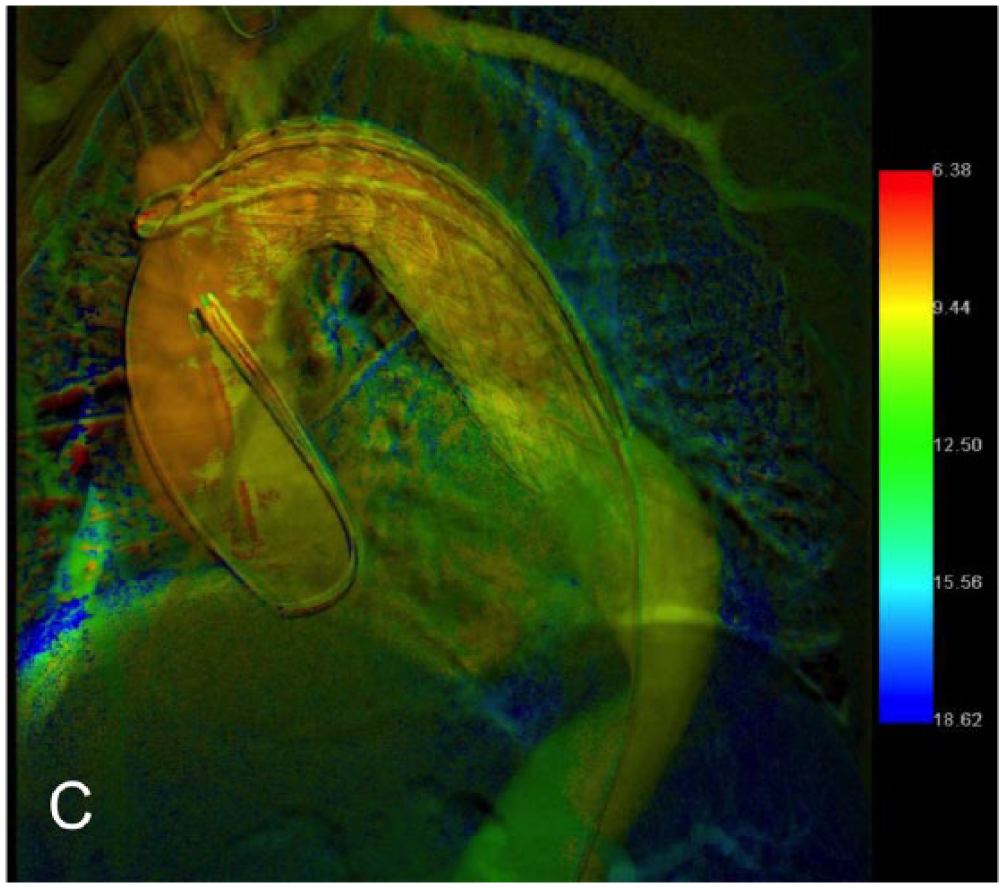
We describe the potential utility of Q-DSA in the endovascular treatment of a 76-year-old man who presented with a thoracic false lumen aneurysm measuring 6.2 cm accompanied by a large proximal entry tear. After a carotid-subclavian bypass to obtain a zone 2 sealing zone, TEVAR for a proximal entry tear coverture was performed. Three intraoperative DSAs (4 frames/s, 20 mL of 350 iomeprol contrast with a flow rate of 10 mL/s) were performed. This series was immediately post-processed (approximately 3 seconds) using Syngo iFlow. The PCC image of visceral aorta DSA indicated the catheter position in the true lumen without further confirmation from an angiogram. The physiologic differences in blood flow into the true and false lumen produce a different PCC that results in the simultaneous identification of the true and false lumen in a single static image (Panel A). The Q-DSA aortic arch view before device deployment displayed more information on the proximal entry tear position and false lumen than the DSA (Panels B1 and B2, arrow indicates the proximal entry tear). Finally, the last quantitative angiogram confirmed a good device deployment and covering of the entry tear. The last angiogram also provided information regarding early false lumen reperfusion (Panel C). In addition, the different aortic color coding before and after device deployment indicated a different contrast medium diffusion due to a new aortic hemodynamic consequence of the entry tear coverture and false lumen depressurization (Panels B2 and C).
These images can facilitate the diagnosis of vascular diseases and procedure assessment, especially for less experienced physicians. 2 Without the additional cost of X-ray and contrast exposure, Q-DSA serves as a real-time application tool that may provide additional support in the angiographic evaluation of type B chronic aortic dissection during TEVAR. Visualizing the complex aortic dissection architecture can be simplified, thereby increasing diagnostic confidence and accuracy.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.