
Abstract

A 66-year-old man with a 30-year history of bilateral intermittent claudication was referred to our hospital. His medical history included hypertension, dyslipidemia, stroke, and impaired glucose tolerance, treated with standard medications. He had a 46 pack-year smoking history, but never used illicit drugs. He had no family history of vascular diseases. Both lower legs were cold and the ankle–brachial index was markedly decreased (0.49 on the right and 0.59 on the left). Laboratory examination was unremarkable, including serum calcium, phosphate, and parathyroid hormone.
Computed tomography showed severely calcified lower extremity arteries, in contrast to little calcification in the aorta (Panel A, left). Conventional X-ray displayed slight pericapsular calcification of the finger joints (Panel B, upper panels: white arrows; R, right; L, left), and bilateral calcified aneurysmal popliteal and brachial arteries (Panel A, right and Panel B, lower panels).


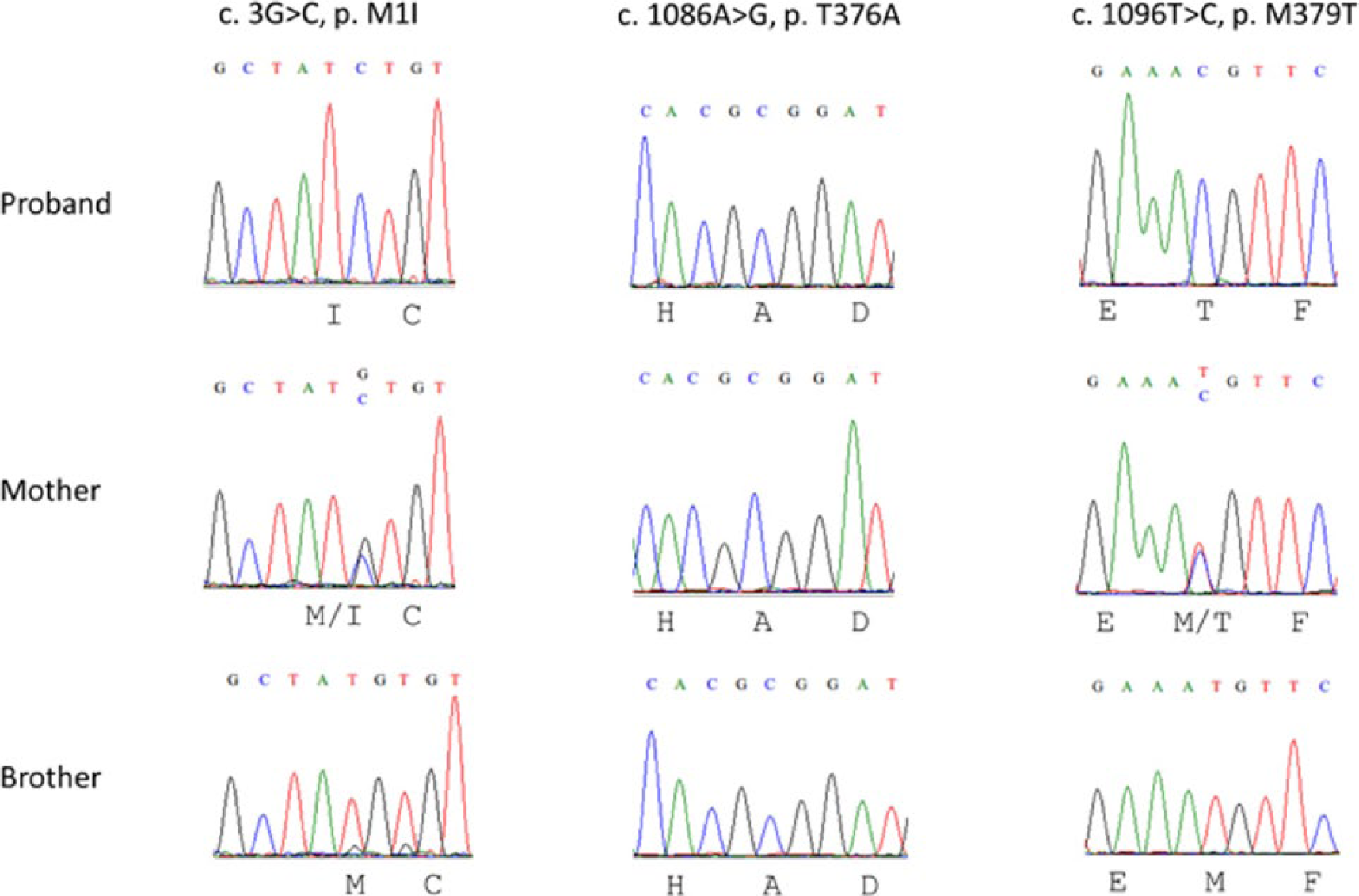
Considering these findings, genetic screening of the ecto-5’-nucleotidase (NT5E) gene was conducted with the patient’s informed consent. Genomic DNA was extracted and amplified by polymerase chain reaction (PCR) for each exon of the NT5E gene (NM_002526.3) and analyzed by direct sequencing. Four novel homozygous mutations were identified (3G>C, 488C>T (silent mutation; not shown), 1086A>G, and 1096T>C) in the proband (Panel C), and he was diagnosed with calcification of joints and arteries (CALJA). Familial screening identified that his mother had one homozygous (1086A>G) and three heterozygous (3G>C, 488C>T, and 1096T>C) mutations, while his brother had one homozygous mutation (1086A>G). The families had no symptoms or findings of CALJA.
CALJA was originally described by Magnus-Levy in 1914, 1 and St Hilaire et al. 2 identified the causal mutations in the NT5E gene in 2011. Since then, 13 cases of CALJA from six families with NT5E mutations have been reported. The NT5E gene encodes CD73, which is thought to be a key inhibitor of tissue calcification. The classical characteristics of CALJA are late-onset profound calcification of lower extremity arteries and hand and foot joint capsules that spares the arteries in the trunk. Zhang et al. 3 reported a case of CALJA involving the upper extremity arteries, and our report is the second case to document a similar distribution.
In this case, we identified novel mutations in the NT5E gene. As 488C>T was a silent mutation (Y176Y), and his family members with 1086A>G seemed unaffected, 3G>C and/or 1096T>C are candidates for the causal mutation in this case. We speculated 3G>C was the causal mutation because it resulted in substitution of the start codon of the NT5E gene.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.