
Abstract
We looked retrospectively at the 3- to 5-year progression of mild, asymptomatic carotid artery stenosis (CAS). A random sample of 600 patients who had undergone at least two carotid artery duplex ultrasounds between 31 October 2006 and 1 November 2016 with a second duplex ⩾3 and ⩽5 years following the initial one were screened for inclusion. Internal carotid arteries (ICAs) were included if they had 20–49% stenosis on the initial duplex, with 440 carotid arteries meeting this criteria. Analyses were performed utilizing chi-squared and two-tailed t-tests. Twenty-four (5.45%) of the initial 440 carotid arteries progressed to moderate CAS. There was a statistically significant increase in the prevalence of hypertension (68% vs 47%, p=0.022) and diabetes mellitus (44% vs 22%, p=0.008) in patients with carotids that progressed to moderate CAS. There was a decrease in moderate-intensity statin use (32% vs 58%, p=0.005) and an increase in patients not on statins (36% vs 11%, p=0.001) in the group of carotids that progressed to moderate CAS. One carotid artery (0.2%) progressed from mild CAS to severe CAS. If supported by others, our data may lead to a change in the recommendations regarding appropriate follow-up of asymptomatic CAS.
Keywords
Introduction
Stroke continues to be the fifth leading cause of mortality and a major source of chronic disability in the United States. 1 The financial cost of stroke in the United States is estimated to be $36.5 billion annually. 2 Roughly two-thirds of all strokes are ischemic in nature and 20–30% of these are attributable to carotid atherosclerotic disease. 3 Stenosis of the extracranial carotid artery is estimated to be responsible for 9% of ischemic strokes. 1 The risk of cerebrovascular accident (CVA) associated with ipsilateral internal carotid artery stenosis (CAS) has declined significantly over the last 20 years as medical therapies for atherosclerotic disease have become more intensive. Recent data have shown that the risk of stroke in patients with asymptomatic carotid stenosis on intensive medical therapy is less than 1% per year.4–6
Patients with asymptomatic, mild CAS are generally followed with periodic carotid duplex ultrasounds (CUS), with the intent of identifying those who progress to severe disease. Such patients might be offered carotid endarterectomy or carotid artery stenting in addition to optimal medical therapy. If a follow-up CUS does not show progression to severe disease, however, then the results do not change management. 7 Optimal medical therapy includes high-intensity statins, anti-platelet therapy, hypertension control, and modification of other risk factors such as smoking. Data from patients treated with statins in the Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) trial showed a 33% reduction in stroke as well as a 43% reduction in coronary events.5,8
There is debate regarding the ideal frequency of follow-up carotid duplex studies in patients with mild, asymptomatic CAS. Performing them too often increases cost unnecessarily, whereas performing them too infrequently risks missing the ideal window for revascularization in those patients who do progress to severe disease. The 2012 American College of Cardiology Foundation (ACCF) Appropriate Use Criteria (AUC) for Peripheral Vascular Ultrasound and Physiologic Testing note that follow-up duplex testing for <50% CAS within 1 year is inappropriate and that frequency of follow-up after 1 year is uncertain. 9 Furthermore, the 2011 ACCF Guideline on the Management of Patients with Extracranial Carotid and Vertebral Artery Disease give a class IIa indication to repeat carotid duplex annually in patients with stenosis >50% but do not make recommendations for <50% stenosis. 7 In our large community-based practice consisting of both cardiologists and vascular surgeons, we are often faced with the challenging question of whether our patients with mild, asymptomatic CAS should have an annual carotid duplex study or if a longer interval such as every 3 years would be more appropriate.
To answer this question we looked retrospectively at the 3- to 5-year rate of progression of mild, asymptomatic CAS to moderate or severe CAS in patients from a large practice with the intent of better informing practitioners and patients regarding the optimal timing of repeat carotid duplex testing. A similar study by Olin et al., in 1998, looked at moderate, asymptomatic CAS and found a frequency of progression of 20% at 3 years. 10 We suspected, however, that our cohort of asymptomatic, mild CAS would progress at a lower frequency because of more aggressive lipid therapy guidelines during the time of our study and because a lower baseline severity of stenosis should predict slower progression of disease.11–13 We hypothesized that patients with asymptomatic, mild CAS could safely have CUS performed at a 3-year interval without missing a significant number of patients progressing to severe CAS in that time. In the absence of progression to severe stenosis, the management of the patient does not change.
Methods
Utilizing data from patients of Iowa Heart Center, a large practice consisting of cardiologists, vascular surgeons, and cardiothoracic surgeons, we designed a retrospective data collection study to evaluate the progression of mild CAS, as determined by CUS. We compiled a database from these records that initially included all patients who had undergone at least two CUS (n = 19,971). Utilizing a random number generator in SPSS (version 24, IBM, Armonk, NY, USA), a randomly selected sample of 600 patients’ records were reviewed for inclusion in the study. Additional data collected included demographics, medical comorbidities, and medical treatments. Since each internal carotid artery (ICA) with asymptomatic stenosis has been shown to be a risk factor for a future transient ischemic attack (TIA) or CVA, all carotids were reviewed individually. 4 The CUS were all performed at the Intersocietal Accreditation Commission Vascular Testing-accredited Iowa Heart Center Vascular Laboratory, and all studies were read by either a vascular surgeon or a cardiologist. Equipment utilized by the Iowa Heart Center Vascular Laboratory to perform carotid ultrasounds over the course of the study included the Acuson Sequoia (Mountain View, CA, USA), Toshiba Aplio 80 (Tustin, CA, USA), Toshiba XG, Toshiba Xario, Toshiba A500, Toshiba MX, Philips CX50 (Andover, MA, USA), GE Vivid Q (Chicago, IL, USA), and Esaote MyLab Alpha.
ICAs were eligible for inclusion if they showed 20–49% stenosis on the initial CUS, defined in the Iowa Heart Center Vascular Laboratory as plaque >2 mm thick and peak systolic velocity (PSV) <125 cm/sec with minimal spectral turbulence. ICAs with 1–19% stenosis, defined as minimal plaque or mild intimal medial thickening, were not included. ICAs reported as ‘<50%’ without specifying presence or absence of plaque, were reviewed by an RPVI reader and the ICA was included only if there was visible plaque of >2 mm in thickness. Additionally, patients must have undergone two CUS between 31 October 2006 and 1 November 2016, with the second CUS 3 to 5 years following the initial one. The first CUS done during the study period showing mild CAS in either ICA was considered the index study. ICAs were excluded if they had undergone carotid endarterectomy or stenting prior to the study period. Moderate ICA stenosis was defined as PSV >125 cm/sec with spectral turbulence and plaque, an ICA/common carotid artery (CCA) ratio of 2.0–3.99, and an end diastolic velocity (EDV) of 40–99 cm/sec. Severe ICA stenosis was defined as PSV >230 cm/sec and either an EDV >100 cm/sec or ICA/CCA >4.0 with spectral turbulence.
Patient demographics, medications, medical comorbidities, indication for initial CUS, and CUS results were obtained from the database and Iowa Heart Center electronic medical record (EMR) (NextGen Healthcare, Horsham, PA, USA). Patient demographics were included separately for each carotid artery that met the inclusion criteria. Patient age was defined as age at the time of the initial CUS included in the study. Tobacco use was self-reported by patients and included current tobacco smokers, former tobacco smokers, and never tobacco smokers. Former tobacco use was defined as any amount of prior tobacco smoking. Statin use during the study interval was obtained via EMR review and statin intensity was classified according to American College of Cardiology (ACC)/American Heart Association (AHA) guideline. 14 Antiplatelet use included use of any antiplatelet medication during the study interval. Presence of diabetes mellitus was determined by EMR review and the presence of diabetes mellitus was defined as a documented history of either type 1 or type 2 diabetes mellitus during the study interval. Additional comorbidities, including coronary artery disease (CAD), peripheral vascular disease (PVD), hyperlipidemia (HLD), and hypertension (HTN) were included as documented in the EMR during the study interval.
Statistical analyses were performed utilizing SPSS statistical software (version 24, IBM, Armonk, NY, USA). Demographic and clinical data are presented as the percentage prevalence in the respective study population. Chi-squared analysis was utilized for categorical data. Post hoc analysis was performed utilizing multiple regression to analyze contingency tables, where appropriate. 15 Continuous data are presented as means with standard deviations. Univariate analysis was performed using two-tailed t-tests for continuous variables. A p-value of <0.05 was considered statistically significant. The single carotid artery that progressed to severe stenosis was not included in statistical analysis due to low statistical power (n = 1).
The Institutional Review Boards at Mercy Medical Center in Des Moines, Iowa and Iowa Heart Center both approved this study.
Results
There were 440 ICAs that met the inclusion criteria out of the 600 patients reviewed. All included ICAs had mild CAS with visible plaque on the initial carotid artery duplex. Figure 1 summarizes the study design and findings. Table 1 contains the demographics, risk factors, antiplatelet medication use, and statin intensity for the carotid arteries included in the study. Figure 2 shows CUS images of ICAs in two different patients as examples of mild CAS with no clinically significant progression over the pre-specified follow-up period.
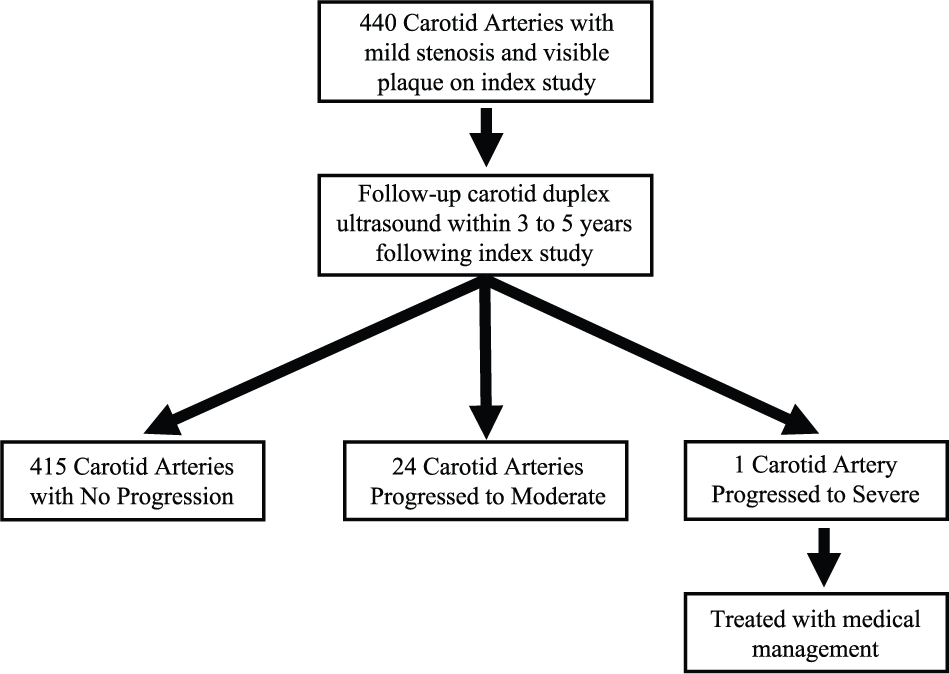
Progression of asymptomatic mild carotid artery stenosis: summary of study outcomes.
Baseline demographics and risk factors of the 440 internal carotid arteries with mild CAS.
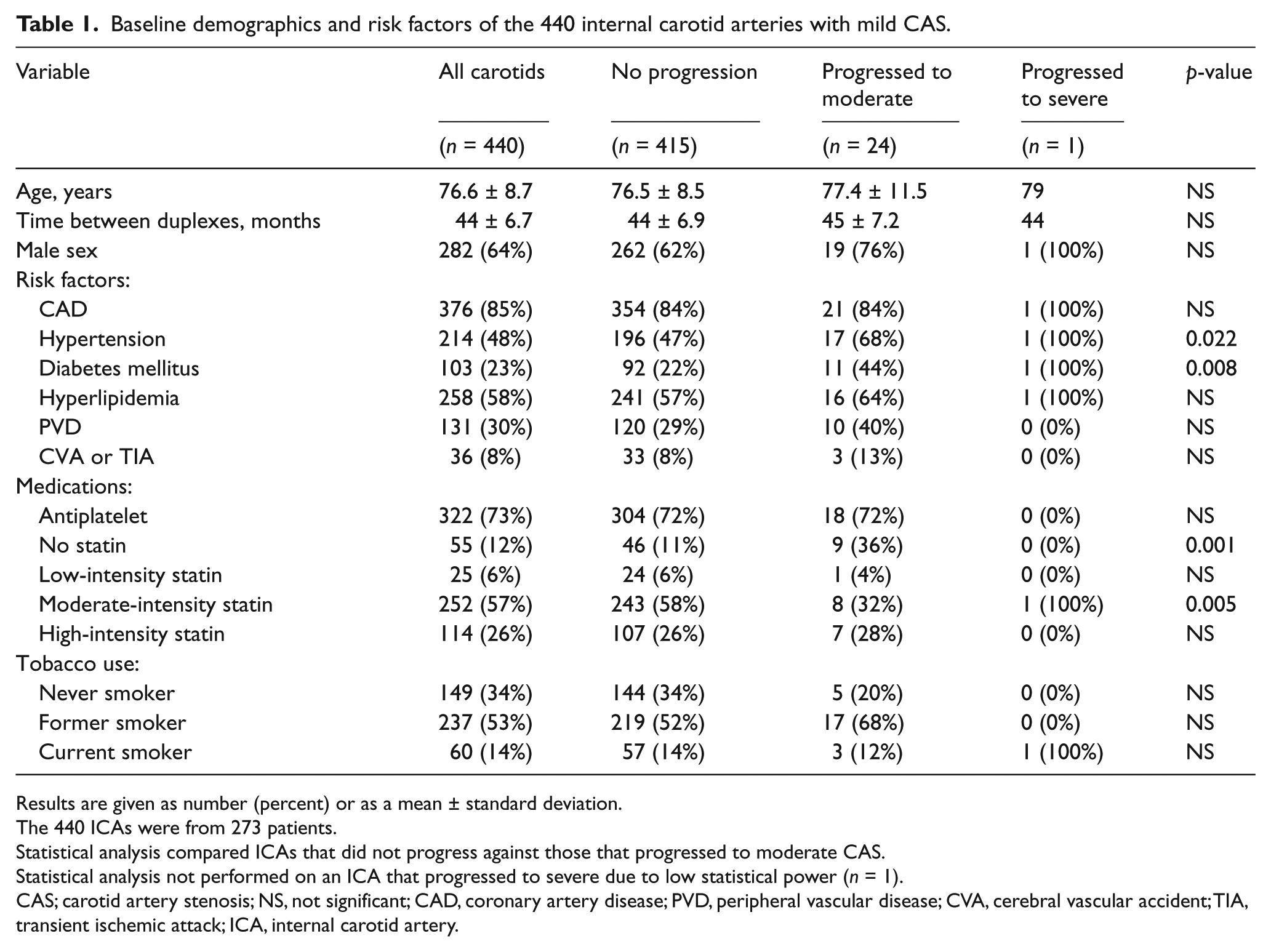
Results are given as number (percent) or as a mean ± standard deviation.
The 440 ICAs were from 273 patients.
Statistical analysis compared ICAs that did not progress against those that progressed to moderate CAS.
Statistical analysis not performed on an ICA that progressed to severe due to low statistical power (n = 1).
CAS; carotid artery stenosis; NS, not significant; CAD, coronary artery disease; PVD, peripheral vascular disease; CVA, cerebral vascular accident; TIA, transient ischemic attack; ICA, internal carotid artery.
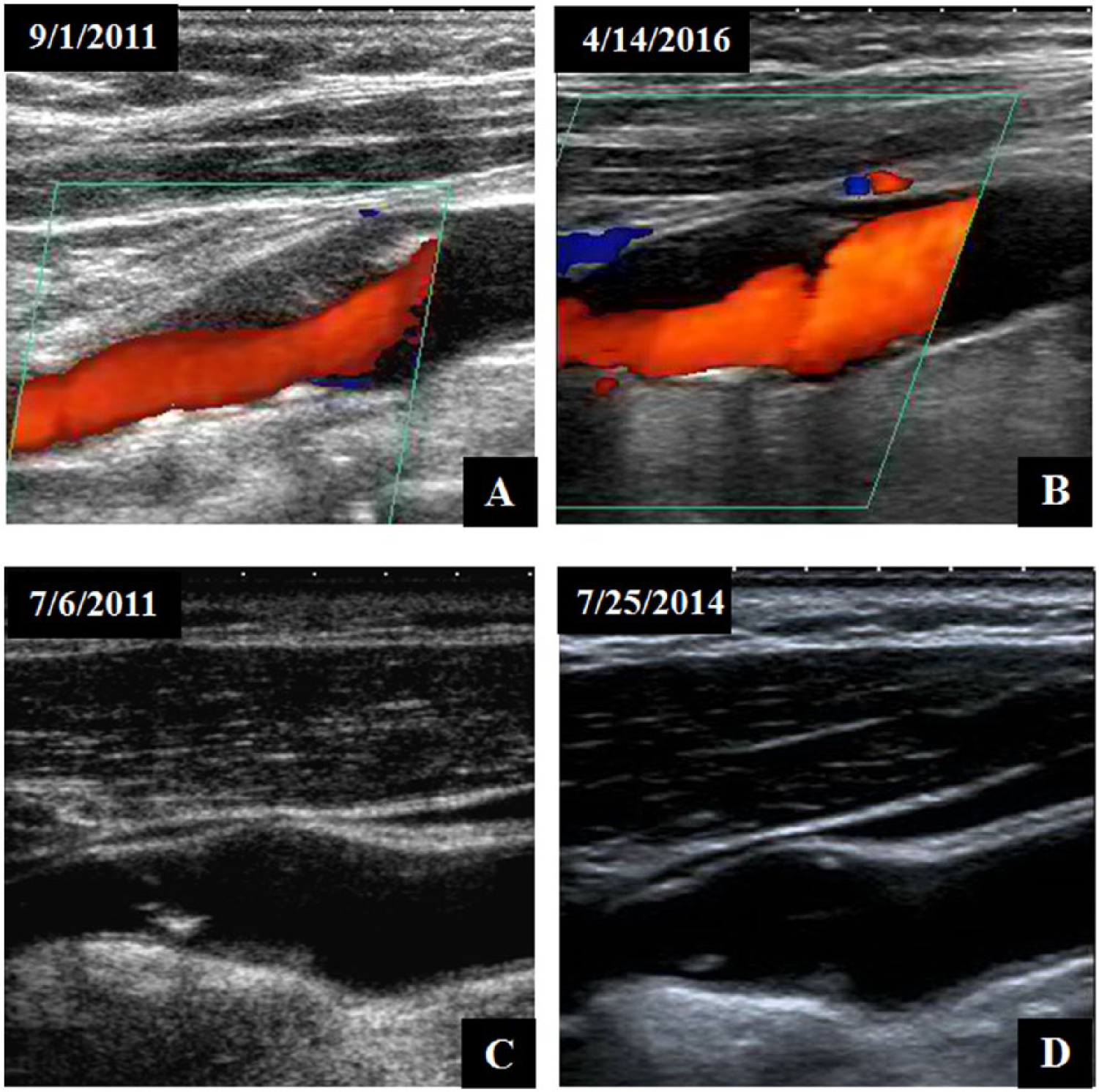
Carotid duplex ultrasound images of internal carotid arteries (ICAs) in two patients with mild carotid artery stenosis (CAS) on initial study (A, C) and no progression on follow-up (B, D). Images A and B are of the same ICA over 4 years apart and demonstrate a prominent heterogeneous plaque (imaged at slightly different magnifications and levels) with predominantly laminar flow. There is no significant morphologic or hemodynamic progression of disease over this time period. Images C and D are of a different patient and show the same ICA approximately 3 years apart and demonstrate visible plaque. There is some progression of the amount of plaque present but the percent stenosis remains <50% and the findings, therefore, do not lead to any change in management.
From the initial cohort of 440 ICAs, only 24 (5.5%) progressed to moderate CAS during the study period. There was no statistically significant difference between the ICAs that progressed to moderate CAS and those that did not regarding mean time between CUS, CAD, antiplatelet use, low-intensity statin use, high-intensity statin use, or current tobacco smokers. There was a statistically significant increase in the prevalence of HTN in the ICAs that progressed to moderate (68% vs 47%, p = 0.022). In the group that progressed to moderate CAS, there was a significantly higher number of those with a diagnosis of diabetes (44% vs 22%, p =0.008) as well as a significant decrease in moderate-intensity statin use (32% vs 58%, p = 0.005). Also, in the group with ICAs that progressed to moderate stenosis, there was a statistically significant increase in the number of patients not on statin therapy (36% vs 11%, p = 0.001). The ICAs in the group that progressed to moderate CAS did have an older mean age (77.4 ± 11.5) compared to the group that did not progress (76.5 ± 8.5), though it was not statistically significant. There was a trend toward increased males in the group that progressed to moderate CAS (76% vs 62%, p = ns). Not surprisingly, there were fewer never smokers (20% vs 34%, p = ns) and increased former smokers (68% vs 52%, p = ns) in the group with ICAs that progressed to moderate CAS, though neither was statistically significant. In the group of ICAs that did not progress, there was a lower prevalence of PVD (29% vs 40%, p = ns). There was not a statistically significant difference in incidence of CVA or TIA between the patients with carotids that progressed to moderate CAS and those that did not (13% vs 8%, p = ns) (Table 1). Of the entire cohort, 22% of the CVAs or TIAs occurred ipsilateral to the CAS, with 25% occurring in a different vascular distribution, and 53% of the vascular distributions were not documented.
Only one ICA of the initial 440 (0.2%) progressed from mild CAS to severe CAS within the study period. Statistical analysis was not performed on the carotid artery that progressed to severe stenosis during the study period due to low statistical power (n = 1). The single carotid that progressed to severe was in a 79-year-old male with risk factors of CAD, HTN, diabetes mellitus, HLD, and ongoing tobacco use. The patient was on a moderate intensity statin during the study period (Table 1).
A comparison of PSV and EDV at the initial CUS as well as at the follow-up study is shown in Table 2. ICAs were included for analysis if velocities at baseline and follow-up were reported. As expected, there was a statistically significant increase in the PSV from the initial CUS to the follow-up CUS in the group with ICAs that progressed to moderate (103 vs 149 cm/sec, p <0.01). There was also a statistically significant increase in EDV in the group of ICAs that progressed to moderate (24 vs 31 cm/sec, p <0.01). Interestingly, there was a significant difference between mean PSV in the group of ICAs that did not progress and those that progressed to moderate CAS at baseline (74 vs 103 cm/sec, p <0.01) and at follow-up (74 vs 149 cm/sec, p <0.01).
Comparison of PSV and EDV of ICAs at baseline and follow-up.
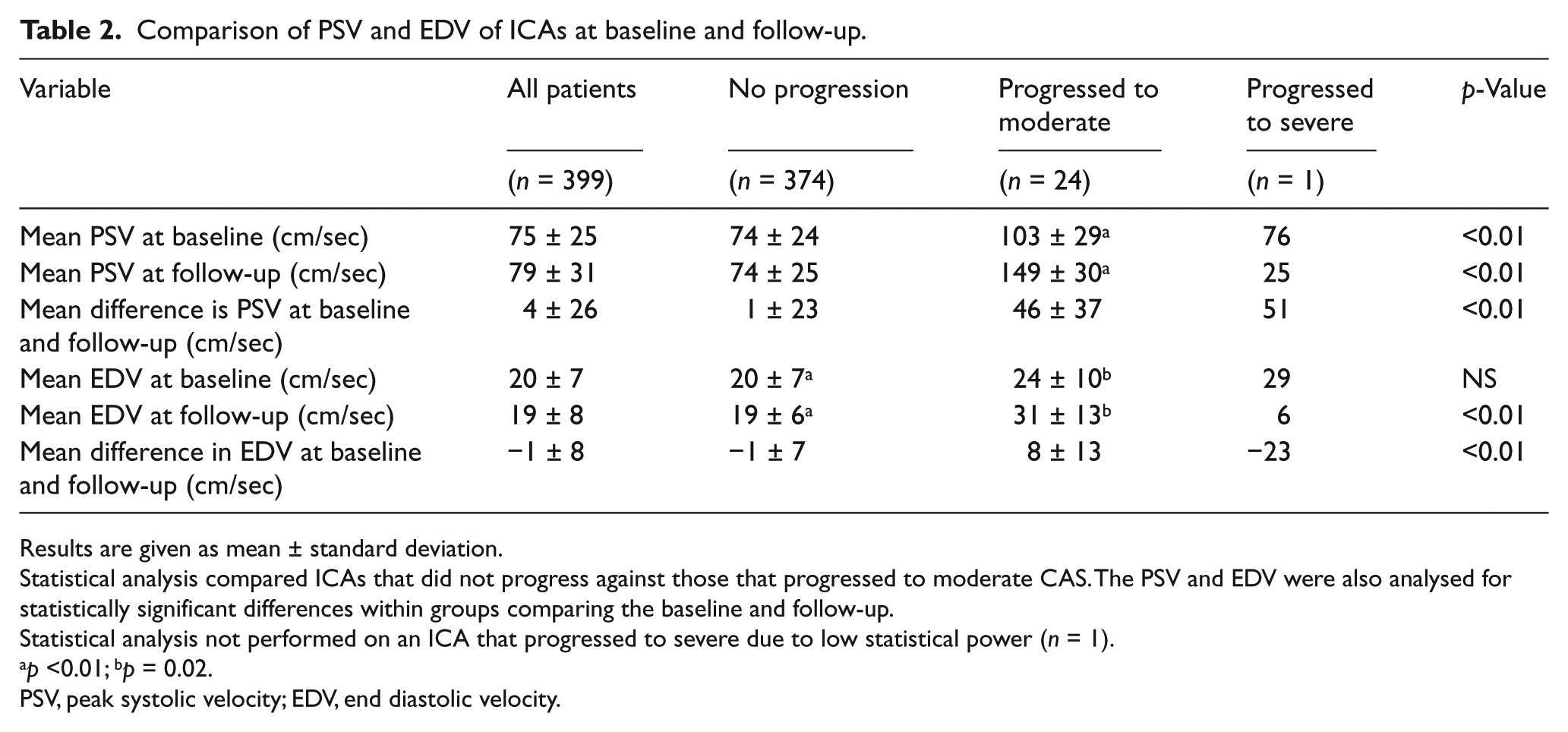
Results are given as mean ± standard deviation.
Statistical analysis compared ICAs that did not progress against those that progressed to moderate CAS. The PSV and EDV were also analysed for statistically significant differences within groups comparing the baseline and follow-up.
Statistical analysis not performed on an ICA that progressed to severe due to low statistical power (n = 1).
p <0.01; bp = 0.02.
PSV, peak systolic velocity; EDV, end diastolic velocity.
The indication for the initial CUS in each included ICA is shown in Table 3. The most common indication for the initial CUS was a history of known CAS, as seen in 23.9% of our population. Additional indications listed included screening (22.5%), presence of a carotid bruit (22.5%), pre-operative examination (13.2%), neurological symptoms (13.0%), and weak carotid pulse (1.6%), with 3.4% of the indications unknown (Table 3).
Indication for initial carotid artery duplex ultrasound.
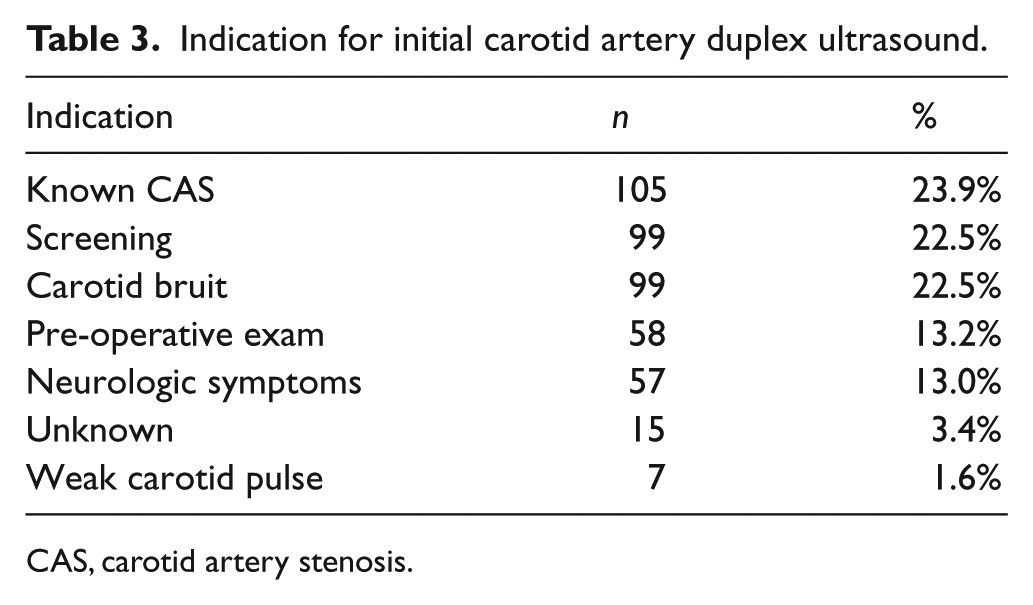
CAS, carotid artery stenosis.
Discussion
Our analysis demonstrated that few ICAs (5.5%) progressed from mild to moderate stenosis, and only one (0.2%) progressed from mild to severe stenosis during the 3- to 5-year follow-up (Table 1). The patient in whom the ICA progressed to severe was a 79-year-old male with a past medical history of HTN, HLD, CAD, peripheral vascular disease, and ongoing tobacco use (Table 1). The patient was on a moderate intensity statin during the study period. Upon discovery of the asymptomatic severe ICA stenosis, the patient was referred to vascular surgery for evaluation. Ultimately, the decision was made to treat the asymptomatic severe ICA stenosis with optimal medical therapy and defer invasive procedures given the patient’s comorbidities.
Of the 24 ICAs that progressed to moderate CAS during the study, our analysis revealed statistically significant increases in the prevalence of HTN and diabetes mellitus. Additionally, there was a non-significant trend toward increased PVD, HLD, and male sex in the group of ICAs that progressed to moderate CAS. With respect to tobacco use, patients with ICAs that progressed to moderate CAS were less likely to have been never smokers and more likely to be former smokers, though this was not statistically significant. Not surprisingly, there was a statistically significant increase in patients not on statin therapy and a significant decrease in moderate-intensity statin use in patients with carotids that progressed to moderate CAS (Table 1). The risk factors for progression in our study were consistent with others and reinforce the importance of statin therapy and lifestyle modification in patients with CAS. 16 This study demonstrates a significantly lower rate of progression of CAS compared to studies done in the 1990s, prior to the current era of optimal medical therapy. 16 Undoubtedly, a significant part of the decrease in progression of CAS is attributable to modern optimal medical therapy, especially statin therapy. This is supported by our data, which demonstrate a statistically significant decrease in moderate-intensity statin use and a statistically significant increase in patients not on statin therapy in the group of ICAs that progressed to moderate CAS.
One of the largest natural history studies of asymptomatic CAS, done in 1999 by Muluk et al., included all degrees of stenosis from none to completely occluded. Of the 306 ICAs with mild stenosis in this study, 38.2% progressed to greater than or equal to 50% stenosis at a mean time interval of 31 months. The percent that progressed from mild to severe disease, however, was not reported. 16 They, along with others, found that severity of baseline stenosis is a risk factor for progression, with moderate stenosis significantly more likely to progress than mild stenosis.11–13 Therefore, the question of how many patients with only mild stenosis will progress to severe disease over 3 years remains intriguing but not definitively answered. Accordingly, the 2012 ACCF AUC writing panel identified ‘Optimal frequency of ultrasound examinations for surveillance of untreated ICA stenosis, accounting for severity of disease on the baseline examination’ as an area in great need of focused research. 9 We hope our data analysis will be helpful in answering this question.
In addition to studies on the natural history of asymptomatic CAS followed by serial carotid duplex studies, there are two areas of ongoing research that may affect recommendations for appropriate surveillance. First is the question of whether revascularization of asymptomatic, severe CAS still confers a significant benefit over optimal medical therapy alone in the era of high intensity statin therapy for atherosclerosis. 17 A presumed benefit from revascularization is currently the main impetus for doing surveillance carotid duplex studies. The landmark clinical trials showing such a benefit occurred in the 1990s (ACAS, ACST) and it is unknown how the progress made in optimal medical therapy and the advances made in revascularization techniques will balance out in terms of risk and benefit.18,19 One trial aiming to address this question was stopped due to slow recruitment (SPACE-2), and another is not anticipating results until December 2020 (CREST-2). A second area of research relevant to carotid disease follow-up is whether techniques such as magnetic resonance angiogram (MRA), computerized tomography (CT), transcranial Doppler, 3D ultrasound, or risk scores can offer better predictive value than serial CUS and improve outcomes. 17
Limitations
The retrospective design and relatively small sample size of our study are limitations. Even taking into account differing definitions of ‘progression’, our cohort had a lower rate of progression than other studies. 16 With only a single ICA progressing to severe CAS during our study, we were unable to perform statistical analysis, which limited our ability to detect meaningful risk factors for progression to severe CAS. Additionally, our study population was drawn solely from a large cardiology practice, which may have affected the intensity of medical therapy and risk factor modification. We suspect that the slower rate of progression in our study group is secondary to improvements in medical therapy, which may have slowed progression compared to studies conducted prior to the improvement in optimal medical therapy. Our conclusion regarding a very low rate of progression of disease over 3 years needs to be validated by additional studies. Furthermore, the index carotid duplex in our study was defined as the first study done in the 10-year window of data we searched but did not in all cases represent the first carotid duplex study a patient had. Theoretically, this should increase the likelihood of progression, which increases with time. 16 This strengthens the conclusion that mild, asymptomatic CAS, at any point in time, can probably be safely checked at a 3-year, rather than 1-year, interval.
Conclusion
In conclusion, in our retrospective, observational study, the likelihood of mild, asymptomatic CAS progressing to severe CAS warranting consideration for revascularization over a 3- to 5-year follow-up period was very low (0.2%). We hope our findings will lessen the uncertainty acknowledged in the 2012 ACCF AUC regarding the optimal time interval between follow-up carotid duplex studies for this condition. If our findings are supported by others, then consideration might be given to changing the AUC for ‘surveillance of the plaque without narrowing noted on initial duplex examination or mild stenosis of <50%’. The current AUC deem any surveillance during the first year of follow-up inappropriate. Increasing the inappropriate time interval to repeat a carotid artery duplex for mild, asymptomatic CAS, particularly in patients on statin therapy with good control of their risk factors, to the first 3 years of follow-up would theoretically lessen the number of duplex studies performed, and thereby lessen health care costs, without compromising outcomes. We believe this is critically important in the era of value-based health care delivery.
Footnotes
Acknowledgements
We thank Aaron Vance for his assistance with compiling the patient database and Iowa Heart Center for allowing us access to their patient database and EMR.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.