
Abstract

Keywords
Impaired kidney function (IKF), defined as glomerular filtration rate (GFR)<60 mL/min/1.73 m2, affects 23–41% of elderly individuals and patients with cardiovascular disease. 1 IKF is independently associated with increased risk for cardiovascular events, 2 including stroke. 3 However, it is unclear whether IKF affects stroke severity and outcome.4–7 Moreover, most studies that evaluated this association used the Modification of Diet in Renal Disease equation (MDRD) to estimate GFR4,6,7 and only one applied the Chronic Kidney Disease Epidemiology Collaboration equation (CKD-EPI), 5 which appears to evaluate GFR more accurately. 8
To assess the effects of IKF on stroke severity and outcome, we prospectively studied all patients admitted in our department with acute ischemic stroke between September 2010 and March 2016 (n=922). GFR was calculated using creatinine measured at the first day after admission. Stroke severity was assessed at admission with the National Institutes of Health Stroke Scale (NIHSS). Severe stroke was defined as NIHSS≥5. The outcome was assessed with dependency at discharge (modified Rankin scale (mRS) 2–5) and in-hospital mortality.
Differences in categorical and continuous variables were assessed with the chi-squared test and independent samples t-test, respectively. Binary logistic regression analysis was used to identify independent predictors of severe stroke, dependency and mortality, including characteristics significant in univariate analysis. Two separate models were built, one with IKF defined according to MDRD and one with IKF defined according to CKD-EPI. When risk of other significant variables is presented, the effect size estimates are based on the model including IKF defined according to CKD-EPI.
Patients’ characteristics at admission are shown in Table 1. NIHSS did not correlate with GFR estimated with MDRD (r=−0.043, p=NS) but correlated with GFR estimated with CKD-EPI (r=−0.071, p<0.05). At admission, 55.2% of patients had severe stroke and a higher prevalence of IKF than patients with non-severe stroke when GFR was estimated with MDRD (38.8 vs 29.9%, respectively; p<0.05) or CKD-EPI (47.9 vs 36.6%, respectively; p<0.005). Independent predictors of severe stroke were age (relative risk (RR) 1.04, 95% confidence interval (CI) 1.02–1.06, p<0.001), atrial fibrillation (RR 1.95, 95% CI 1.44–2.64, p<0.001) and IKF according to CKD-EPI (RR 1.37, 95% CI 1.02–1.85, p<0.05).
Patients’ characteristics at admission.
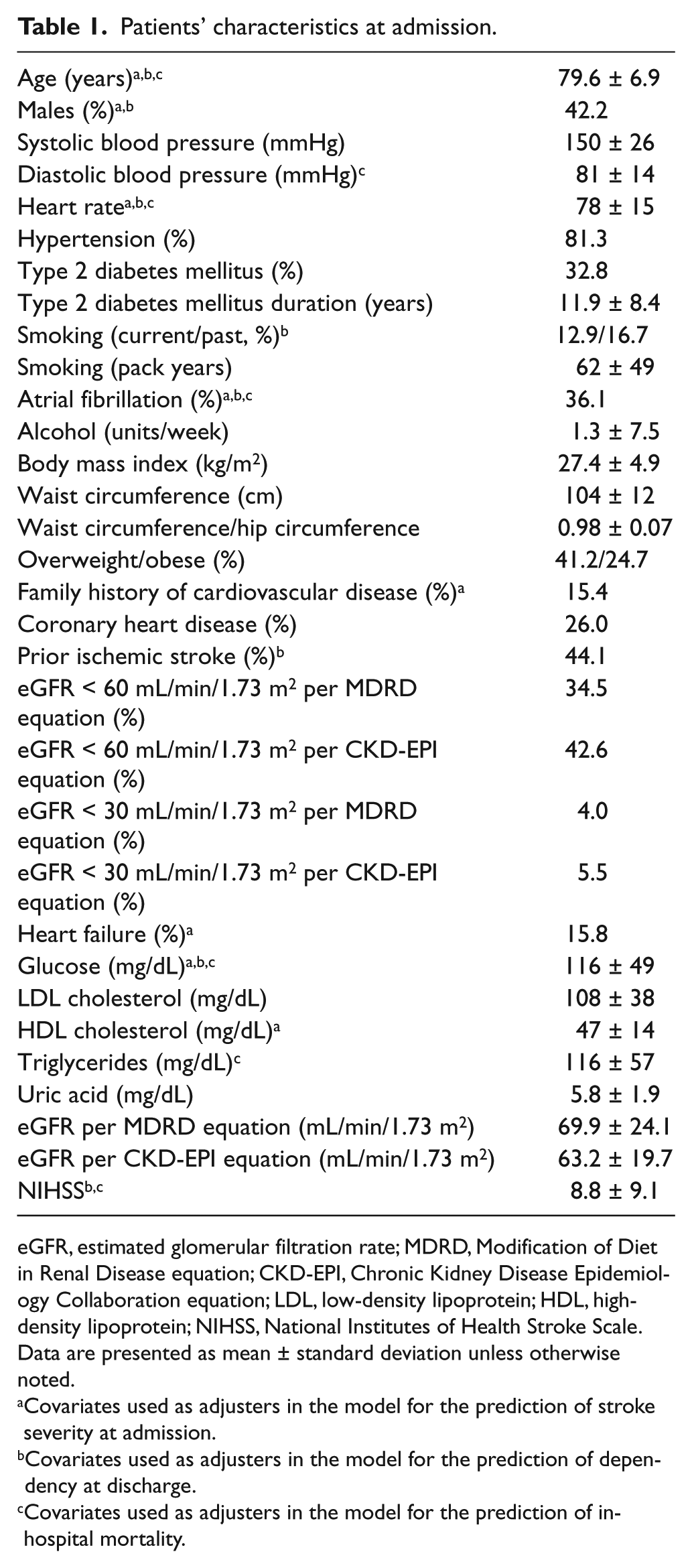
eGFR, estimated glomerular filtration rate; MDRD, Modification of Diet in Renal Disease equation; CKD-EPI, Chronic Kidney Disease Epidemiology Collaboration equation; LDL, low-density lipoprotein; HDL, high-density lipoprotein; NIHSS, National Institutes of Health Stroke Scale.
Data are presented as mean ± standard deviation unless otherwise noted.
Covariates used as adjusters in the model for the prediction of stroke severity at admission.
Covariates used as adjusters in the model for the prediction of dependency at discharge.
Covariates used as adjusters in the model for the prediction of in-hospital mortality.
At discharge, 60.8% of patients were dependent on others for performing usual activities. The prevalence of IKF according to CKD-EPI was higher in dependent than in independent patients (46.5 vs 37.2%, respectively; p<0.05) but the prevalence of IKF according to MDRD was similar (37.6 vs 31.9%, respectively; p=NS). Independent predictors of dependency were age (RR 1.08, 95% CI 1.04–1.12, p<0.001), history of ischemic stroke (RR 1.89, 95% CI 1.22–2.94, p<0.005) and NIHSS (RR 1.49, 95% CI 1.39–1.62, p<0.001).
During hospitalization, 9.4% of patients died. The prevalence of IKF did not differ between patients who died and those discharged regardless of whether IKF was defined according to MDRD (35.5 vs 34.4%, respectively; p=NS) or CKD-EPI (47.4 vs 42.1%, respectively; p=NS). GFR estimated with MDRD and CKD-EPI did not differ between the two groups (70±28 vs 70±24 mL/min/1.73 m2, respectively; p=NS, and 61±21 vs 63±19 mL/min/1.73 m2, respectively; p=NS). Independent predictors of mortality were diastolic blood pressure (RR 1.05, 95% CI 1.03–1.07, p<0.001) and NIHSS (RR 1.20, 95% CI 1.16–1.25, p<0.001).
A major finding of the present study is that IKF is independently associated with severe stroke only when CKD-EPI was used and not when MDRD was applied. Previous studies that evaluated this association included both patients with ischemic and hemorrhagic stroke 4 or did not adjust for differences between patients with and without IKF,4,5 and none applied both CKD-EPI and MDRD.4,5 Both equations include age, sex, race and creatinine for estimating GFR. 8 However, MDRD was developed in patients with CKD and systemically underestimates GFR at higher values 8 whereas CKD-EPI estimates GFR more accurately 8 and predicts cardiovascular events better. 9
GFR estimated with MDRD or CKD-EPI did not predict dependency or mortality. Notably, only one study (n=464) evaluated whether GFR estimated with CKD-EPI predicts short-term outcome after stroke and reported that patients with IKF had a higher mRS and mortality rate at 1 month after stroke; however, only unadjusted comparisons were performed. 5 Reduced GFR estimated with MDRD appears to predict in-hospital mortality 6 but the only study that evaluated its association with dependency at discharge was small (n=229) and did not identify a relationship. 7
In conclusion, GFR<60 mL/min/1.73 m2 evaluated with CKD-EPI appears to be associated with more severe ischemic stroke. In contrast, GFR estimated with MDRD does not appear to have predictive value. Therefore, physicians should utilize CKD-EPI instead of MDRD for evaluating kidney function in patients with acute ischemic stroke. Moreover, electronic medical record systems should also implement CKD-EPI. However, given that our findings are limited by the single-center and cross-sectional design of the study and the lack of power to evaluate the effects of GFR on mortality, more data are needed to validate our observations.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.