
Abstract
Isolated distal deep vein thrombosis (IDDVT) is a common clinical manifestation of venous thromboembolism (VTE). However, there are only scant and heterogeneous data available on the long-term risk of recurrent VTE after IDDVT, and the optimal therapeutic management remains uncertain. We carried out a retrospective cohort study of consecutive patients diagnosed with symptomatic IDDVT between 2004 and 2011, according to a predefined short-term treatment protocol (low molecular weight heparin (LMWH) for 4–6 weeks). The primary outcome was the occurrence of recurrent VTE. A total of 321 patients were enrolled. IDDVT was associated with a transient risk factor or cancer in 165 (51.4%) and 56 (17.4%) patients, respectively. LMWH was administered for 4–6 weeks to 280 patients (87.2%), who were included in the primary analysis. Overall, during a mean follow-up of 42.3 months, 42 patients (15%) developed recurrent VTE, which occurred as proximal DVT or PE in 21 cases. The recurrence rate of VTE per 100 patient-years was 3.5 in patients with transient risk factors, 7.2 in patients with unprovoked IDDVT, and 5.9 in patients with cancer (p=0.018). At multivariable analysis, unprovoked IDDVT and previous VTE were significantly associated with recurrent VTE (HR 2.16, 95% CI 1.12–4.16 and HR 1.97, 95% CI 1.01–3.86, respectively). In conclusion, the long-term risk of recurrent VTE after IDDVT treated for 4–6 weeks is not negligible, in particular in patients with unprovoked IDDVT or cancer. Further studies are needed to clarify whether a longer, but definite treatment duration effectively prevents these recurrences.
Keywords
Introduction
Isolated distal deep vein thrombosis (IDDVT) represents a common clinical manifestation of venous thromboembolism (VTE), ranging from 20% to 50% of all VTE events.1–3 IDDVT is commonly considered a benign disease, in particular when compared with proximal deep vein thrombosis (DVT), although up to 20–25% of IDDVTs extend to the proximal vein system,4–10 and 13–33% of IDDVTs are associated with asymptomatic pulmonary embolism (PE) at onset. 11
Despite this high incidence, scant and heterogeneous data are available on the clinical history of IDDVT.2,3 Information on the recurrence rates of the disease is hampered by the heterogeneity among studies in terms of initial treatment, duration of anticoagulation, duration of follow-up and definition of outcomes. A recurrence rate of 2–3% after 1 year was reported in some studies,12,13 whereas a higher rate up to 9–19% after about 2 years was reported in other studies.7,9
There is still uncertainty on the need to treat all cases of IDDVT and on the optimal duration of anticoagulation. 14 Current guidelines suggest that only selected patients diagnosed with IDDVT (i.e. those with severe symptoms or risk factors for extension) should be treated, and that in these patients anticoagulation should be given for a minimum of 3 months, as for patients with proximal DVT. 15 However, these recommendations are weak and mainly based on a low level of evidence. Indeed, a shorter course of anticoagulation (i.e. 4–6 weeks) was used in several studies6,8,12,16–18 and, when compared to longer durations,8,12,18 no significant differences were found on the incidence of recurrent VTE in some studies.12,18
Given the paucity and the heterogeneity of available information, we decided to perform a cohort study aimed at evaluating the long-term risk of recurrent VTE in consecutive patients diagnosed with symptomatic IDDVT, who received a short course of anticoagulant therapy according to a predefined local protocol, and were followed-up for at least 2 years.
Methods
We performed a retrospective study on a cohort of consecutive patients objectively diagnosed with symptomatic IDDVT between January 2004 and December 2011, who were followed as routine practice. The study was conducted at the Thrombosis and Haemostasis Center of the University Hospital of Varese, in Italy, which serves as a tertiary referral center for the diagnosis and treatment of patients with venous thromboembolism.
Diagnosis and follow-up
Based on the local management protocol, being active since 2004, all patients presenting with suspected DVT were evaluated by means of bilateral whole leg compression ultrasound. 19 All the examinations were registered on a computerized database, and patients diagnosed with IDDVT were scheduled for regular follow-up visits for up to 6 months, including an ultrasound evaluation at 6 months. In addition, all patients were instructed to immediately report to the center in case of signs or symptoms suggestive of recurrent DVT.
For the purpose of the study, patients were retrospectively identified by a systematic search of the center database. Patients were eligible if aged ⩾ 18 years and if no concomitant proximal DVT and/or PE were diagnosed. Asymptomatic PE was not systematically searched.
Relevant information was extracted from the electronic medical records on the index event and follow-up visits; follow-up was completed by telephone contact after a minimum of 2 years, performed by a physician using a follow-up form. Documentation was retrieved for any outcome event.
Treatment
According to the local protocol, based on the guidelines of the Italian Society for the Study of Haemostasis and Thrombosis (SISET), 20 patients were treated with low molecular weight heparin (LMWH) for 4–6 weeks, given at a full therapeutic dose for 1 week followed by 50% of that dose for 3–5 weeks. In case of contraindications to anticoagulation (e.g. active bleeding, high risk of bleeding, platelet count < 30,000/mm3, known allergy to LMWH or severe renal failure), treatment strategies were left to the treating physician, who decided on a case by case basis.
Study outcomes
The primary study outcome was the composite of objectively documented recurrent VTE, including symptomatic IDDVT, proximal DVT, PE or deep venous thrombosis in other sites. All events were locally adjudicated by consensus among three authors (MPD, FD, SP). Proximal DVT was adjudicated if documented by a compression or duplex ultrasound. Recurrent symptomatic IDDVT was adjudicated in case of ultrasound evidence of thrombosis of a previously normal vessel or in a previously completely recanalized distal venous segment. PE was adjudicated when documented by a positive computed tomography pulmonary angiography or high probability perfusion lung scan (in case of a previous PE event, the recurrent event was adjudicated in the presence of a previously normal or completely recanalized pulmonary artery segment or completely resolved perfusion defect).
Secondary outcomes were major bleeding, defined according to the International Society on Thrombosis and Haemostasis as fatal bleeding, and/or symptomatic bleeding in a critical area or organ (such as intracranial, intraspinal, intraocular, retroperitoneal, intra-articular or pericardial, or intramuscular with compartment syndrome), and/or bleeding causing a fall in hemoglobin level of 2 g/dL or more, or leading to transfusion of two or more units of whole blood or red cells, 21 and overall mortality. The incidence of all outcome events during follow-up in patients receiving a longer treatment duration is also reported.
The study adhered to the Helsinki Declaration. An ethical committee approval was not sought as this was a retrospective study on data already collected as part of routine clinical practice, according to a pre-existing local treatment and follow-up protocol. As per routine local practice, all patients signed an informed consent on personal data use for the purpose of the diagnosis and treatment, at the time of the index event. A verbal informed consent for the long-term follow-up was already obtained at the time of the telephone contact, which was not included in the local protocol but was part of a quality assurance activity.
Statistical analysis
Continuous data are presented with mean and standard deviations (SD) or median and interquartile range (IQR) according to their distribution, after applying the Kolmogorov–Smirnov test. A multivariable Cox-regression analysis was performed to calculate the hazard ratio (HR) and 95% confidence interval (CI) associated with potential predictors of recurrent VTE, after maintaining variables that resulted at least marginally significant (p<0.10) at the univariable analysis. IBM SPSS Statistics software, version 19 (IBM Corp., Armonk, NY, USA) was used for all the analyses.
Results
A total of 321 patients with IDDVT were included in the study. Baseline characteristics are presented in Table 1. According to the presence of underlying VTE risk factors, 165 IDDVTs (51.4%) were classified as provoked by transient risk factors (trauma 22.1%, surgery 9.3%, bed rest >3 days 8.1%, and oral contraceptives 8.4% were the most common), 55 (17.1%) were associated with cancer, and 96 (29.9%) were unprovoked; 72 patients (22.4%) had a previous VTE.
Baseline characteristics and treatment.
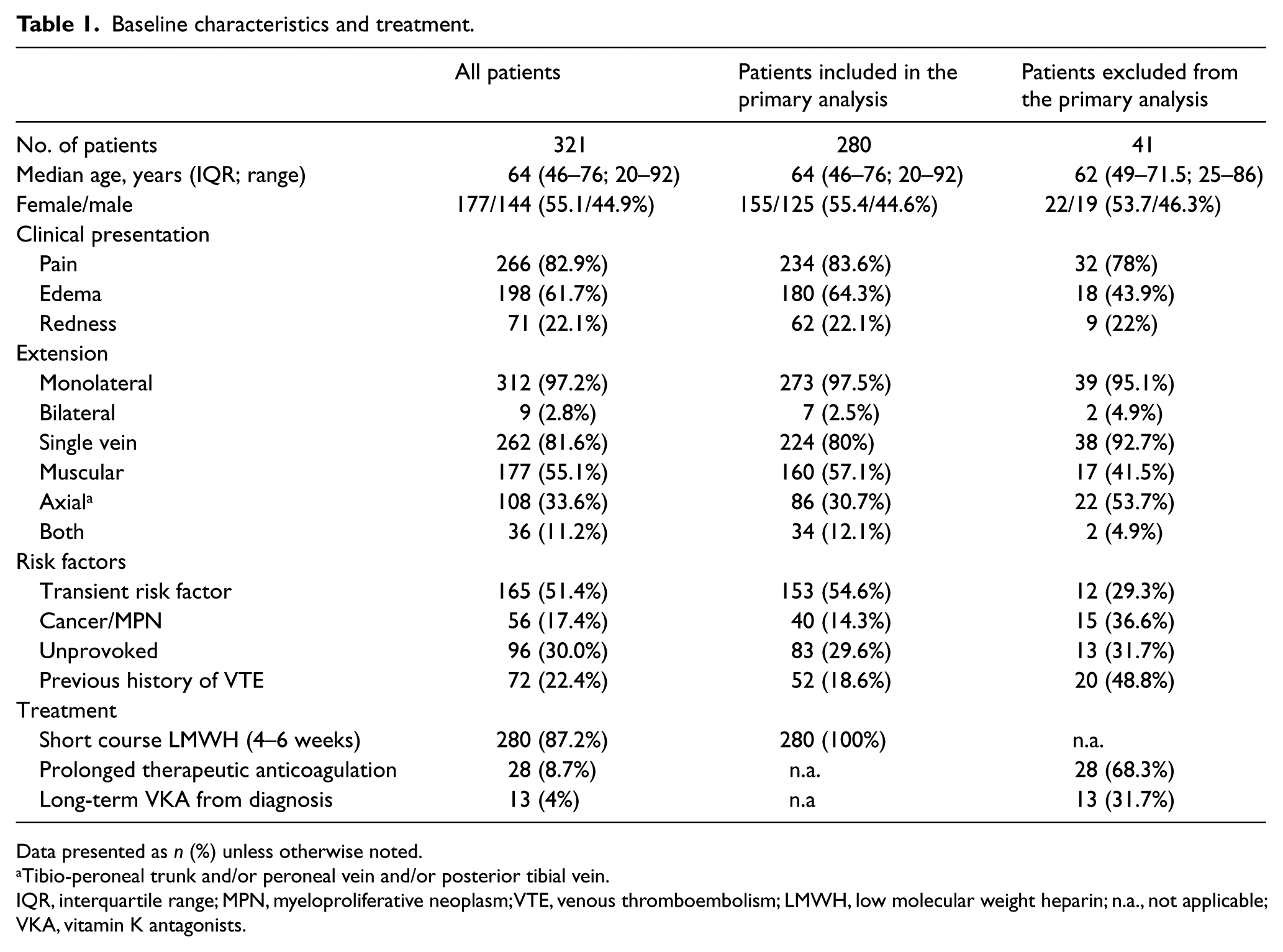
Data presented as n (%) unless otherwise noted.
Tibio-peroneal trunk and/or peroneal vein and/or posterior tibial vein.
IQR, interquartile range; MPN, myeloproliferative neoplasm; VTE, venous thromboembolism; LMWH, low molecular weight heparin; n.a., not applicable; VKA, vitamin K antagonists.
Among the 321 included patients, 13 (4%) were started on long-term VKA at the time of IDDVT diagnosis because of previous major VTE, leaving 308 patients (96%) eligible for the 4–6 weeks LMWH treatment regimen. Of them, 28 patients were continued on therapeutic anticoagulation after the initial 4–6 weeks, based on the decision of the treating clinician at the first follow-up visit, because of the presence of active cancer, pregnancy or other conditions (Figure 1).
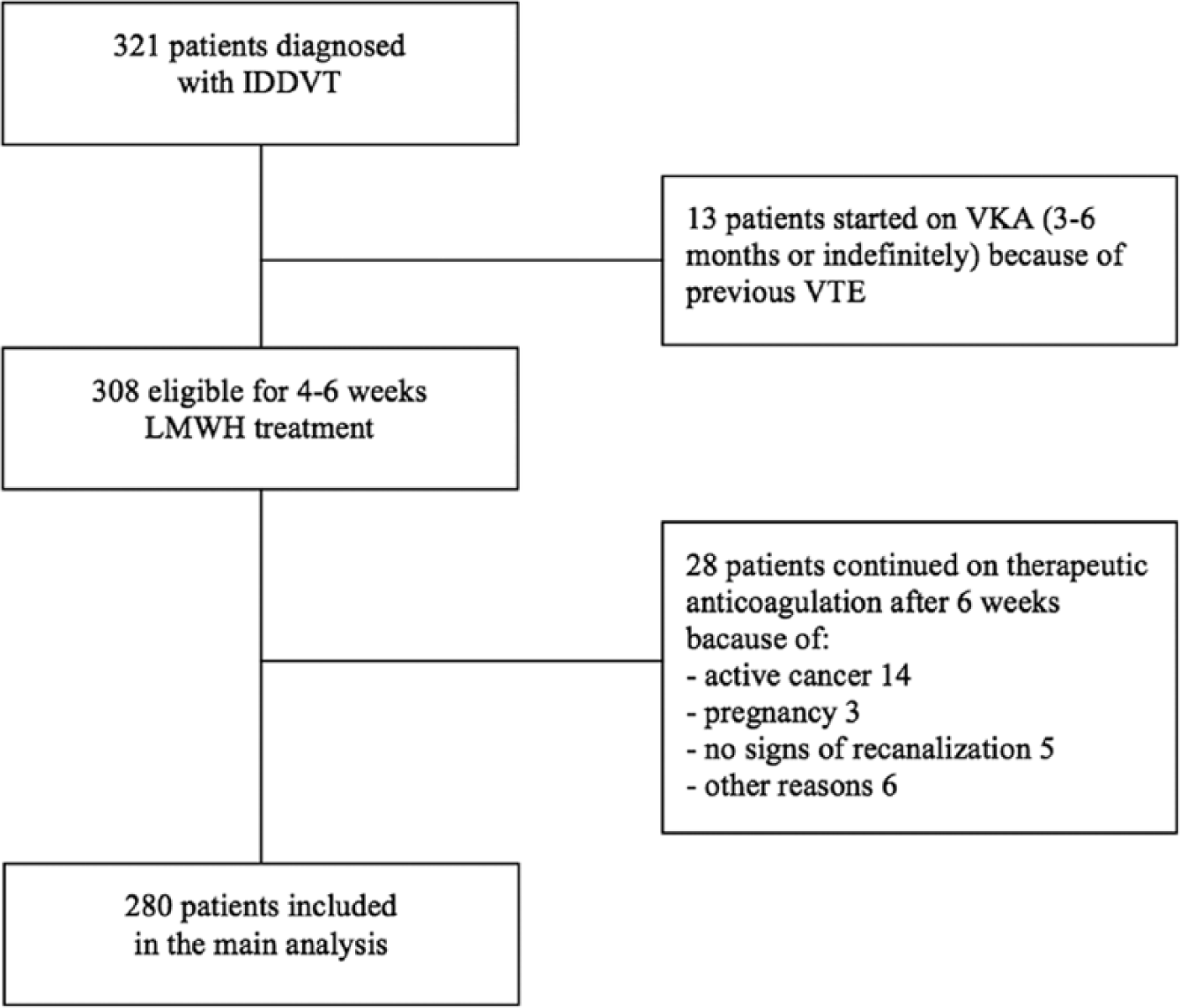
Study population. IDDVT, isolated distal deep vein thrombosis; VKA, vitamin K antagonists; VTE, venous thromboembolism; LMWH, low molecular weight heparin.
Therefore, 280 patients were included in the primary analysis (Table 1). Of them, 10 patients (3.6%) received a shorter course of LMWH because of anemia and/or thrombocytopenia at onset (seven patients) or because of previous bleeding complications (three patients). Finally, four patients (1.4%) had LMWH treatment stopped by their general practitioner before the completion of a period of at least 4 weeks with apparently no clinical reasons.
During a mean follow-up of 42.3 months (SD 27.8), 42 patients (15%) experienced symptomatic recurrent VTE, for an annualized recurrence rate of 4.4 per 100 person-years (95% CI 3.3–5.9). Recurrent VTE events were represented by recurrent IDDVT in 19 patients (45.2%), proximal DVT in eight patients (19%), PE in 13 patients (31%), and deep venous thrombosis in other sites in two patients (4.8%) (Table 2 and Figure 2).
Results of the primary analysis and on patients excluded from the primary analysis.
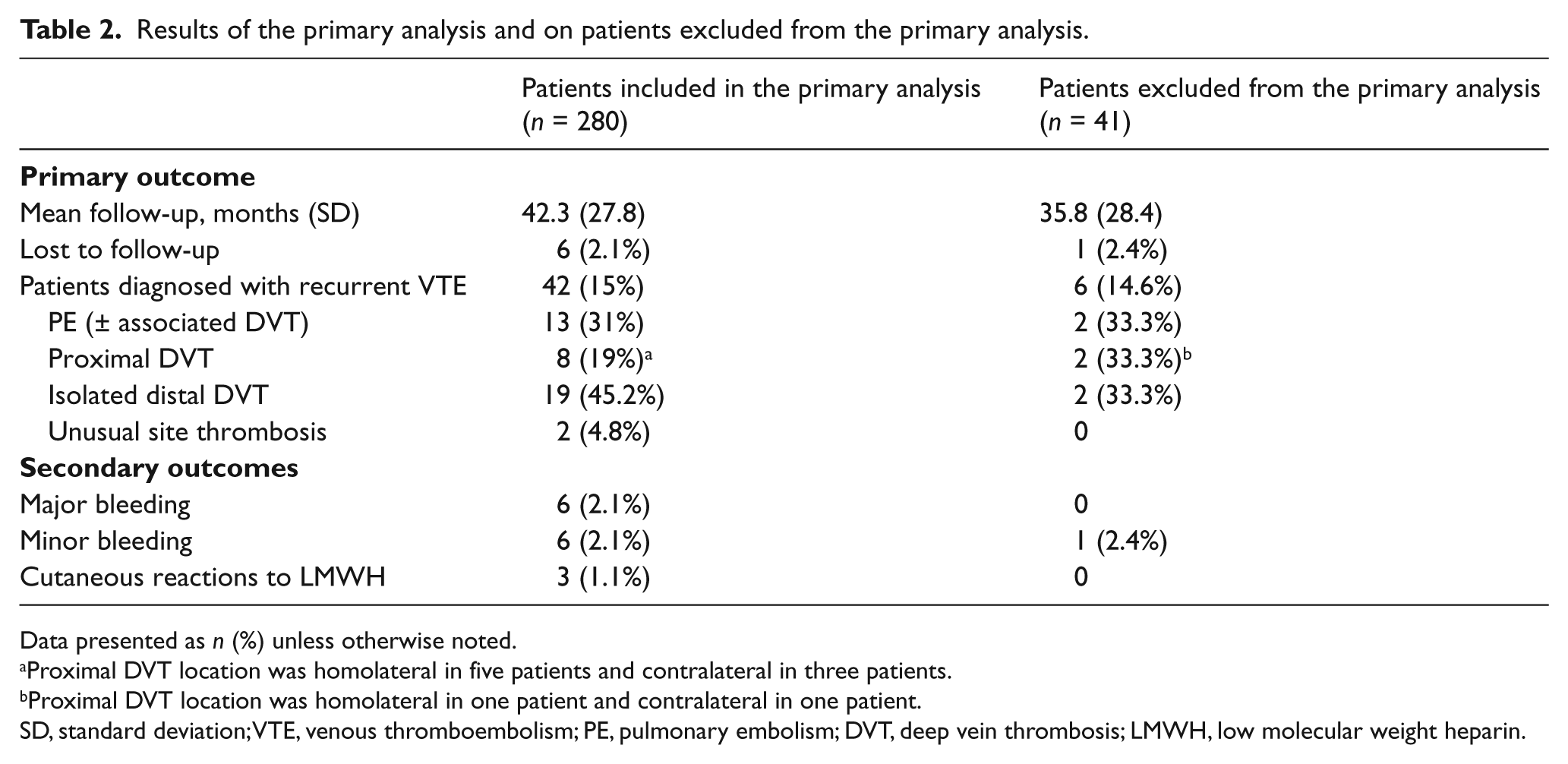
Data presented as n (%) unless otherwise noted.
Proximal DVT location was homolateral in five patients and contralateral in three patients.
Proximal DVT location was homolateral in one patient and contralateral in one patient.
SD, standard deviation; VTE, venous thromboembolism; PE, pulmonary embolism; DVT, deep vein thrombosis; LMWH, low molecular weight heparin.
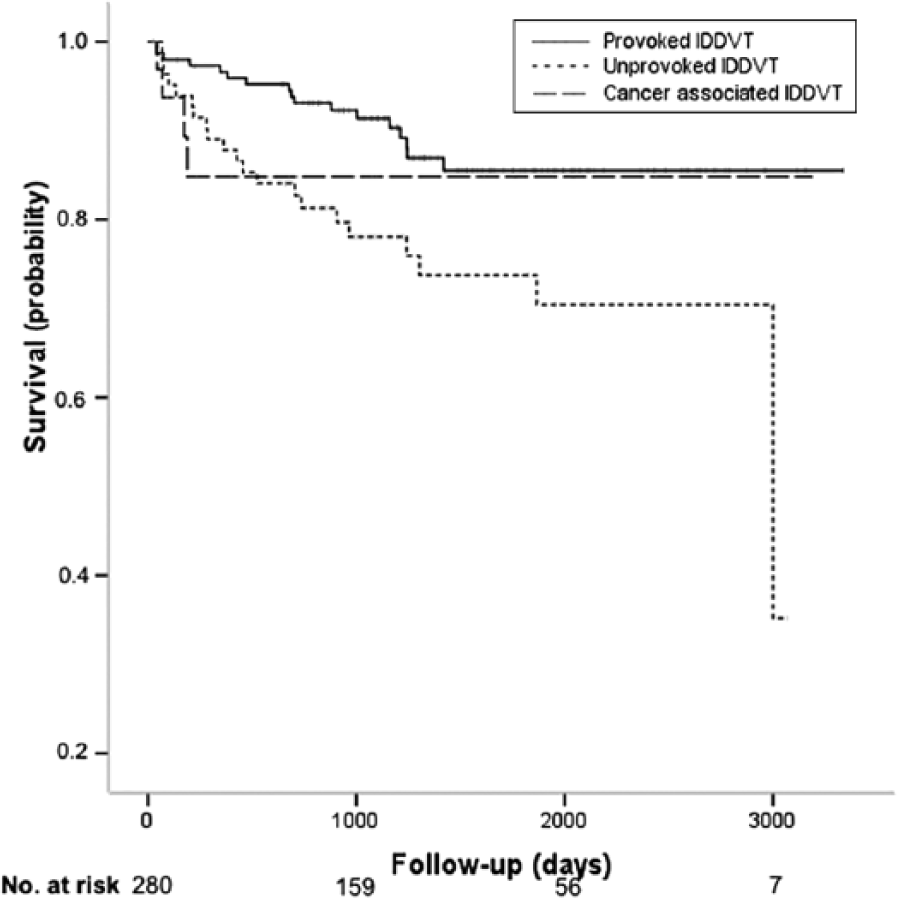
Kaplan–Meier VTE recurrence-free survival curve.
Table 3 shows the results of univariable and multivariable analysis. Among potential predictors of recurrence, only unprovoked IDDVT and a previous history of VTE remained significantly associated with recurrent VTE at multivariable analysis (HR 2.16, 95% CI 1.12–4.16 and HR 1.97, 95% CI 1.01–3.86, respectively). The annualized rate of recurrent VTE was 7.2 per 100 patient-years after unprovoked IDDVT (95% CI 4.8–10.8) and 5.9 per 100 patient-years after IDDVT associated with active cancer (95% CI 2.3–14.1), as compared with 3.5 per 100 patient-years after provoked IDDVT (95% CI 2.9–4.5) (p = 0.018, log-rank test).
Cox-regression analysis on the population included in the primary analysis.
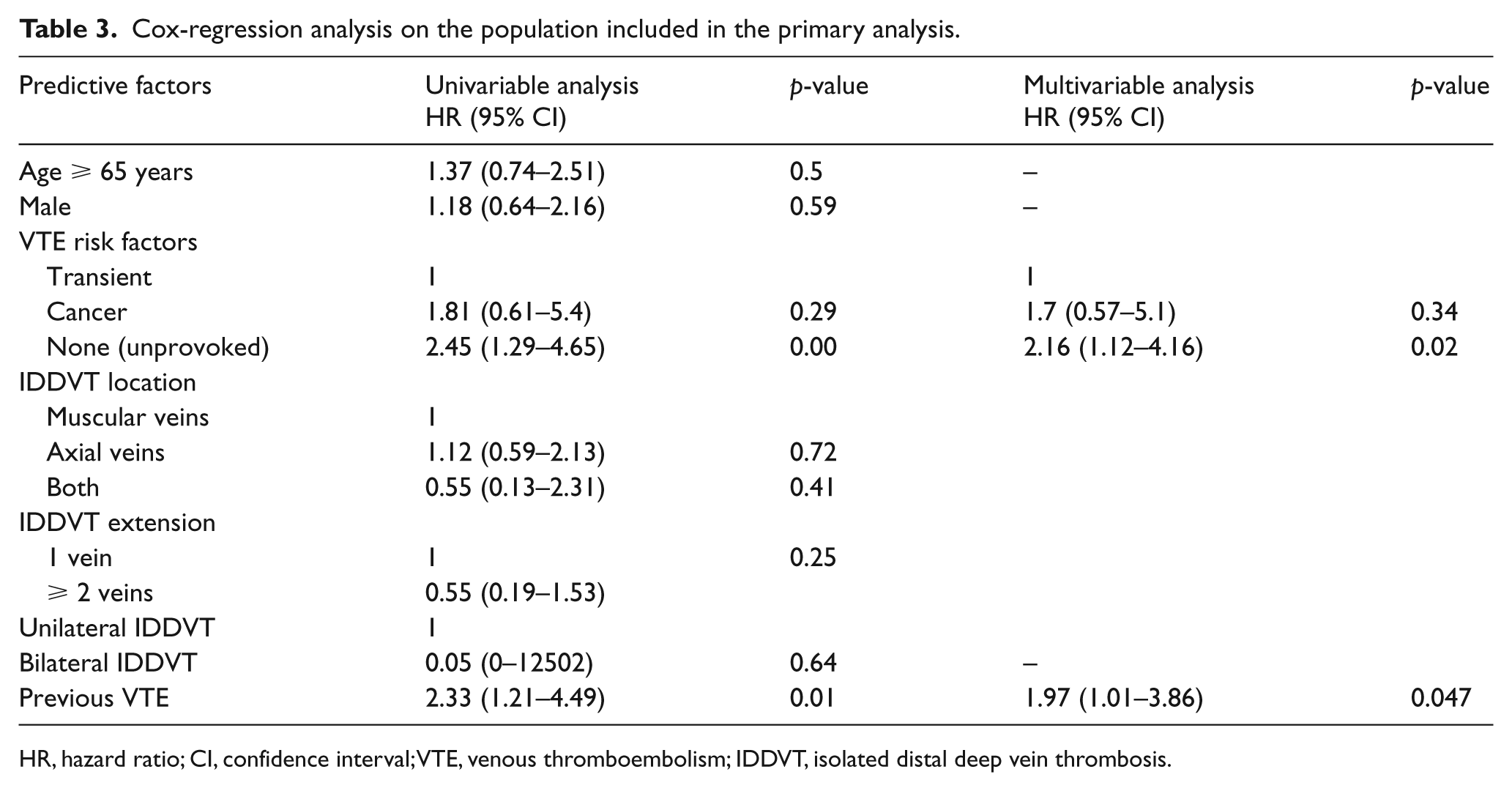
HR, hazard ratio; CI, confidence interval; VTE, venous thromboembolism; IDDVT, isolated distal deep vein thrombosis.
During anticoagulant treatment, six patients (2.1%) experienced major bleeding, none was fatal. During the entire follow-up period, 48 patients (17.1%) died. Follow-up was complete for 97.5% of patients (seven patients were lost to follow-up), and data on mortality were retrieved for 98.9% of patients (three were lost to follow-up).
Discussion
In this large cohort study of patients with symptomatic IDDVT treated with a short course of anticoagulant therapy, the incidence rate of recurrent VTE was not negligible (4.4 per 100 patient-years), with half of recurrences occurring in the proximal veins or as PE. Recurrence rates were significantly higher in patients with an index unprovoked event (7.2 per 100 patient-years), as compared to patients with a transient provoking factor (3.5 per 100 patient-years).
Previous studies on IDDVT were quite heterogeneous in terms of number of patients enrolled, type and duration of treatment and follow-up. In two randomized controlled trials, the recurrence rate of VTE after IDDVT was found to be 4% and 2.6% after 12 and 15 months of follow-up, respectively, in patients who received anticoagulation for 12 weeks or 6/12 weeks, respectively.12,22 Higher cumulative rates of recurrence were described in more recent observational studies, which present, however, some important limitations.9,23 Finally, data on a large number of patients with IDDVT (almost 2000) are available from the international RIETE registry, but the duration of follow-up was of 3 months only, during which 2% of patients experienced recurrent VTE. 24 Therefore, our study may be considered innovative and shows several strengths: being conducted on a large number of patients treated homogenously and followed for more than 3 years, with negligible loss to follow-up (< 3%).
More recently, the results of a multicenter prospective cohort study enrolling 490 patients were published (OPTIMEV study). 13 Differently from our study, patients with cancer or a previous history of VTE were excluded and therapeutic anticoagulation was given for the entire duration of treatment, which was longer than in our study (median 92 days, IQR 61–123 and 42 days, IQR 35–42, respectively). These differences may explain the lower rate of recurrent VTE in the OPTIMEV study as compared to our study, both in the overall population (2.7 and 4.4 per 100 patient-years, respectively) and in patients with provoked IDDVT (1.4 and 3.5 per 100 patient-years, respectively) or unprovoked IDDVT (3.8 and 7.2 per 100 patient-years, respectively). One similarity between the OPTIMEV study and our study was in the failure to find any significant difference in the risk of recurrent VTE between patients presenting with axial vein involvement and patients with muscular vein involvement. Differently from the OPTIMEV study, we did not find older age and increasing number of involved veins to be associated with recurrent VTE at multivariable analysis.
The results of our study confirm that the risk of recurrent VTE after treated IDDVT is relevant in patients with an unprovoked event or with previous VTE. In patients with unprovoked IDDVT we found a 25.3% cumulative incidence of recurrent VTE after 3.5 years. Interestingly, half of the events occurred during the first year, for a cumulative incidence of 12% at 1 year, an incidence that is quite similar to that of proximal DVT or PE (15% at 1 year, 26% at 3 years).25,26
In patients with IDDVT and cancer, we found a 18.2% cumulative incidence of recurrence at 1 year. Of particular note, recurrent events were represented by PE in three out of four patients. The rate of recurrent VTE after cancer-associated IDDVT was not statistically different from that occurring after IDDVT associated with transient risk factors, probably due to the small number of cancer patients included in the primary analysis (40) and to a selection bias after the exclusion of 16 additional patients who received a longer treatment duration because of a perceived higher risk of recurrence due to the activity of the underlying malignancy. Recent consensus guidelines on the treatment of VTE in cancer patients and clinical practice data from international surveys do not specifically consider the issue of IDDVT. 27 Given the observed risk of recurrence, additional evidence is urgently needed.
Current guidelines and guidance statements suggest that anticoagulation for IDDVT should be given for a minimum of 3 months, as for patients with proximal DVT.15,28 However, this recommendation is based on a low level of evidence. The results of our study show that a short course of anticoagulation (4–6 weeks) may be sufficient for a substantial proportion of patients, such as those with IDDVT associated with transient risk factors. The efficacy of this approach, at least for this subgroup, is confirmed by the results of a number of studies6,8,12,16–18 and a similar short-course heparin treatment (6 weeks) was used in a recently published randomized controlled trial. 29 Conversely, a longer treatment duration appears to be necessary in higher risk subgroups, such as patients with unprovoked VTE or with cancer, or patients with previous VTE. However, whether a treatment duration of 3 months is sufficient to prevent recurrences in these subgroups remains to be better established by clinical trials.
Limitations
Our study has limitations. First, the observational design can be associated with incomplete and/or inaccurate data. However, information was collected and electronically recorded, according to a pre-existing internal protocol, so minimizing the risk of incompleteness. Moreover, all patients underwent a telephone interview at least 2 years after the index event and only a few were lost to follow-up.
Second, there is a potential risk of recall bias if patients contacted during follow-up reported as recurrent VTE events some episodes that were only suspected. For this reason, we requested and carefully checked all available clinical documentation in order to adjudicate objectively diagnosed events only, thus minimizing the risk of overestimating recurrence rates. On the other hand, we may have underestimated the recurrence rate, since only symptomatic events were considered. However, this approach may better resemble the usual clinical practice.
Third, although the internal protocol indicated a course of LMWH for 4–6 weeks for all patients, the final decision was left to the attending physician. Reasons for changes to the protocol were heterogeneous, although predominantly related to the perceived persistence of major risk factors for recurrence (i.e. active cancer and pregnancy). However, about 90% of patients received LMWH according to the protocol and the primary analysis was restricted to this population.
Conclusions
In conclusion, the results of our study show that the long-term risk of recurrence in patients with IDDVT treated with a short course of LMWH is not negligible. This therapeutic approach appears to be sufficient for patients with IDDVT secondary to transient risk factors, whereas patients with unprovoked IDDVT or cancer and those with previous VTE events may benefit from a longer treatment period. Future studies should try to assess the optimal duration of treatment in these patients and to identify IDDVT patients who may deserve extended anticoagulation.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.