
Abstract

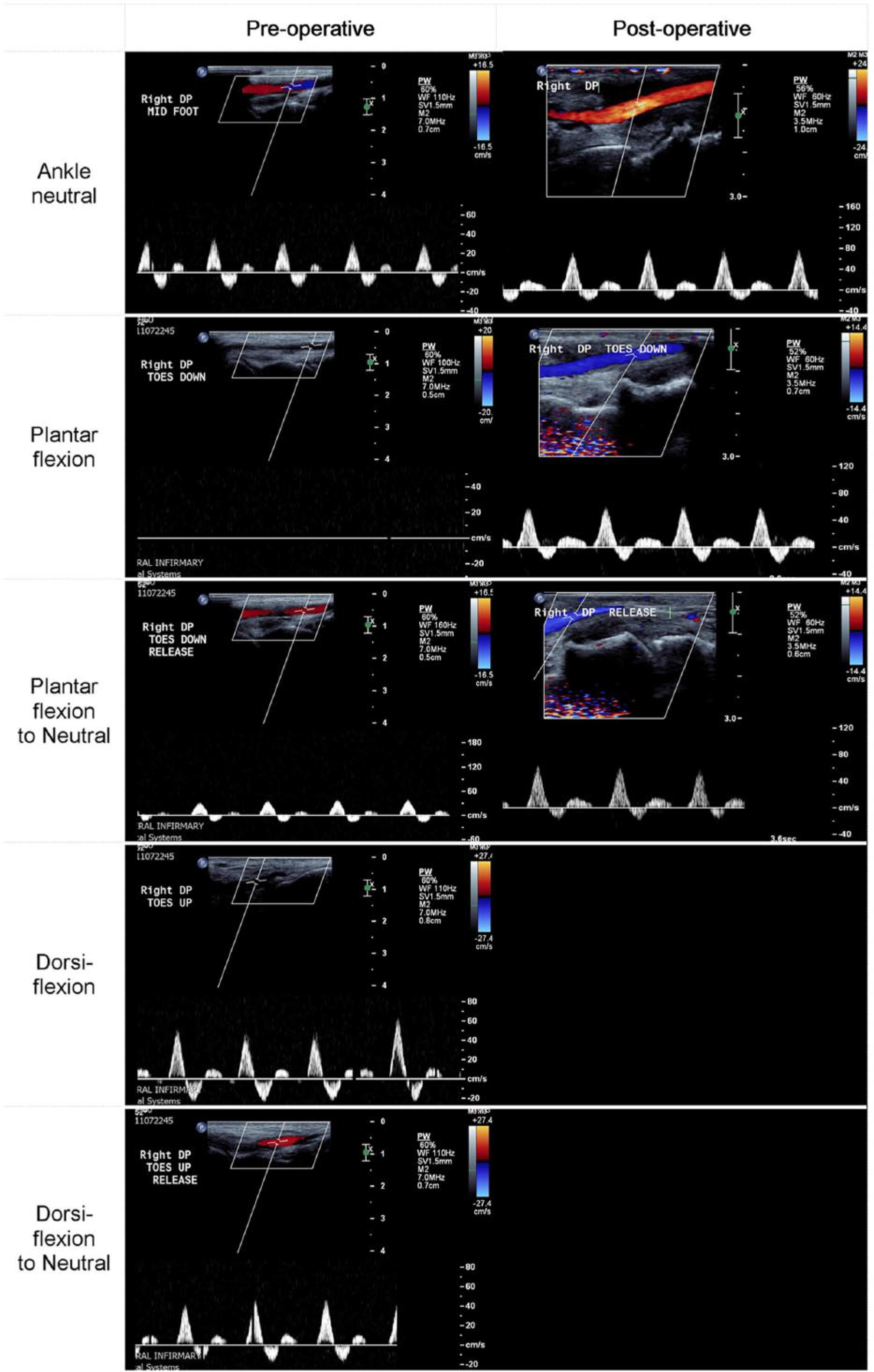
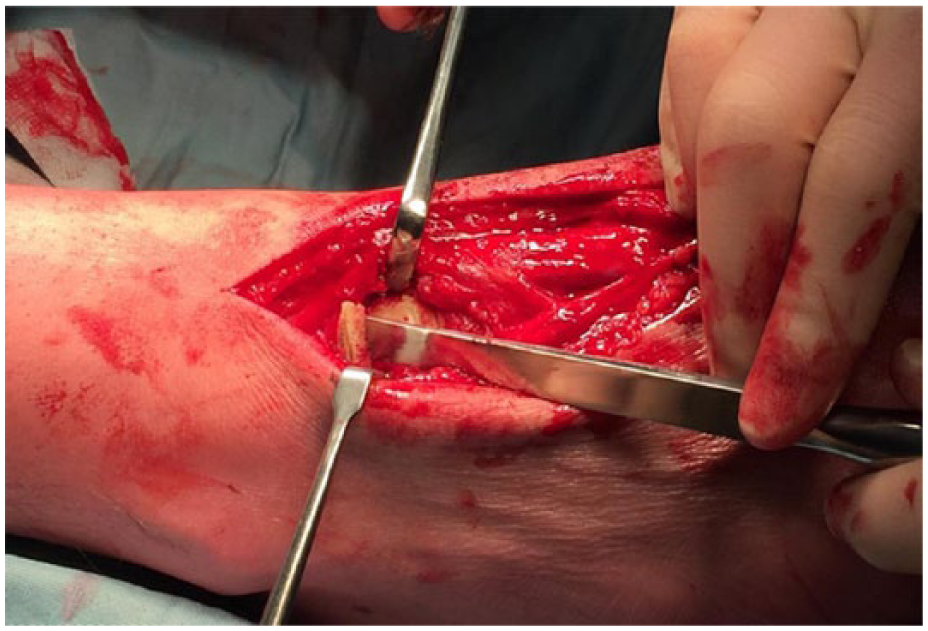
A 46-year-old self-employed property developer, under surveillance for a thrombosed left dorsalis pedis artery (DPA) secondary to impingement, presented with a 4-month history of discomfort and numbness of the right foot. Symptoms were most marked whilst kneeling (Panel A). He had no other co-morbidities, although he weighed 123 kg. On examination, pallor of the plantar aspect of the left foot was evident after a period of standing, despite angiographic evidence of a patent posterior tibial artery and medial and lateral plantar arches. Magnetic resonance angiography of both legs in the neutral position demonstrated no significant disease of vessels proximal to the foot. Duplex ultrasound imaging of the right foot in the neutral position demonstrated patency of the DPA with a triphasic waveform (Panel B; pre-operative). Plantar flexion of the right foot highlighted signs of entrapment and forced plantar flexion resulted in complete cessation of flow, features which resolved on neutralizing these manoeuvres. Operative intervention was undertaken. Thickened tissue bands were divided deep to the tendon of the extensor hallucis brevis (EHB), which appeared to be compressing the DPA on extreme plantar flexion. Exostosis of the talus was also removed, as it was causing bow stringing of the DPA, which was amplified on plantar flexion (Panel C). The patient recovered with complete resolution of symptoms. Surveillance duplex ultrasonography of the right foot at 6 months demonstrated normal triphasic antegrade flow in the DPA (Panel B; post-operative).

Primary vascular atherosclerotic disease is rare in young adults. Symptoms related to anatomical positioning in this patient group should prompt assessment for extra-vascular anatomical impingement. To date, causes described have been limited to the encroachment of the EHB tendon running superficial to the DPA or anomalous fibrous bands.1,2 These anatomical features are the consequences of intense physical activity leading to overuse injury and remodelling. We present a case of bilateral dorsalis pedis impingement, which is unique in highlighting bony remodelling to compromise the passage of the DPA. Our case, along with the case described by Smith et al., implicates occupation to be a potential risk factor leading to the development of dorsalis pedis entrapment syndrome. 1 There also appears to be a tendency towards developing bilateral impingement, which is exemplified by existing case reports.1,2 This case highlights the importance of surveillance in patients with unilateral impingement so that contralateral impingement may be identified early and corrective surgery undertaken to prevent complications and subsequent lifestyle limiting symptomology.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.