
Abstract

Deep vein thrombosis (DVT) is commonly unsuspected and under-diagnosed in intensive care unit (ICU) patients. 1 Screening for DVT with lower extremity ultrasound (LEUS) has been suggested in ICU patients but has not been proven beneficial, 2 and guidelines recommend against this practice. 3 At our hospital, LEUS is routinely performed to screen for asymptomatic DVT prior to sequential compression device (SCD) application to avoid the theoretical risk of causing pulmonary embolization (PE) of pre-existing DVT.
We evaluated whether screening for asymptomatic DVT with LEUS is warranted prior to SCD application in adult ICU patients with contraindications to anticoagulation. We specifically assessed asymptomatic DVT prevalence, outcomes and risk factors, and the delay in SCD application associated with LEUS.
ICU patients who underwent LEUS to screen for asymptomatic DVT prior to SCD application were identified retrospectively using the American University of Beirut Medical Center (AUBMC) vascular laboratory records. Of 325 patients who underwent LEUS in the AUBMC ICUs (medical, surgical, and neurology) from 10/2011 to 6/2013, 68 were excluded (18 for suspected DVT, nine for known DVT or PE, and 41 on anticoagulation), resulting in 257 patients. The AUBMC-Institutional Review Board approved this study.
A certified ultrasound technologist performed whole LEUS using Philips CX30-ultrasound (Philips Healthcare, The Netherlands). A vascular surgeon reviewed all studies.
Data were collected from medical records. Risk factors for DVT were systematically recorded for all patients as part of the AUBMC DVT-prophylaxis protocol. Indication, results, date and time of LEUS order, test, and report, and date of SCD application were collected.
Independent predictors of asymptomatic DVT were evaluated using logistic regression that included all DVT risk factors. Vital status at discharge was compared for patients with or without asymptomatic DVT and for patients with asymptomatic DVT who were or were not treated with anticoagulation. Delay in SCD application after admission and ordering LEUS was calculated.
Eighteen of 257 patients had asymptomatic DVT (a prevalence of 7%), of which 13 were proximal (iliac, femoral and popliteal veins) and five were calf DVT.
Six were in neurology-ICU, 10 in medical-ICU, and two in surgical-ICU. Three patients with asymptomatic DVT had a seizure diagnosis (n=10, 30%), three had an intracerebral bleed (n=38, 7.9%), one had pancreatitis (n=6, 16.7%), one had a gastrointestinal bleed (n=11, 9.1%), one had respiratory failure (n=17, 5.9%), and nine had sepsis (n=115, 7.8%). Factors associated with asymptomatic DVT are presented in Table 1; prior DVT (adjusted odds ratio (OR)=47.4, 95% CI: 3.9–575.4), thrombophilia (adjusted OR=20.2, 95% CI: 3.2–126.8), and recent surgery (adjusted OR=4.1, 95% CI: 1.1–14.9) were significant predictors in multivariable adjusted analyses.
Characteristics of the study sample, stratified by presence of deep venous thrombosis (DVT), n=257.
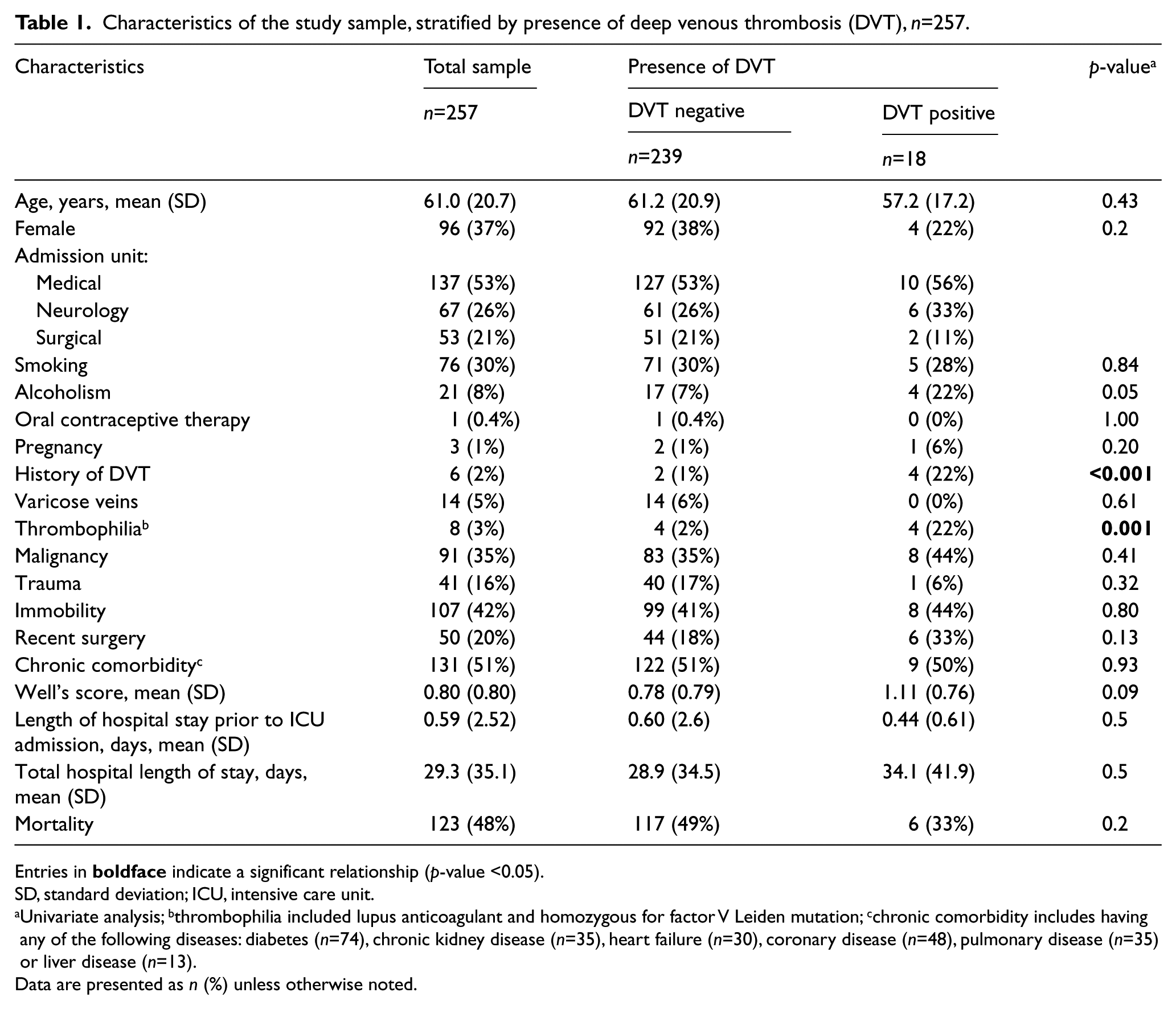
Entries in
SD, standard deviation; ICU, intensive care unit.
Univariate analysis; bthrombophilia included lupus anticoagulant and homozygous for factor V Leiden mutation; cchronic comorbidity includes having any of the following diseases: diabetes (n=74), chronic kidney disease (n=35), heart failure (n=30), coronary disease (n=48), pulmonary disease (n=35) or liver disease (n=13).
Data are presented as n (%) unless otherwise noted.
Mortality was 33.3% in patients with asymptomatic DVT and 49.2% in patients with a negative LEUS (p=0.2). Among 18 patients with asymptomatic DVT, 12 received therapeutic-dose heparin, two received prophylactic-dose heparin, three received an inferior vena cava filter and one was untreated; six died, of whom one had PE with cardiorespiratory arrest. All patients who died were treated for DVT, while none of the three patients who were untreated or given prophylactic-dose heparin died.
The median delay in SCD application was 2.0 [interquartile range (IQR): 1.0–5.0] days after ICU admission, and 1.0 [IQR: 0.8–2.0] day after ordering a SCD. Median delays were 0.0 [IQR: 0.0–2.0] days between admission and ordering LEUS; 1.0 [IQR: 0.0–2.0] day between ordering and performing LEUS; and 0.0 [IQR 0.0–0.0] days between performing LEUS and ordering a SCD. Patients without contraindications received a pharmacologic prophylaxis within hours from admission following the AUBMC protocol.
This is the first study that evaluates LEUS screening for asymptomatic DVT prior to SCD application. SCDs are recommended for DVT prophylaxis in ICU patients with contraindications to anticoagulation. 3 SCDs are thought to decrease the risk of DVT by enhancing blood flow in the lower extremities; however, if DVT is present, the movements could theoretically enhance embolization. Nevertheless, our findings suggest that applying SCDs without prior screening for DVT with LEUS could avoid unnecessary delay in DVT prophylaxis while being unlikely to affect outcomes negatively.
The presence of asymptomatic DVT in this population with contraindications to pharmacologic prophylaxis due to bleeding risk was low, but was associated with prior DVT, thrombophilia, and recent surgery. Thrombophilia and prior DVT were similarly identified as DVT risk factors in a prior ICU-based study 1 and could be used in the prospective validation of risk models for screening.
Our study is limited by retrospective data collection; however, data were pre-recorded in medical records before LEUS was performed and outcomes were objective. Thus, LEUS results were unlikely to have influenced risk factors or outcomes ascertainment. Furthermore, this study is observational; a randomized trial would provide superior evidence. Balancing these limitations are the novel study question and systematic assessment of DVT risk factors that resulted in no exclusion for missing data.
LEUS screening for asymptomatic DVT prior to SCD application in ICU patients with contraindications to anticoagulation was associated with a delay in SCD application, low diagnostic yield, and no proven benefit. Prospective randomized studies are needed to better evaluate this practice and test risk assessment models and clinical algorithms.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.