
Abstract

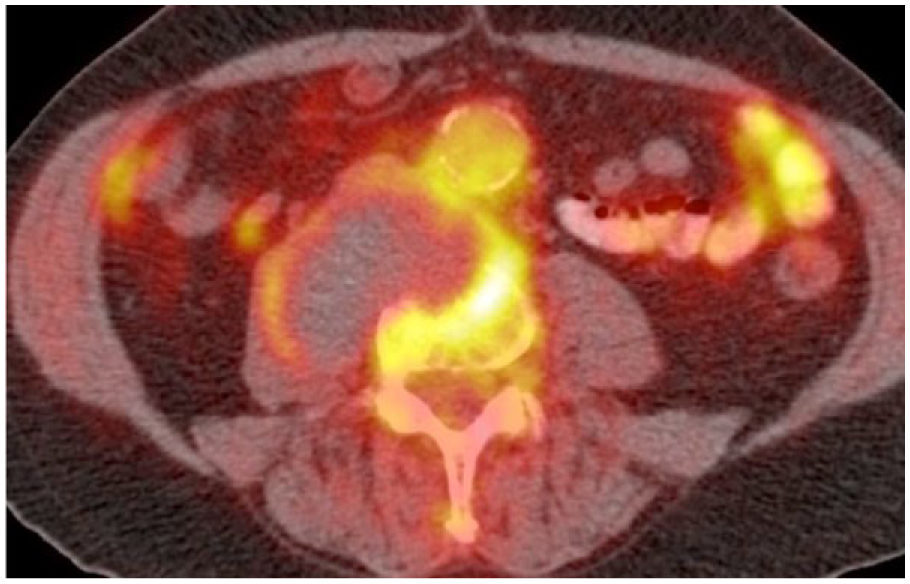
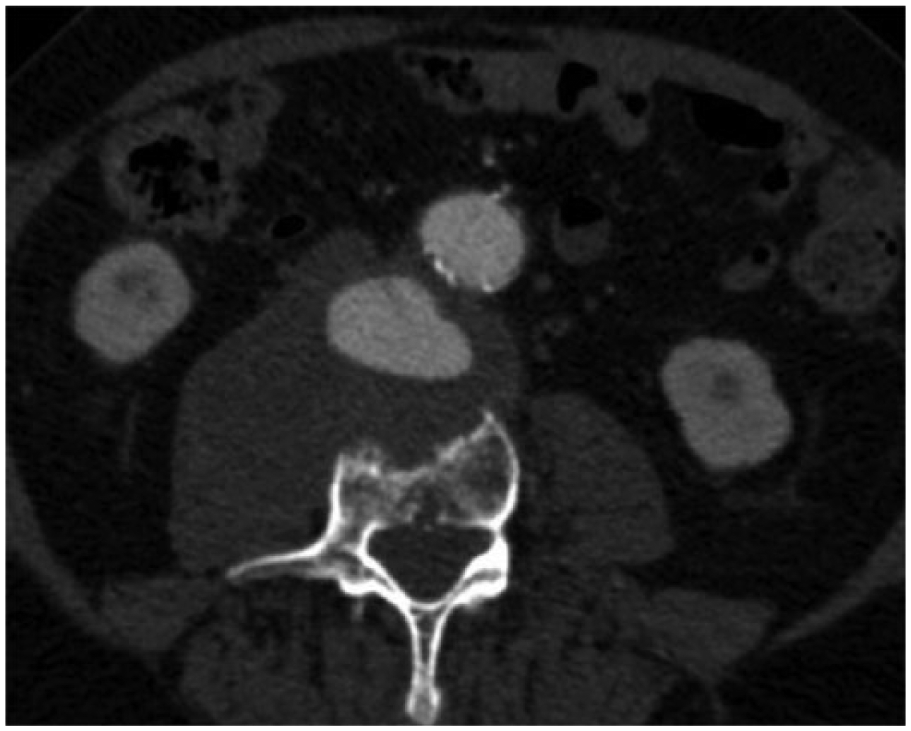
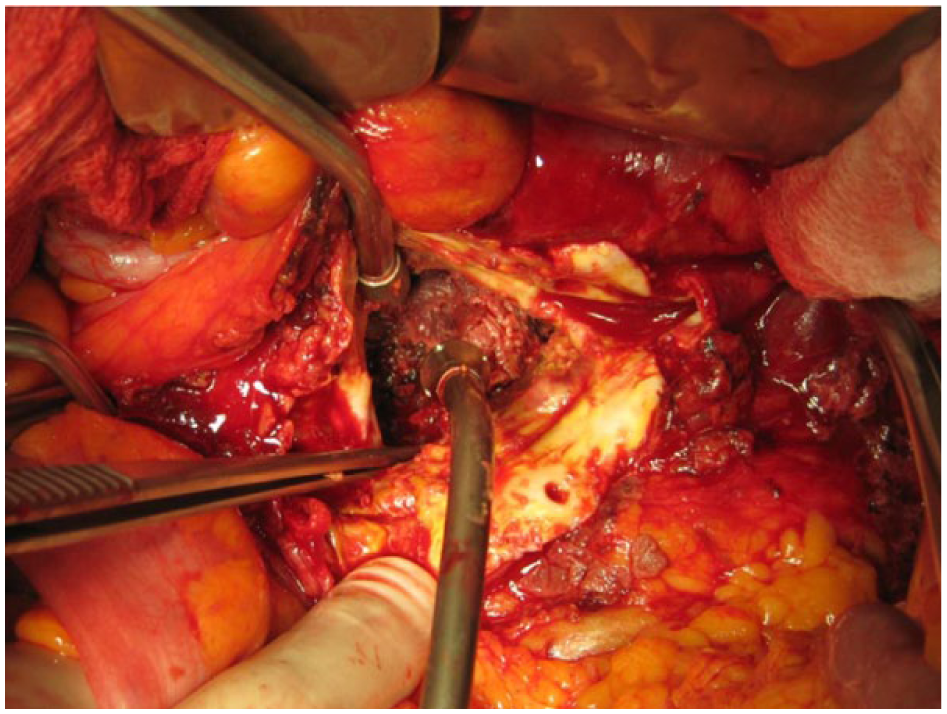
A 69-year-old male presented to the vascular surgery clinic with a 4-month history of low back pain. His previous medical history was unremarkable except for a smoking habit (100 pack-years). The patient had undergone a computed tomography (CT) scan illustrating a 4-cm diameter infrarenal abdominal aortic aneurysm (AAA) and a large soft tissue mass between the abdominal aorta and the lumbar spine, eroding the L3 and L4 vertebrae (Panel A: axial view at the level of lumbar spine 4). Magnetic resonance imaging (MRI) documented the same features and suggested a mesenchymal lesion of neurogenic origin as the most likely diagnosis. Fluorodeoxyglucose (FDG)-positron emission tomography (PET) revealed increased uptake in the peripheral rim of the mass with central sparing, indicative of malignancy with central necrosis or infection (Panel B). However, a fine-needle aspiration was negative for malignancy. The diagnosis of infection was rejected since the intervertebral disks were preserved. Subsequent computed tomography angiography (CTA) of the abdominal aorta displayed extravasation of contrast media within the ‘soft tissue mass’ (Panel C: axial view at the level of lumbar spine 4). Thus, the diagnosis of chronic contained rupture of an AAA with vertebral erosion was unequivocally made. An elective AAA open repair followed where a 3-cm diameter hole in the posterior wall of the aneurysm was found, through which the eroded vertebrae could be seen after removal of the clot (Panel D). Specimens of the retroperitoneal hematoma and the vertebral body were negative for infection or malignancy.
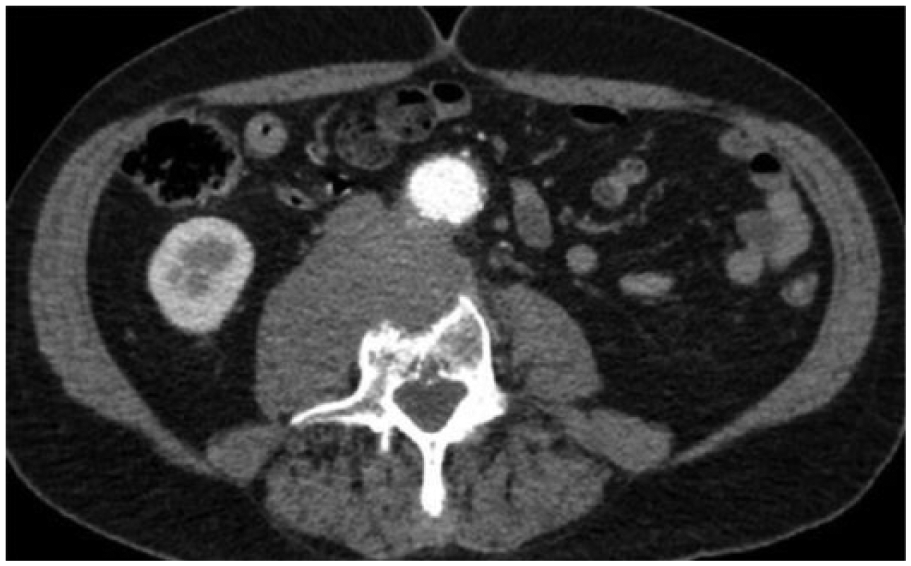
Vertebral erosion due to chronic contained rupture of an AAA is a rare clinical entity, posing significant diagnostic challenges. Differential diagnosis of a retroperitoneal soft tissue mass eroding vertebrae includes infection and tumor. 1 The diagnosis of infectious spondylodiscitis can be safely excluded when the intervertebral discs are preserved, whereas a causative tumor can be difficult and risky to diagnose if a needle biopsy is performed. 2 Characteristic features of a chronic contained aneurysm rupture causing vertebral erosion include a well-corticated, curvilinear erosion in the anterior segment of the vertebral body and the ‘draped aorta’ sign, defined as draping of the posterior aortic wall on the anterior margin of the vertebral body.2,3
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.