
Abstract

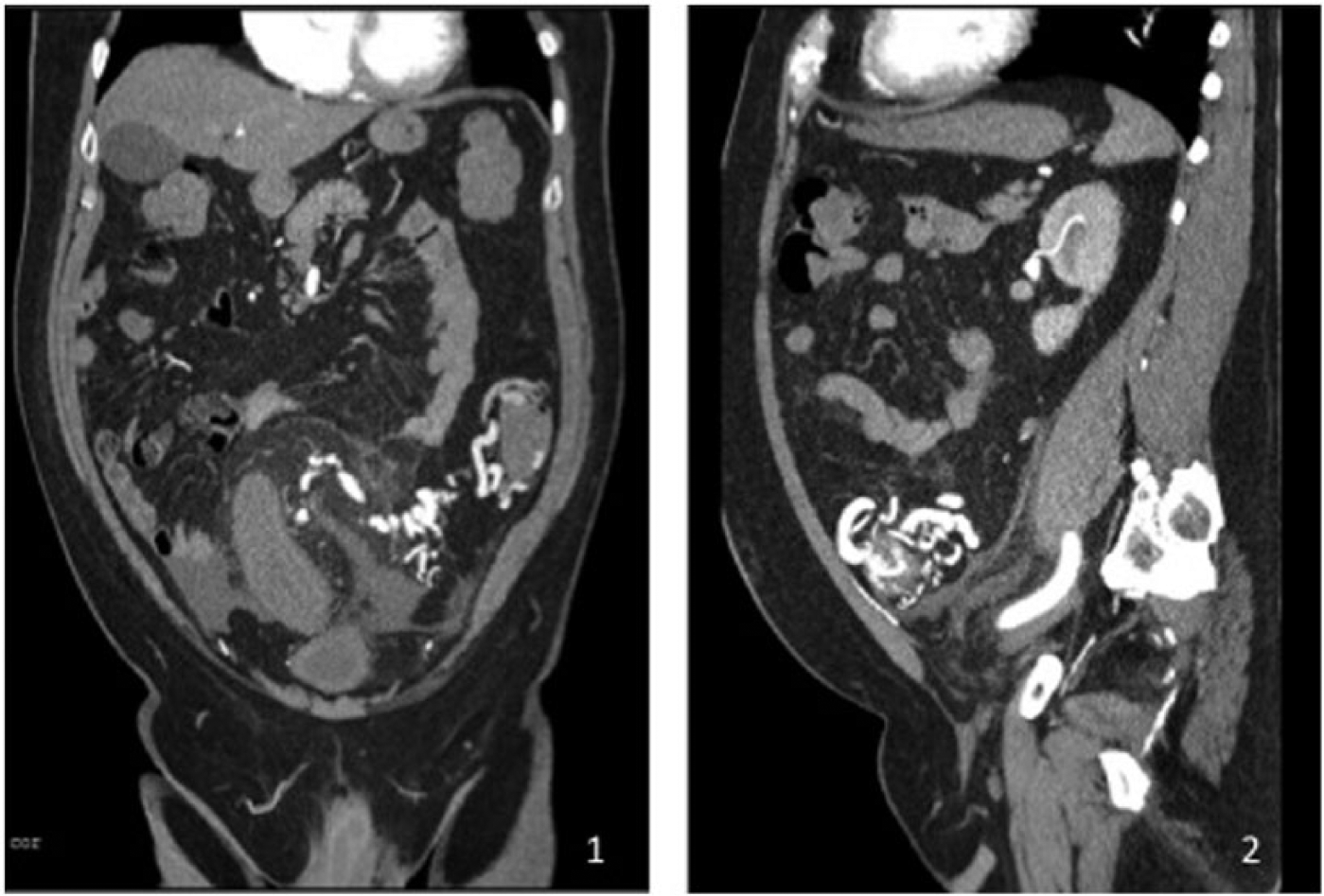
A 61-year-old man presented with a 1-month history of abdominal pain. The pain was suprapubic and associated with a decrease in bowel movements and trace blood in his stool. Suprapubic and left lower quadrant (LLQ) tenderness were noted on physical exam. Relevant labs included hemoglobin of 12.0 g/dL, white blood cell count (WBC) of 8.3 K/μL and lactic acid of 1.0 mmol/L. Colonoscopy showed segmental colitis of the descending and sigmoid colon with evidence of extrinsic inflammatory tissue. A computed tomography angiogram (CTA) revealed a tangle of vessels and an intramural enhancing focus in the sigmoid colon suggestive of an arteriovenous malformation (AVM) (Panels A1 and A2). Signs of bowel ischemia were present, including wall thickening, mesenteric fat stranding and trace free fluid, but no pneumatosis, portal venous gas or free air were identified. A magnetic resonance angiogram (MRA) revealed similar findings, but also demonstrated an enlarged inferior mesenteric artery (IMA) with early opacification of the portal venous system via the inferior mesenteric vein (IMV) (Panel B). An angiogram was performed, which confirmed a LLQ AVM with early draining veins and convoluted vessels distal to the left colic artery, with two separate groups of venous varicosities located in the sigmoid and distal descending colon (Panels C1–C4). The venous outflow was entirely through an enlarged but otherwise unremarkable IMV. Arterial recruitment was also present from the left gonadal artery and a hypertrophied lumbar artery. The lesion was deemed too extensive for endovascular therapy, and the patient proceeded to open sigmoid colectomy. Pathology of the specimen demonstrated an AVM involving the mesentery and bowel wall with prominent polypoid growths arising from the antimesenteric border of the bowel and extensive fatty hypertrophy (Panel D).



Diagnostic criteria and management options remain case-specific due to the relative infrequency of these lesions (less than 20 cases described in the English literature). 1 Evidence of the AVM can be uncovered by identifying turbulent flow on Duplex ultrasound: cross-sectional imaging can reveal the AVM itself, or can manifest as colonic thickening, mesenteric congestion, and early enhancement of the venous structures on arterial-phase studies. Furthermore, evidence of ischemic colitis can be obtained with colonoscopy, although the underlying etiology is often not evidenced endoscopically. Management options include embolization of the IMA or surgical resection of the colon. Embolization risks bowel infarction. Surgical resection, by nature of the lesion, carries a high risk of hemorrhage. Controlled, limited pre-operative embolization of the lesion has been performed to decrease intra-operative blood loss. 2
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.