
Abstract

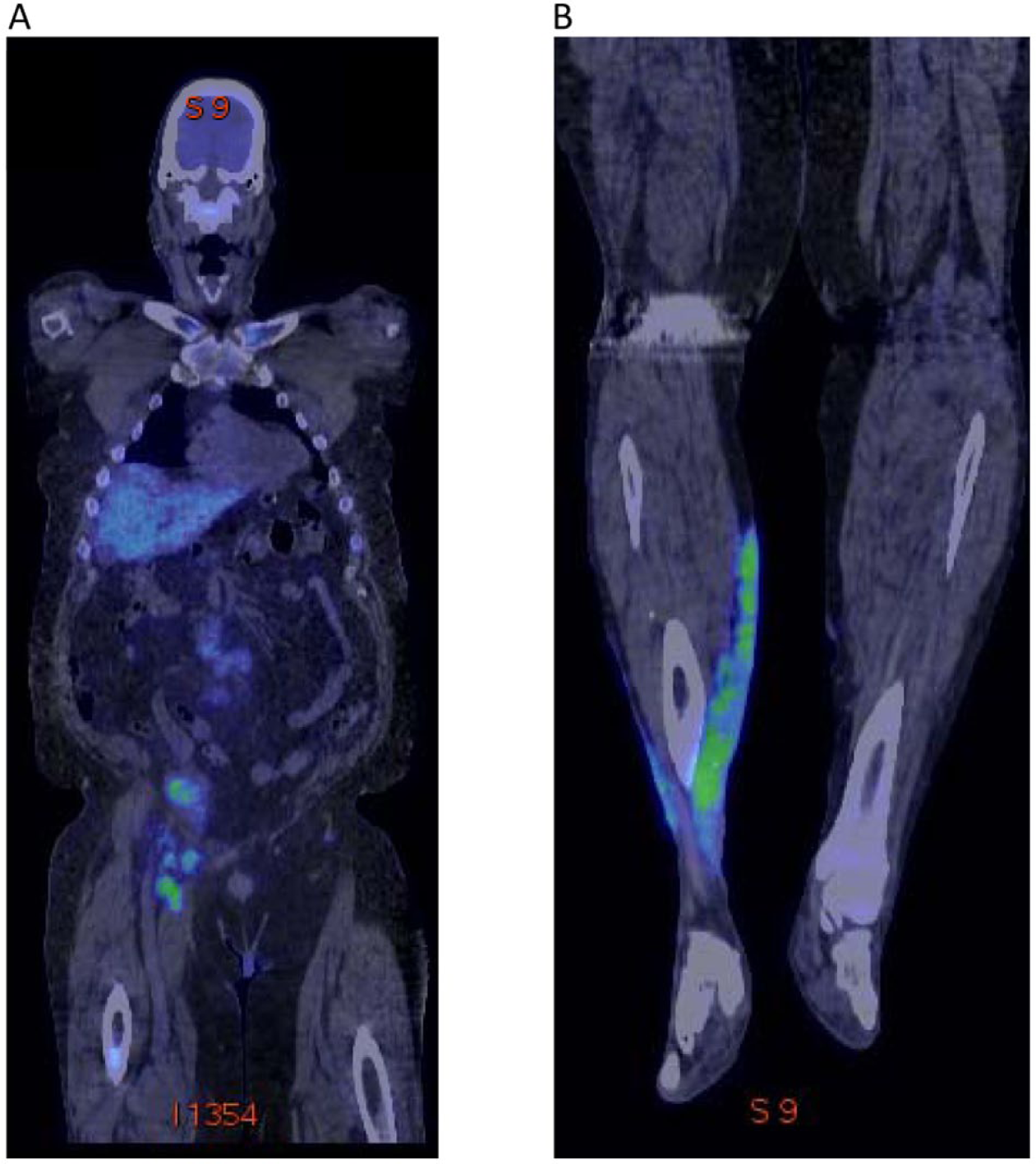
A 62-year-old male developed multiple blistering ulcerations along the medial aspect of both calves (Panel 1A and 1B) and was referred to the vascular wound clinic with the diagnosis of ‘venous stasis’ ulcerations. These lesions progressed over 6 months, beginning with a minor scratch. He had no prior history of venous disease including deep venous thrombosis. The atypical proximal extension involving the anterior foreleg of the right leg lesion (Panel 1A), the infiltrative texture, the violaceous coloration and the absence of coexisting hemosiderosis or lipodermatosclerosis (Panel 1A and 1B) suggested an alternative diagnosis. Moreover, the short segment of irregular wall thickening of the right femoral vein with two incompetent perforating veins measuring 0.3 cm and 0.4 cm noted on Duplex ultrasound was insufficient to explain the physical findings. Inguinal lymph nodes that appeared malignant were noted during the ultrasound exam. The complete blood count and differential revealed a very mild normocytic, normochromic anemia (Hgb 12.9 g/dL) but were otherwise completely normal. Abnormal ultrasound revealed apparent malignancy in the retroperitoneal and pelvic adenopathy. Positron emission tomography imaging revealed diffuse fluorodeoxyglucose (FDG) uptake involving the axial and appendicular skeleton, kidneys, spleen, liver, lymph nodes, and medial right calf dermis (Panel 2A and 2B). Lymph node, bone marrow and dermal biopsies were consistent with B-cell acute lymphocytic leukemia and leukemia cutis. Although his leg ulcers responded to aggressive leukemia treatment, the patient ultimately succumbed to this diagnosis 5 months later.

Dermal manifestations of acute leukemia can be non-specific and contain no malignant cells or may infrequently involve true leukemic cell dermal infiltrates. 1 In rare presentations, leukemic cells may invade the skin before there is clinical evidence of leukemia elsewhere, as in our patient. 2 In our case, dermal biopsy provided the diagnosis, which was confirmed with bone marrow and lymph node sampling.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.