
Abstract
What exactly is lymphedema?
Lymphedema is a condition that arises when some or all of the lymphatic vascular system does not function properly. There are many causes of lymphedema, but they all involve an inability of this circulatory system to move fluid efficiently. Because lymphedema alters the appearance and function of the affected parts of the body, it can very frequently alter the person’s sense of well-being or the ability to undertake normal activities. There is no cure for lymphedema at present but, fortunately, effective treatment options are available.
What is the lymphatic system?
The lymphatics are tiny vascular channels that are distributed throughout the body. These channels are actually part of the circulation. Each time the heart pumps blood through the circulation, approximately 1% of the fluid becomes trapped in the tissues. In order to return to the heart, this fluid must enter the lymphatics and these small vessels carry the fluid back to the heart.
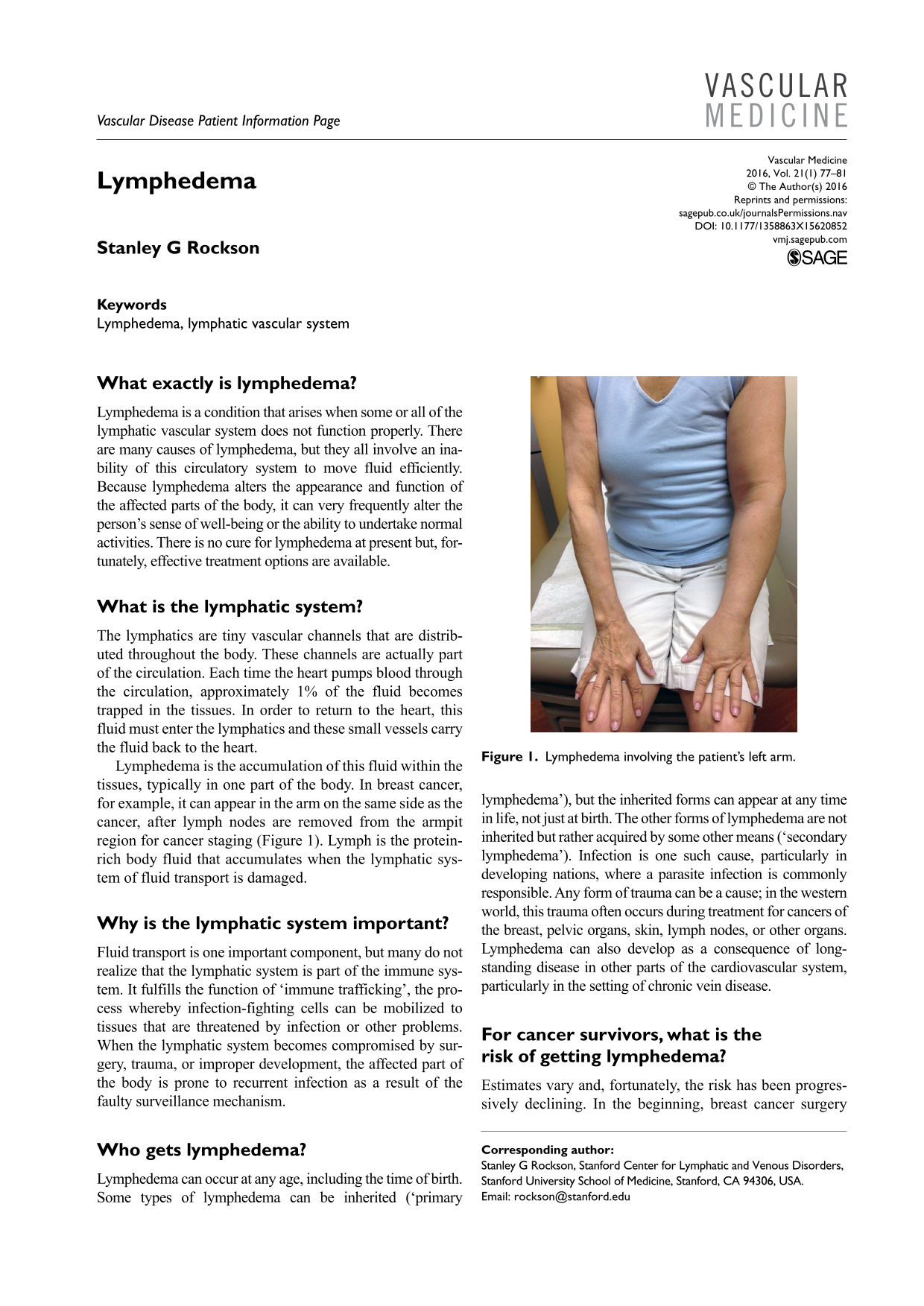
Lymphedema is the accumulation of this fluid within the tissues, typically in one part of the body. In breast cancer, for example, it can appear in the arm on the same side as the cancer, after lymph nodes are removed from the armpit region for cancer staging (Figure 1). Lymph is the protein-rich body fluid that accumulates when the lymphatic system of fluid transport is damaged.

Lymphedema involving the patient’s left arm.
Why is the lymphatic system important?
Fluid transport is one important component, but many do not realize that the lymphatic system is part of the immune system. It fulfills the function of ‘immune trafficking’, the process whereby infection-fighting cells can be mobilized to tissues that are threatened by infection or other problems. When the lymphatic system becomes compromised by surgery, trauma, or improper development, the affected part of the body is prone to recurrent infection as a result of the faulty surveillance mechanism.
Who gets lymphedema?
Lymphedema can occur at any age, including the time of birth. Some types of lymphedema can be inherited (‘primary lymphedema’), but the inherited forms can appear at any time in life, not just at birth. The other forms of lymphedema are not inherited but rather acquired by some other means (‘secondary lymphedema’). Infection is one such cause, particularly in developing nations, where a parasite infection is commonly responsible. Any form of trauma can be a cause; in the western world, this trauma often occurs during treatment for cancers of the breast, pelvic organs, skin, lymph nodes, or other organs. Lymphedema can also develop as a consequence of long-standing disease in other parts of the cardiovascular system, particularly in the setting of chronic vein disease.
For cancer survivors, what is the risk of getting lymphedema?
Estimates vary and, fortunately, the risk has been progressively declining. In the beginning, breast cancer surgery carried a 50% risk of lymphedema development. Today, patients who have axillary (armpit) lymph node dissection have a lifetime risk of 15–25%. For individuals whose surgery is limited to sentinel node techniques (removal of four or fewer lymph nodes), without radiation, the risk is about 6–10%. Pelvic cancers or other cancers that require lymph node dissection may carry a lifetime risk of 20–50%.
Does radiation increase the risk of lymphedema?
Yes. Radiation can traumatize the lymphatic system as much as surgery, even if surgery is not done. However, just as all surgery is not alike, not all radiation therapy is the same. In general, radiation therapy confers risk that is roughly equivalent to axillary lymph node dissection and increases the risk associated with surgery if both treatments are performed.
If I have had lymph nodes removed under one arm, do I have to worry about the lymph nodes in other areas of my body?
No. The lymphatic system is present throughout the body, but lymphedema is a regional disease that affects only the part of the body that is subjected to surgery or radiation.
If I experience swelling of a limb after surgery, how would I know whether or not this is indeed lymphedema?
We can never be certain without more clinical information, since there are a variety of reasons that swelling of a single arm or leg might occur after surgery. In the setting of cancer surgeries, we become concerned that the swelling might be lymphedema, since cancer surgery is a known provoking cause. In such circumstances, it is very important to seek the input of a health care professional. Physical examination and, possibly, additional tests will help to determine the cause. It is likely, but not certain, that the swelling will prove to be lymphedema.
If I suspect that I might have lymphedema, is it time-critical that I take action?
It is important to act promptly. There is evidence to suggest that the duration of lymphedema will determine its severity and its responsiveness to treatment. At the earliest sign of a potential problem, a health care professional should be consulted to initiate whichever tests and treatments may be indicated. The most time-critical aspect of lymphedema relates to the risk of infection in the tissues, which occurs in 20–25% of patients with lymphedema. This type of infection is called

Cellulitis in a patient with lymphedema. The skin is red and warm, and the leg is more swollen than usual.
Should I allow blood-drawing from my affected limb? Vaccinations? Acupuncture? Tattoos?
There are life-compromising and life-saving situations in which intravenous or surgical interventions on the limb at risk are unavoidable. Since there is a potential risk associated with intravenous punctures, the correct answer would be to never allow needle punctures in a situation where these are avoidable; on the other hand, if the health care team has a valid, unavoidable need to use the arm for your health, do not hesitate to give your consent. Vaccinations, acupuncture, tattoos and all other forms of avoidable skin trauma should also be avoided in the limb at risk.
What about taking blood pressure in the arm?
It is preferable that this be avoided, particularly in circumstances where the blood pressure is measured repetitively. There are no prospective studies to support this advice, but it is a prudent precaution when feasible.
What if both arms are at risk?
The cautious approach would be to take all blood pressure readings in the legs. One can also draw blood from the foot, although the procedure is more time-consuming and laborious. Here, again, in urgent or life-saving circumstances, it is certainly acceptable to use the arm(s) at risk.
Do I need to worry about sunburn?
Absolutely. Sunscreen should always be applied, particularly to the limbs at risk. Sunburn can definitely trigger lymphedema.
If I get a cut, a scratch from my pet, or an insect bite, should I panic?
Definitely not. There is a very low likelihood of any of these events leading to lymphedema development. For breaks in the skin, it is, nevertheless, important to cleanse well and apply a local over-the-counter disinfectant. If there is any sign of swelling (even modest) or any visible red streaks or other signs of active infection, consultation with a health care provider should occur immediately.
What about hot tubs and saunas?
Hot tubs and saunas pose no problem, provided that the temperature remains below 105°F (40.6°C).
What about massage therapy?
Gentle massage is generally okay, but shiatsu and deep pressure massage should be avoided.
How important is weight control for preventing lymphedema?
Weight control is very important. Excess weight is a known risk factor for the development of lymphedema among high-risk patients. Preventing weight gain and obesity will help to limit the risk of lymphedema.
Does exercise help?
Exercise is definitely beneficial. Contraction of the muscles during exercise stimulates lymph flow through direct action on the lymphatic and venous vessels. Regular exercise can help to prevent lymphedema in those at risk, and can minimize the impact of the problem in people with established lymphedema. Exercise should always be performed with an appropriate compression garment in place. Swimming and water aerobics are a wonderful alternative because the water itself provides compression and no additional garment is required.
Should I be measuring my limb(s) regularly at home?
No. There is no added benefit over simply taking care of the limb(s) and avoiding risky situations when feasible.
Should I get a compression sleeve even if I don’t have lymphedema?
There is no hard evidence to support the efficacy, but this is a reasonable choice to consider for airline travel, high altitudes, and strenuous physical exertion of the limb if there is a risk of developing lymphedema. Compression garments should always be worn during the day if lymphedema is already present.
How is the diagnosis of lymphedema established?
The most important element in the diagnosis is the physical examination. If there is any question about the diagnosis, imaging studies can be performed. Most often, this might entail a nuclear scan, called a lymphoscintigram (Figure 3), in which a small dose of a tracer compound is injected into the hand or foot. Images are taken of the compound’s trip through the lymphatic system to the draining lymph nodes in the armpit or groin. Slowing of transit and/or build-up of tracer in the tissues will indicate the presence of lymphedema.
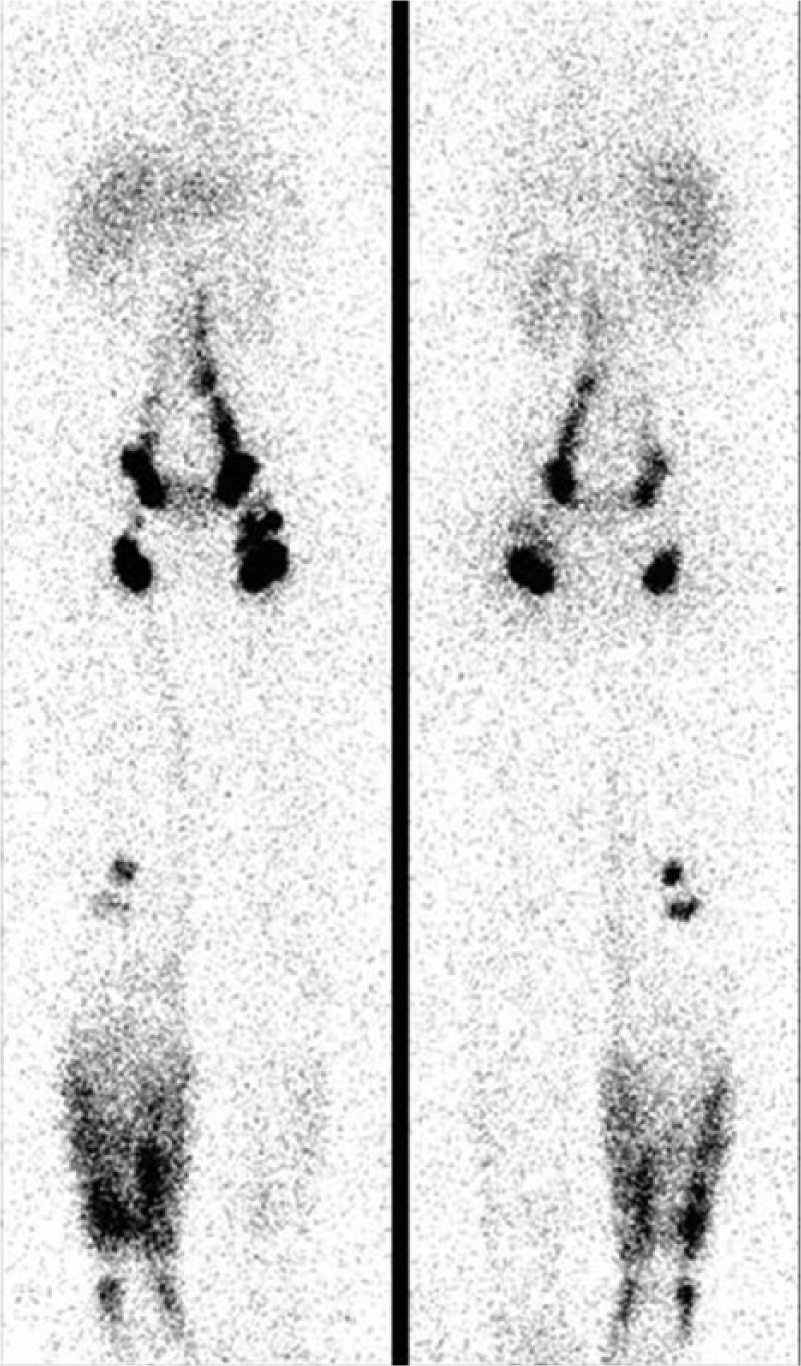
A lymphoscintigram showing signs of lymphedema in the lower right leg.
In establishing the diagnosis, it is sometimes important to document the health of other parts of the circulation, so a cardiac or venous ultrasound may also be performed.
What is the treatment for lymphedema?
Lymphedema is treated through physical means. Lymphedema causes an accumulation of fluid in the tissues. In order to mobilize that fluid, we have to stimulate the lymph system to be more active. The complete treatment approach is called
What is MLD and how does it work?
MLD is an acronym that stands for manual lymphatic drainage. The technique was discovered about 75 years ago. MLD stimulates the contraction of the lymphatic channels. MLD uses directed, light touch to produce the desired stimulation to the skin. The massage opens the lymphatic capillaries and encourages them to permit the entry and transport of fluid. MLD cannot be done intuitively: lymphedema therapists undertake intensive training to learn how to do MLD correctly. Patients can be taught a self-administered form of simple MLD, but it is vital that the patient is guided through direct instruction given by the therapist.
Is lymphedema treated by a physician or therapist?
The therapist treats the patient, ideally under the direction of the physician who orders the treatment. Typically, each session of therapy will include 15–30 minutes of MLD. Following MLD, a multi-layer bandage will be applied; this procedure typically requires 30–45 minutes. Ideally, the patient will wear the bandaging material for several hours following treatment and, if possible, overnight. This same treatment sequence will be repeated over 15–30 additional sessions, depending upon the severity of the lymphedema and depending upon its responsiveness to treatment. With each application of the bandages, there will be an incremental reduction in the volume or size of the limb. When volume reduction is maximal, the therapist will measure the limb for a compression garment. This stocking or sleeve will be supplied to the patient to be worn on a daily basis.
How do I find a therapist?
Finding a therapist can be a little bit of a challenge because, in the United States, there are insufficient numbers of well-trained lymphedema therapists. In addition, the geographical distribution of therapists is quite uneven: some areas have many and some areas have only a few or none at all. Therapists come from a variety of training backgrounds: physical or occupational therapists, nurses, or even massage therapists who have completed additional training. In this search, the most important element is to be certain that the therapist has had sufficient, specific training in lymphedema treatment techniques. MLD is not an athletic massage; it must be done correctly and under appropriate supervision. It is best to look for a therapist who works closely with referring physicians, to facilitate the dialogue about your care between your doctor and the therapist. If possible, get some feedback from other patients who have been treated by this therapist.
What about intermittent pneumatic compression devices?
Intermittent pneumatic compression devices can be very useful and effective in lymphedema, but they should not be used as stand-alone treatment, since the pump cannot supplant the other manual therapies. All devices are not identical. Because these devices are used for a variety of medical problems, it is important that the pump mechanism is appropriate for lymphedema care.
Once you have completed CDPT and have been fitted with a garment, you may find that you are not completely satisfied with the response to treatment. In some cases, adding in device therapy to garment use, exercise, and self-administered MLD will lead to further improvement.
Are there any effective drug therapies for lymphedema?
At the moment there are few, if any, effective drug treatments. While there are no available prescription drugs for lymphedema, active research is underway to identify effective drug therapies for lymphedema.
Is surgery an option?
There are surgical options for selected patients. Historically, many surgical approaches have failed to be effective in lymphedema, such that these previously recommended interventions are no longer used. One successful surgical intervention, for certain situations, is suction-assisted lipectomy: in some cases of established lymphedema, the fluid accumulation in the limb is gradually replaced by equivalent volumes of fat-storage cells. Because body fat is fluid at room temperature, the excess limb volume has many of the attributes of edema fluid, but, unlike tissue fluid, it cannot be displaced. For this reason, typical treatment techniques (MLD, compression garments, and pumps) no longer encourage the limb to reduce in size. The excess fat storage tissue can be removed surgically, through a very safe technique under general anesthesia. However, the caveat is, if you are to be considered for this surgery, you must be willing to maintain 24 hour/day garment use after the surgery is completed. Surgery will reduce the lymphedematous limb to normal size, but, without postoperative compression, the limb will quickly become edematous again.
Other surgical approaches include autologous vascularized lymph node transfer and lymphaticovenous anastomosis; experience with these techniques is still quite limited.
Summary
The lymphatic system is a part of the circulation that is responsible for the transportation of tissue fluid back to the heart. This system can be damaged by many conditions, including developmental disorders, surgery, trauma, or chronic diseases of the heart or of the veins, among many other potential causes. When the lymphatics are damaged, swelling in one or more limbs can occur. This is called lymphedema. Lymphedema is chronic and has no cure, but can be treated effectively. Treatment generally includes a focused form of physical therapy called complex decongestive physiotherapy. Long-term care requires the use of compression garments to prevent re-accumulation of tissue fluid. Soft-tissue infection, called cellulitis, is a common, and potentially recurrent, complication of lymphedema. Prompt treatment of cellulitis is important. Prevention of progression of lymphedema includes proper skin care, avoidance of additional trauma, and regular exercise with the compression garment in place.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.