
Abstract

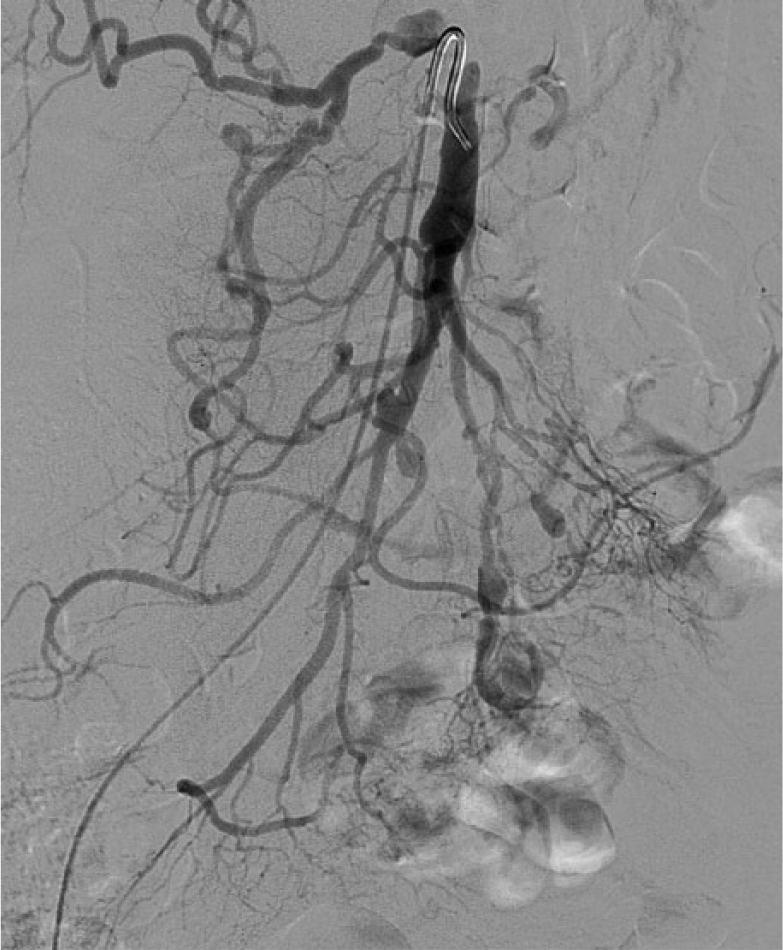
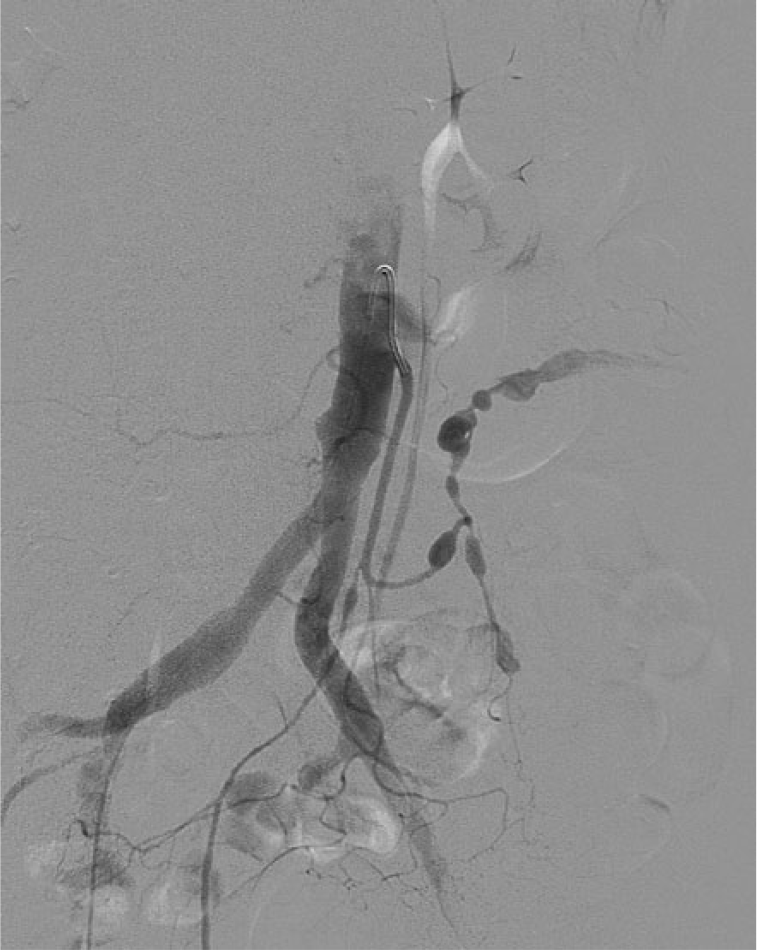
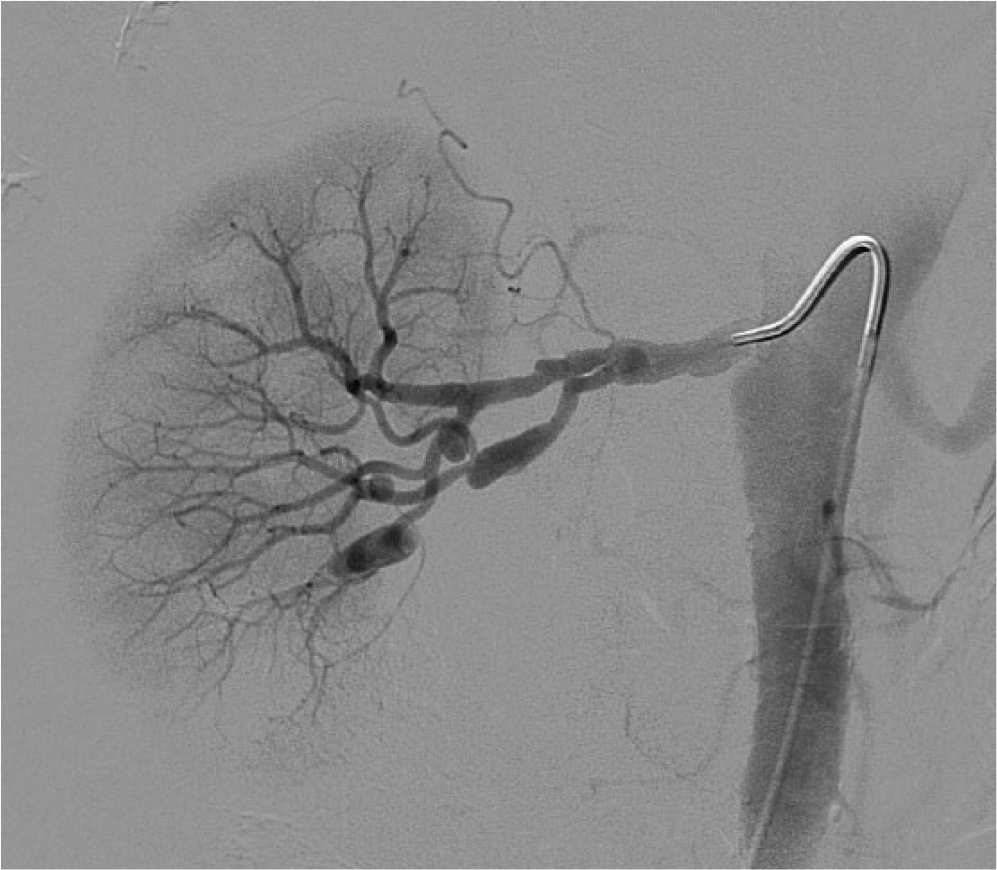
A 61-year-old woman presented to our hospital complaining of months of episodic postprandial abdominal pain with weight loss, malnutrition, and multiple outside hospital admissions. She also had a history of basilar artery aneurysm and hypertension. Comprehensive laboratory testing excluded autoimmune, inflammatory, or infectious etiologies. Computed tomographic angiography (CTA) of the abdomen revealed multiple aneurysms and stenoses of the superior and inferior mesenteric arteries (SMA and IMA, respectively). Invasive angiography confirmed that the SMA (Panel A) had diffuse stenoses and multiple aneurysms of its branch vessels. Similarly, the IMA (Panel B) had large aneurysms and slow flow. Renal artery angiography (right renal artery in Panel C) showed aneurysms alternating with stenoses. Our working diagnosis was mesenteric ischemia caused by multifocal fibromuscular dysplasia (FMD) of the visceral arteries. 1 However, segmental arterial mediolysis and quiescent polyarteritis nodosa could not be definitively excluded by imaging alone. Therefore, laparoscopic biopsy of the left colic artery was performed.
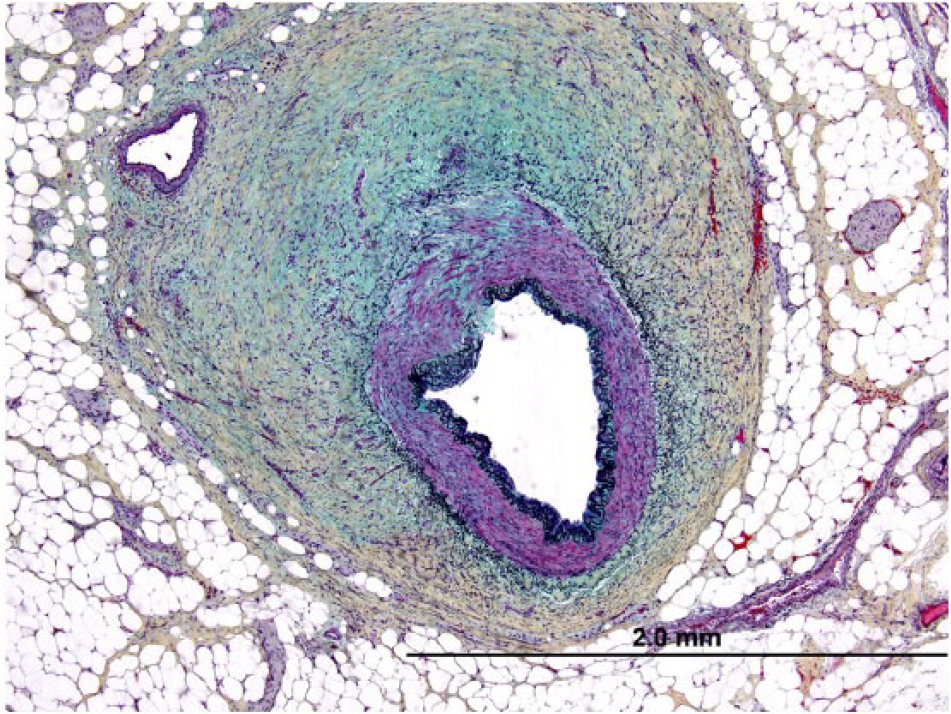
Histopathologic examination of the biopsied artery revealed multiple tears and dissections of the medial layer and aneurysmal formation without inflammation or atherosclerosis (Panel D shows a representative section with an intimal tear at 11 o’clock). Secondary fibrointimal thickening was observed and the medial layer was mostly absent. An overlying organized thrombus was seen in one section as a result of a medial tear and dissection. There was no evidence of vasculitis. Taken together, the pathologic diagnosis was of medial FMD, consistent with the patient’s angiographic findings.
Percutaneous revascularization was not feasible because of the extent of her disease. Given the morbidity and risk of mesenteric bypass surgery, particularly in a weakened patient, 2 we pursued anticoagulation and supportive care. Over a 6-month follow-up, the patient has gained weight and avoided hospitalization.
FMD is a non-inflammatory, non-atherosclerotic vascular disease that can result in occlusion or aneurysm of affected vessels. Most frequently involved are the renal, carotid, and vertebral arteries. 1 In the FMD registry, evidence of mesenteric FMD was seen in 26.3% of patients who had abdominal vascular imaging. But, only 1.8% of patients had a history of mesenteric ischemia at the time of enrollment. 3 While symptomatic visceral FMD is rare, early catheter angiography may expedite diagnosis in patients with otherwise unexplained symptoms of mesenteric ischemia. Biopsy may be warranted in cases with diagnostic uncertainty.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.