
Abstract
Up to half of patients with signs and symptoms of stable ischemic heart disease have non-obstructive coronary artery disease (NoCAD). Recent evidence demonstrates that two-thirds of patients with NoCAD have demonstrable coronary endothelial dysfunction represented by microvascular or diffuse epicardial spasm following acetylcholine challenge. Patients with coronary endothelial dysfunction are recognized to have significant health services use and morbidity as well as increased risk of developing flow-limiting coronary artery disease and myocardial events, including death. Currently, there are few centers that test for this etiology owing to lack of knowledge, limited evidence for treatment options and invasive diagnostic strategies. This article reviews the pathophysiology, epidemiology, diagnosis and treatment of coronary endothelial dysfunction as a subgroup of NoCAD.
Keywords
Introduction
The importance of chest pain syndromes in the setting of non-obstructive coronary artery disease (NoCAD) is increasingly being recognized, as the burden of this condition is significant in terms of cost and morbidity.1–4 Furthermore, while classically NoCAD had not been thought to be associated with increased risk of mortality or cardiovascular events,5,6 more recent evidence suggests that certain subpopulations with NoCAD are at heightened risk.7–14 In particular, patients with endothelial dysfunction make up roughly two-thirds of the patients with NoCAD and display increased risk of aggregate cardiovascular events.11–14 Despite the serious nature of this entity, patients with NoCAD are often reassured without due consideration to diagnostic or treatment options. 15 This paper explores the definition, pathogenesis, diagnosis and treatment of endothelial dysfunction as a subset of NoCAD.
Definitions and epidemiology
Non-obstructive coronary artery disease (NoCAD), cardiac syndrome X (CSX), conduit vessel endothelial dysfunction and microvascular angina are all terms used to describe patients that have chest pain yet no obstructive coronary artery disease on coronary angiography. The nomenclature for chest pain syndromes is often confusing, with differing terms occasionally used to describe the same population and the same terms occasionally used to describe heterogeneous populations. The terminology is most easily understood in the containment model proposed in Figure 1.
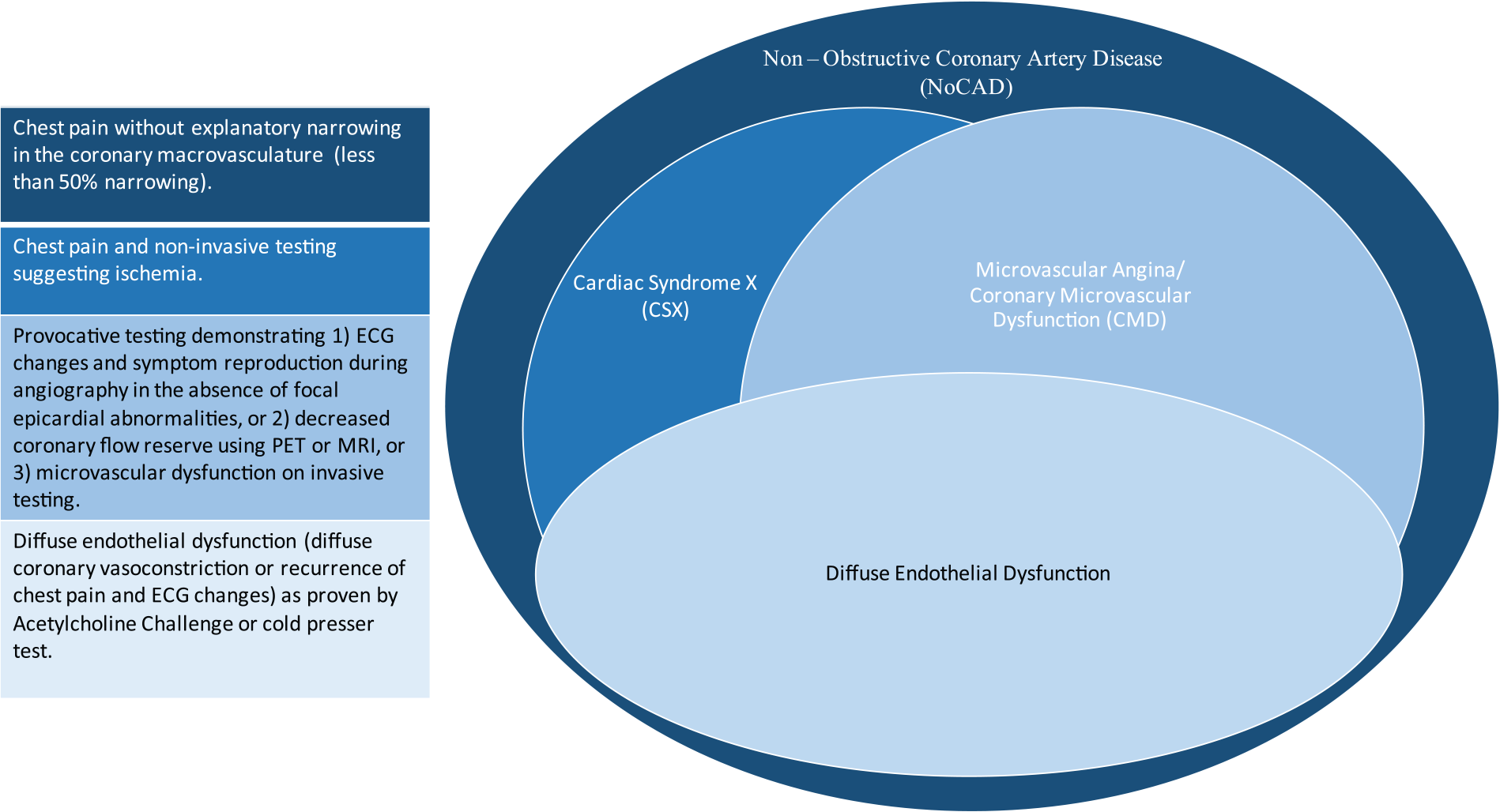
Defining the terminology of chest pain syndromes. (ECG, electrocardiogram; MRI, magnetic resonance imaging; PET, positron emission tomography.).
NoCAD
NoCAD, sometimes called chest pain with minimal coronary artery disease, is an all-inclusive term for chest pain syndromes without hemodynamically significant obstructive coronary artery disease and includes patients with non-cardiac chest pain. NoCAD is defined as either less than 50% narrowing, less than 20% narrowing or unimpaired coronary blood flow, depending on the study.
Large retrospective studies of patients referred for non-urgent angiography demonstrated a prevalence of NoCAD of between 40% and 60% of all referrals,16–18 with women being more likely than men to have this presentation. 19
A recent prospective study of the same patient population found a prevalence of 47%. 20 Other studies report lower prevalence rates but are not confined to non-urgent angiography, include myocardial infarction (MI) or exclude patients with insignificant but identifiable coronary artery disease.21–27
Etiology
There are several potential explanations for NoCAD that can be divided into ischemia and non-ischemia categories. Non-ischemic explanations include non-cardiac chest pain and increased proprioceptor sensitivity. 28 Distinguishing ischemic from non-ischemic chest pain can be challenging as high rates of false positive diagnoses are differentially associated with ECG, stress test or perfusion study. Invasive testing, although controversial, due to the relative benefit or risk of the procedure, remains the best way to distinguish between etiologies of NoCAD (Figure 2). Ischemic explanations of NoCAD include: (1) microvascular dysfunction caused by impairment of smooth muscle relaxation; (2) microvascular dysfunction caused by abnormal vasomotion response in the coronary microcirculation; (3) coronary slow flow phenomenon; (4) diffuse epicardial vasomotion abnormalities; (5) focal/proximal epicardial constriction (Prinzmetal’s angina); and (6) spontaneous coronary artery dissection. Taken together, explanations 1–4 encompass CSX, explanations 1 and 2 refer to microvascular angina 29 and explanations 2 and 4 together encompass distal endothelial dysfunction. 20 Coronary slow flow, coronary artery dissection and focal/proximal epicardial spasm have distinct and unrelated pathological explanations and are outside of the scope of this review.
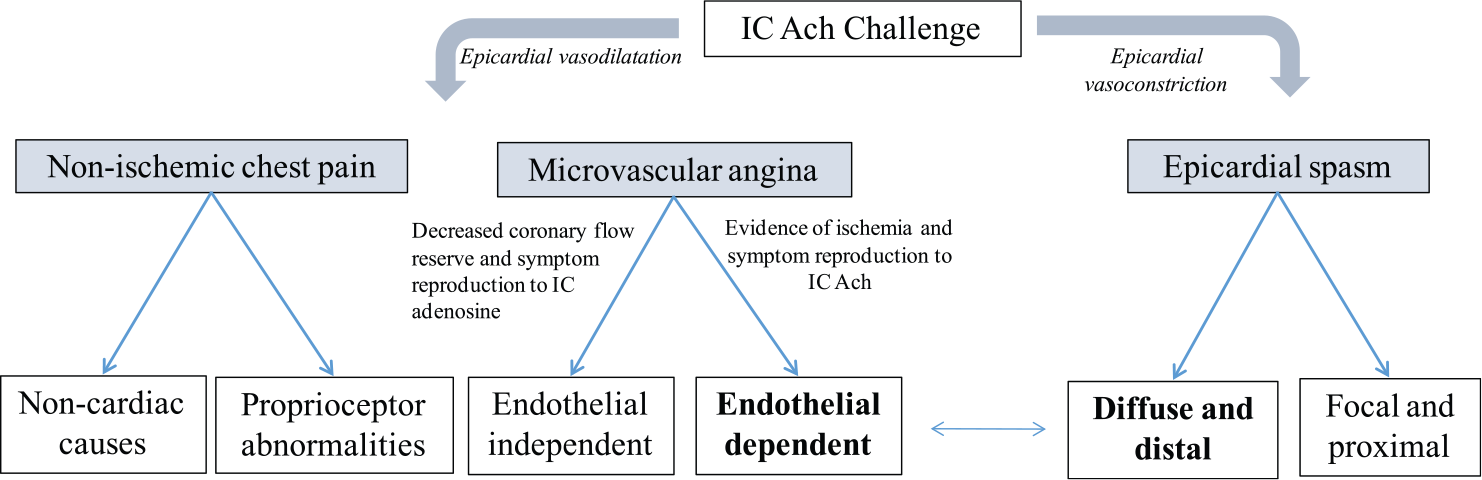
Proposed diagnostic algorithm for invasive testing in NoCAD (endothelial dysfunction in
Cardiac syndrome X
CSX, a term originally coined by Kemp in 1973, 29 differs from chest pain with NoCAD in the requirement for proof of ischemic changes on non-invasive testing. CSX is a further narrower term than NoCAD as it excludes those patients with ST elevation and/or MI, thus theoretically excluding those patients with occlusive focal vasospastic abnormalities of the proximal to mid-coronary macrovasculature. This distinction is seldom relevant as the vast majority of patients with acute coronary syndrome and non-obstructive coronary arteries present without troponin or ST elevation. 1 Furthermore, while a significant portion of these patients have epicardial vasomotion abnormalities, they are very rarely occlusive. The prevalence of CSX in patients with chest pain and minimal coronary artery disease is difficult to determine as up to 30% of stable angina patients referred for invasive coronary angiography have not undergone non-invasive testing for risk stratification. 16 Owing to the uncertainty of the definition of CSX and the difficulty in distinguishing a pathologically distinct group from NoCAD, the broader terms will be used in its place hereafter.
Microvascular angina
Microvascular angina (sometimes called coronary microvascular dysfunction) is a narrower term than CSX as it refers to patients with positive provocative testing during angiography or a myocardial perfusion reserve defect detected on positron emission tomography (PET) or cardiovascular magnetic resonance (CMR). Evidence for ischemia in microvascular angina is demonstrated by reproducible angina and ECG changes in the absence of conduit vessel vasoconstriction. More definitive objective evidence of ischemia, including coronary sinus lactate elevation, cardiac wall motion abnormalities and perfusion defects are found in a minority of these patients. 30 The lack of consistent confirmatory evidence of ischemia is proposed to be resultant of the patchy and distributed nature of microvascular disease processes. Alternatively, differences between subgroups might help explain inconsistent results as ischemic changes are more readily identified if testing is restricted to those patients with endothelial dysfunction. 31
Microvascular dysfunction related to impaired smooth muscle relaxation is an endothelium-independent mechanism for cardiac ischemia. 32 Structural abnormalities such as micro-vessel hypertrophy, embolization or surrounding myocardial irregularities could account for this phenomenon but studies are limited and present heterogeneous results. 30 The microcirculation accounts for 70% of resistance within the coronary circulation 33 and thus ineffective smooth muscle relaxation prevents demand-related increases in flow. 34 Accordingly, these patients are theorized to present with exercise- or stress-related angina. 35 Endothelial-independent microvascular dysfunction is studied by measuring coronary flow reserve using transthoracic Doppler echocardiography, 36 myocardial contrast echocardiography, 37 PET, 38 intracoronary Doppler 39 or CMR 40 following induced vasodilation with an endothelium-independent agent such as adenosine or dipyridamole.
Coronary endothelial dysfunction
Endothelial-dependent dysfunction is caused by pathologic constriction of a vessel or vascular bed. Diffuse distal epicardial and microvascular constriction causes ST depression and can present as either rest or stress angina. 41 Furthermore, diffuse epicardial constriction is likely resultant from the same process as microvascular endothelial dysfunction and bears the same risk. 11 It is difficult to differentiate epicardial endothelial dysfunction from microvascular angina clinically without the use of coronary vasomotion studies. Even with acetylcholine challenge, chest pain or ECG, changes usually precede diffuse epicardial constriction, indicating that microvascular constriction may be the instigating event that propagates proximally. 42 Endothelial dysfunction is a significant contributor of chest pain with NoCAD and will be the subject of the review hereafter.
While it is difficult to determine the relative contribution of vasoconstrictive abnormalities to cases of NoCAD, owing to a proportion of patients with evidence of both endothelial-dependent and independent microvascular dysfunction, 43 it is extremely common within the condition. A prospective study found that in two-thirds of patient presenting with stable angina with no evidence of obstructive epicardial coronary disease, induction of endothelium-dependent constriction of the epicardial or microcirculatory vessels reproduces patient symptoms and evidence of ischemia on ECG. 20
In patients with NoCAD, it is the subset of patients with endothelial dysfunction that have a worsened prognosis. In a prospective study of patients with and without any evidence of obstructive coronary artery disease on coronary angiogram, both epicardial and microvascular endothelial dysfunction were found to be independent predictors of acute cardiovascular events. 11 Events included stroke, MIs and cardiovascular death measured at an average follow up of 40 months. In the same study, endothelial-independent microvascular dysfunction was not an independent risk of cardiovascular events, even when recurrent percutaneous coronary intervention (PCI) was included in the aggregate measure. This study is consistent with other reports showing an association between coronary endothelial dysfunction with atherosclerotic progression12–14 and cardiovascular events. 13 In contrast, a study of endothelial-dependent and independent epicardial dysfunction found both to be predictive of aggregate cardiovascular events. 44
Pathogenesis
The vascular endothelium regulates local vascular tone by causing smooth muscle relaxation and vasodilation through release of nitric oxide (NO), prostacyclin (PGI2) and endothelium-derived hyperpolarizing factor (EDHF) or by causing vasoconstriction through release of thromboxane A2, endothelin-1 or free radicals. 45 Abnormalities of the counter-regulatory balance between these factors in favor of microvascular constriction may be responsible for endovascular dysfunction. Of these factors, NO is the most studied as it is the predominant mediator of vascular tone in conduit vessels.
Decreased levels of NO bioactivity are observed in patients with CSX
46
and infusion of
Endothelin-1 has been demonstrated to be elevated at baseline in CSX57–59 and under stress. 60 Rho kinase, a downstream effector of endothelin-1, contributes significantly to the constriction of vascular smooth muscle cells and is a mediator of the vasospastic response in those patients with endothelial dysfunction and microvascular angina. 61
Alternative mechanisms other than the NO pathway have also been invoked in coronary endothelial dysfunction. Investigations have demonstrated increased inflammation in association with endothelial dysfunction in CSX. 62 Voltage-gated potassium channels are responsible for basal coronary microvascular tone and respond to endothelial factors including EDHFs. 63 ATP-dependent potassium channels likewise modulate vascular tone in response to endothelial agents yet their role in the coronary arteries is unclear.
Additionally, other studies have connected estrogen deficiency to endothelial dysfunction, which may help explain the disproportionate quantity of peri-menopausal women amongst those with CSX. 64 Endothelial dysfunction is known to occur in healthy women during menopause 65 and in the short term estrogen replacement therapy normalizes the vasospastic response to acetylcholine in post-menopausal women with coronary endothelial dysfunction. 66
Diagnosis
Invasive testing
Some cardiovascular guidelines recommend provocative testing of the coronary endothelium in those patients undergoing angiography for suspicion of coronary artery disease when no explanatory obstructive coronary artery disease is present.67–69 However, few centers are conducting provocative testing on a regular basis despite the low-risk profile when a stringent protocol is followed. 70
Intracoronary acetylcholine injection is a sensitive and specific test for variant/Prinzmetal angina 71 and is also used to diagnose endothelial dysfunction19,72–74 (see Figure 2 for invasive diagnostic pathway). Acetylcholine binds vascular muscarinic acetylcholine receptors leading to endothelial NO release and subsequent arterial dilatation when endothelial function is intact. Alternatively, when there is damage or dysfunction of the endothelium, acetylcholine induces conduit vessel arterial constriction due to direct smooth muscle cell constriction. Ergonovine is another provocative agent that induces endothelial-dependent vascular smooth muscle constriction and has been used to diagnose Prinzmetal angina. 70 However, its role in testing for microvascular angina in CSX is unclear and not recommended.
Direct observation of the microcirculation is not possible and thus endothelial-dependent microvascular angina is diagnosed as reproduction of symptoms and ST-segment depression on ECG during acetylcholine infusion without significant epicardial vasoconstriction. 42 This method has been validated by observation of concordant elevated coronary sinus lactate levels during provocative testing. 73 In patients with either chest pain or ST depression, but not both, the test is inconclusive and retesting or a trial of treatment has been proposed. 34 Alternatively, it is possible to measure coronary flow response during acetylcholine infusion using intracoronary Doppler flow wire recording. 75 A less than 50% increase in flow is considered abnormal and indicative of small vessel endothelial dysfunction.
Interestingly, in many patients with CSX, epicardial artery spasm is also present but follows a different phenotype than in variant angina 74 and is more difficult to treat. 70 Instead of focal epicardial spasm, diffuse distal epicardial spasm can be seen following acetylcholine challenge and often follows the induction of pain and ST depression, suggesting a progression of spasm from the microcirculation to the visualized arteries.
Non-invasive testing
Only a subset of patients with NoCAD have indication to undergo repeat angiography, 76 rendering invasive provocative testing less desirable. Therefore, the development of non-invasive measurements of coronary endothelial dysfunction is critical to accurately diagnose this problem in patients with NoCAD.
The cold pressor test (CPT) uses a natural sympathetic response to emersion of the feet or hands in ice-cold water, and the subsequent downstream release of NO in the coronary circulation to test coronary endothelial dysfunction. 77 The technique has been validated using intracoronary Doppler flow wire recordings in patients with coronary artery disease 77 but has not been adequately compared to intracoronary acetylcholine challenge in patients with NoCAD. Abnormal coronary CPT response does help prognosticate cardiovascular events in patients with hypertension 78 or diabetes. 79 CPT has been studied with various modalities including transthoracic Doppler echocardiography, contrast echocardiography, PET and CMR. 80
Peripheral measures of peripheral conduit artery function are validated non-invasive tools that differentially correspond to their cardiac counterparts. Flow-mediated dilatation (FMD) of the brachial artery is correlated to epicardial endothelial dysfunction in coronary arteries.81,82 However, it is a poor rule in test for epicardial endothelial dysfunction 81 and does not predict risk of future cardiovascular events83,84 in primary prevention. In patients identified as having NoCAD, impaired FMD is an independent predictor of the condition. 85
The relationship between coronary endothelial dysfunction Coronary endothelial dysfunction and peripheral microvascular dysfunction has been studied using reactive hyperemia peripheral arterial tonometry (RH-PAT). 86 In patients with NoCAD, RH-PAT has reasonable ability to predict CED or endothelial-independent microvascular angina (+likelihood ratio of 4.05). The prognostic value of peripheral measurements in NoCAD patients is currently unknown.
Treatment
Limited studies have been conducted on therapeutic options for the subgroup of NoCAD patients with proven endothelial-dependent microvascular or macrovascular dysfunction. We conducted a review of the literature with the inclusion criteria as follows: (1) endothelial dysfunction as identified by CPT with measurement of coronary flow reserve or acetylcholine/ergonovine coronary challenge as measured by symptom reproduction or Doppler flow wire recording; (2) the population had to have demonstrated chest pain with NoCAD; and (3) the treatment trial had to last 1 month or longer. The results are summarized in Table 1.87–92 Of note, only one small randomized control trial (RTC) was discovered and all trials were conducted on less than 60 subjects. Thus, no concrete evidence for treatment has yet to be established for this group. Many other small studies have looked at treatment for NoCAD or CSX without assessing the underlying etiology. The following is a noted sample with symptom control as the endpoint for therapy.
Summary of studies of treatment for patients for endothelial dysfunction and NoCAD.
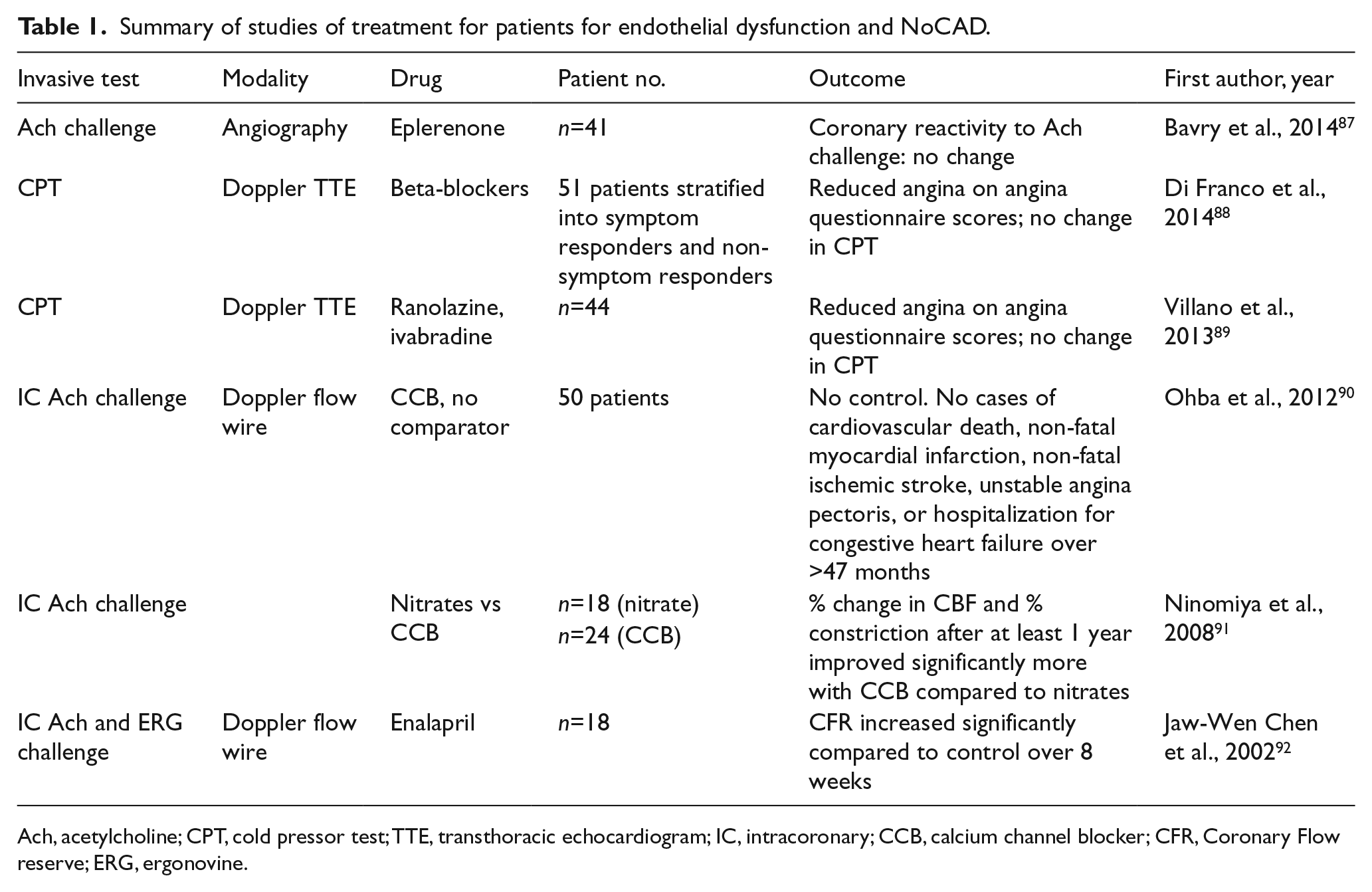
Ach, acetylcholine; CPT, cold pressor test; TTE, transthoracic echocardiogram; IC, intracoronary; CCB, calcium channel blocker; CFR, Coronary Flow reserve; ERG, ergonovine.
Drug comparators
A longitudinal study using phased therapeutic trials of CCBs, beta-blockers and nitrates demonstrated limited and transient treatment effects. 93 In a small comparative study of amlodipine, atenolol and isosorbide mononitrate only atenolol improved angina symptoms. 94 A comparative study of propranolol and verapamil demonstrated a reduction in ischemic events in the propranolol group as measured by a Holter monitor. 95 In a small phased treatment trial both nisoldipine and ramipril demonstrated a reduction in symptoms and nitrate use as well as increased exercise duration on stress test. 96
Calcium channel blockers (CCBs)
Nifedipine, as compared to a control, decreased stress-induced ST-segment depression and increased exercise tolerance. 97 Similarly, verapamil demonstrated a modest improvement in exercise duration on stress test but did not affect ST-segment depression 98 and did not reduce ischemic events on a Holter monitor. 95
Nitrates
Sublingual nitrates worsened or did not impact exercise duration and time to ST-segment depression during exercise testing with no anti-anginal effect.99,100 Despite this, clinical experience would suggest that nitrates decrease symptoms in up to 50% of subjects at least transiently.
Beta-blockers
Atenolol, as compared to control patients with CSX, caused reductions in angina symptoms and time to ST depression on exercise stress test.101,102
ACE inhibitors
ACE inhibitors are well established to have a beneficial effect in patients with CSX and proven endothelial-independent microvascular angina.103,104 However, the evidence for use in NoCAD and endothelial dysfunction is limited to the small study reviewed above. 92
Statins
In two randomized controlled trials, patients with CSX and endothelial dysfunction demonstrated by impaired brachial artery FMD were assigned to pravastatin/simvastatin or control therapy.105,106 In both trials the statin group demonstrated both an improvement in FMD and an increase in exercise capacity and time to ischemia on stress test compared to control.
Estrogen
Estrogen deficiency is associated with endothelial dysfunction and estrogen treatment diminishes acetylcholine-induced coronary reactivity. 66 Mixed results have been shown in the treatment of CSX patients. While several small controlled prospective studies of transdermal estrogen therapies demonstrate a reduction of chest pain episodes 107 and time to ischemia on stress testing, 108 there is also evidence that symptomatic benefits are attenuated in longer duration treatments. 109 Given the current controversy over HRT in cardiovascular disease disease prevention, this therapy is not currently recommended. 110
Nicorandil
Nicorandil is thought to act as an anti-anginal, spasmolytic therapy by blocking ATP-dependent K+ channels and down-regulating cGMP leading to vasodilatation.111,112 Moreover, nicorandil has been demonstrated to improve exercise duration and time to ischemia on stress test in patients with endothelial-dependent microvascular angina. 113
Clinical perspective
Taken together, the population of patients with chest pain and minimal coronary artery disease is at low risk of future cardiovascular events. However, the subgroup of patients with endothelial dysfunction is a possible exception to this rule that several studies have identified as being at higher risk of adverse cardiovascular events and atherosclerosis development. While further supporting evidence for the risk characteristics of this group is needed, there is an imperative developing to identify and treat these patients. Two questions are thus raised: (1) how is the subset of patients with endothelial dysfunction identified safely? and (2) what therapies are available to treat this condition?
Relying on endothelial provocation testing during angiography is unrealistic because in most cases it provides unnecessary risk to the patient with unclear benefit. However, if a patient is already undergoing angiography to rule out obstructive coronary artery disease, acetylcholine challenge using the strict protocol provided by Ong et al. 72 provides little additional risk and should be considered for prognostic and therapeutic purposes (see Figure 3 for workup and treatment algorithm).
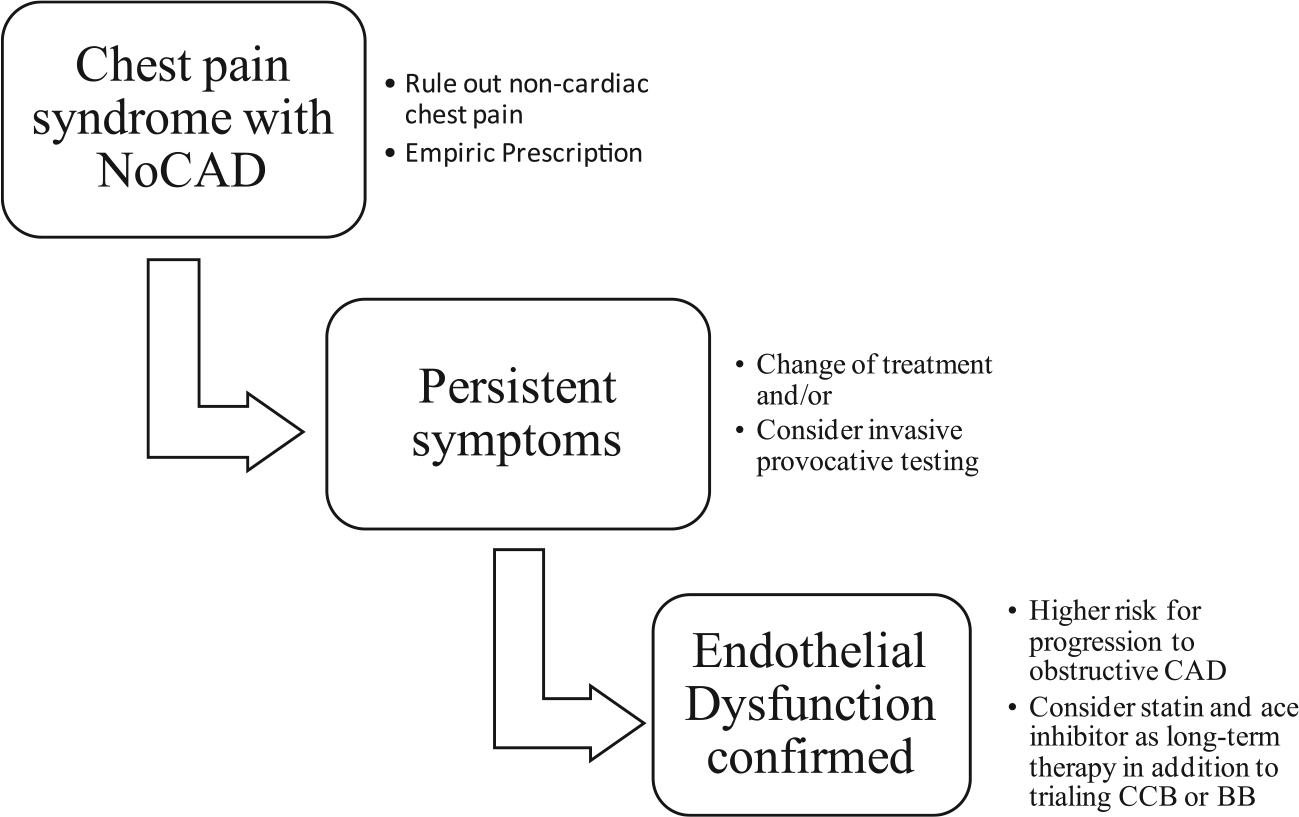
Proposed algorithm for diagnosis and treatment of coronary endothelial dysfunction. (NoCAD, non-obstructive coronary artery disease; CAD, coronary artery disease; CCB, calcium channel blocker; BB, beta-blocker.).
Patients suffering from NoCAD and endothelial dysfunction represent a large population of untreated or poorly treated patients. Currently, studies of therapies for endothelial dysfunction are limited in size and number. Of the currently used therapies, statins and ACE inhibitors have the most supportive evidence; however, it is still reasonable to trial nitrates, CCB and beta-blockers, as subsets of patients are responsive. New potential therapies such as nicorandil offer exciting potential but lack robust evidence to support their use.
New interest in the field of chest pain with NoCAD and a better understanding of risk within subpopulations will hopefully drive larger trials to be carried out and the development of new therapies. We can no longer ignore or dismiss these patients with chest pain.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.