
Abstract
Management of chronic disease often requires multidisciplinary clinical efforts and specialist care. With the emergence of Accountable Care Organizations (ACOs), health care systems are incentivized to evaluate methods of information exchange between generalists and specialists in order to provide value while preserving quality. Our objective was to evaluate patient and referring provider satisfaction and outcomes of asynchronous electronic consultations in vascular care in a large tertiary academic medical center. Referring providers were offered a vascular ‘e-consult’ option through an electronic referral management system. We conducted chart review to understand the downstream effects and surveyed patients and referring providers to assess satisfaction. From 24 March 2014 to 1 March 2015, 54 e-consults were completed. Additional testing and recommendations were made in 49/54 (90.7%) e-consults, including lower-extremity venous duplex ultrasonography with reflux testing, duplex ultrasonography of the carotid artery, computed tomography, magnetic resonance imaging, non-invasive physiology arterial studies, laboratory tests, medications, compression stockings, and sequential lymphedema compression therapy. Referring providers were compliant with recommendations in 40/49 (81.6%) of e-consults. A total of 17/54 (31.5%) patients were surveyed with a median patient satisfaction score of 13.7/15 (91.3%) (SD ± 6.4). The program was associated with high referring provider satisfaction, with 87.0% finding the e-consult very helpful and 80.0% stating it averted the need for a traditional visit. Our experience suggests that e-consults are an effective way to provide vascular care in some patients and are associated with high patient and provider satisfaction. E-consults may therefore be an efficient method of care delivery for vascular patients within an ACO.
Keywords
Introduction
Vascular disease is the leading cause of morbidity and mortality globally.1–4 Increasing vascular disease burden is a consequence of risk factors that are becoming more prevalent in the United States, including an aging population, obesity, tobacco use, poor diet, high blood pressure, dyslipidemia, diabetes and physical inactivity.4–6 The Centers for Disease Control and Prevention (CDC) suggests that successful management of chronic disease requires a multifaceted, integrated team approach including health care system interventions to improve the efficient use of clinical services while decreasing cost.7–9
At the same time, the Affordable Care Act (ACA) has encouraged quality and efficiency in treating patients with chronic disease, including by encouraging the development of Accountable Care Organizations (ACOs). 10 In the setting of increased specialist referral in the last decade, with the projected growth of work for vascular specialists, one method of increasing efficiency and value by ACOs is to develop novel methods integrating specialty expertise into primary care.11,12
The American College of Physicians has distinguished three types of interactions between generalists and specialists that could be enhanced to provide well-coordinated care while increasing value and impacting medical trend: (1) pre-consultation exchange; (2) formal consultation; and (3) co-management. Electronic consults (e-consults) have emerged as a mechanism to enhance provider communication and have demonstrated feasibility and facilitated timely specialty advice in a variety of settings. 13 At Massachusetts General Hospital (MGH), e-consults in outpatient cardiology enabled cardiologists to make recommendations to referring providers after reviewing a patient’s electronic medical record and imaging data. To date, this alternate form of consultation accounts for nearly 10% of cardiac consult requests and has been associated with high patient and provider satisfaction.14,15 While there are e-consult programs in a variety of specialties, to our knowledge there are no published reports evaluating a program for patients with vascular disease. In this context, an e-consult pilot program was launched in an outpatient vascular practice in an effort to validate its use for clinical communication and management of patients with vascular disease.
Methods
On 24 March 2014 we launched a vascular e-consult pilot program at the MGH, the largest hospital in New England. Referring clinicians within the hospital system were given the option in the existing electronic referral system to request either a traditional vascular consult or a vascular e-consult, depending on the clinical question and patient preference. The program was offered only to referring clinicians who were staff providers at the hospital because patient information (progress notes, laboratory data, imaging studies) is contained within a system-wide electronic health record available for specialist review.
Patients were selected for an e-consult at an office visit, typically during a primary care encounter. To answer a clinical vascular question, the referring provider would present the two vascular consult options to the patient. This included either referring the patient for a traditional face-to-face visit with a vascular specialist or referring the patient for a vascular e-consult in which the specialist reviews the patient’s chart and makes recommendations without requiring a visit. Both the patient and referring provider had to agree to a vascular e-consult before the referral. After the referral was submitted, the vascular specialist had an option of converting the e-consult to a traditional consult. Examples of e-consult requests that were converted to traditional consults included management of difficult-to-control hypertension in the setting of renal artery stenosis and management of symptomatic mesenteric ischemia. Two vascular specialists within the multispecialty Fireman Vascular Center (MRJ and VIP) performed all e-consults. The e-consult process mandated that the vascular specialist review a patient’s electronic medical record (EMR), including imaging, prior notes and laboratory values, and write a formal consultation note within 48 hours of the request and email a copy to the referring provider. The consultation must include the specific data and images reviewed, formal interpretation of the data, assessment and recommendations. Specialists spent approximately 10 minutes on an e-consult and were paid $54 per e-consult. The referring provider subsequently followed up with the patient by phone, mail or e-mail to communicate the specialist’s assessment, implement recommendations and answer any additional patient questions.
Data collection
We tracked the volume of vascular e-consults requested using the hospital’s electronic referral system. To confirm the accuracy of the administrative data, vascular e-consult charts were reviewed weekly by a vascular specialist (MDC). Data collection included the reason for the e-consult; whether a vascular specialist was seen within 90 days following the e-consult; any adverse events among patients who received e-consults including any emergency department visits or hospital admissions for a vascular problem within 90 days following the e-consult; and referring physician compliance with the specialist recommendations. This included tracking whether any medication adjustments were made, new therapeutic interventions initiated, or additional imaging and laboratory tests ordered. To ensure satisfaction with the process, a random sample of referring providers was surveyed using an electronic survey. All 54 patients were contacted once by phone to complete a telephone survey (Tables 1 and 2).
Patient satisfaction survey response distribution.
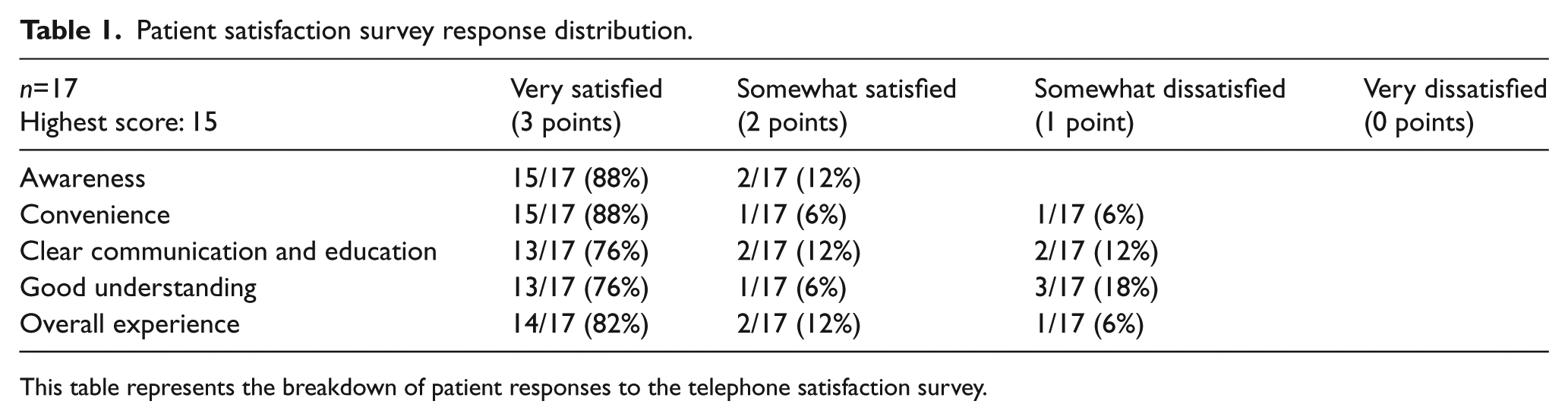
This table represents the breakdown of patient responses to the telephone satisfaction survey.
Referring provider electronic satisfaction survey response distribution.
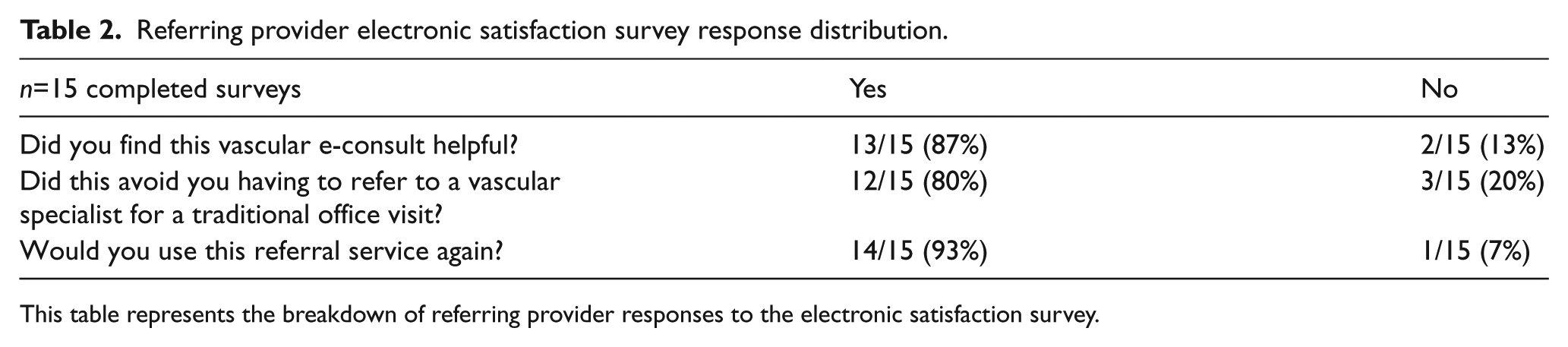
This table represents the breakdown of referring provider responses to the electronic satisfaction survey.
Results
From 24 March 2014 to 1 March 2015, 59 vascular e-consults were requested. Of those, 5/59 (8.5%) e-consults were changed to traditional face-to-face visits, as they were felt to be unanswerable by e-consult alone. In two of these situations, the problem was deemed too complex and in three of these situations the specialist desired an in-person consult with a physical exam to assess whether surgical/endovascular interventions might be indicated. A total of 54 e-consults were performed during the pilot phase. A total of 1632 vascular consults were requested during this time period, indicating that the total volume managed by e-consults was 54/1632 or 3.3% of all vascular requests (Figure 1).
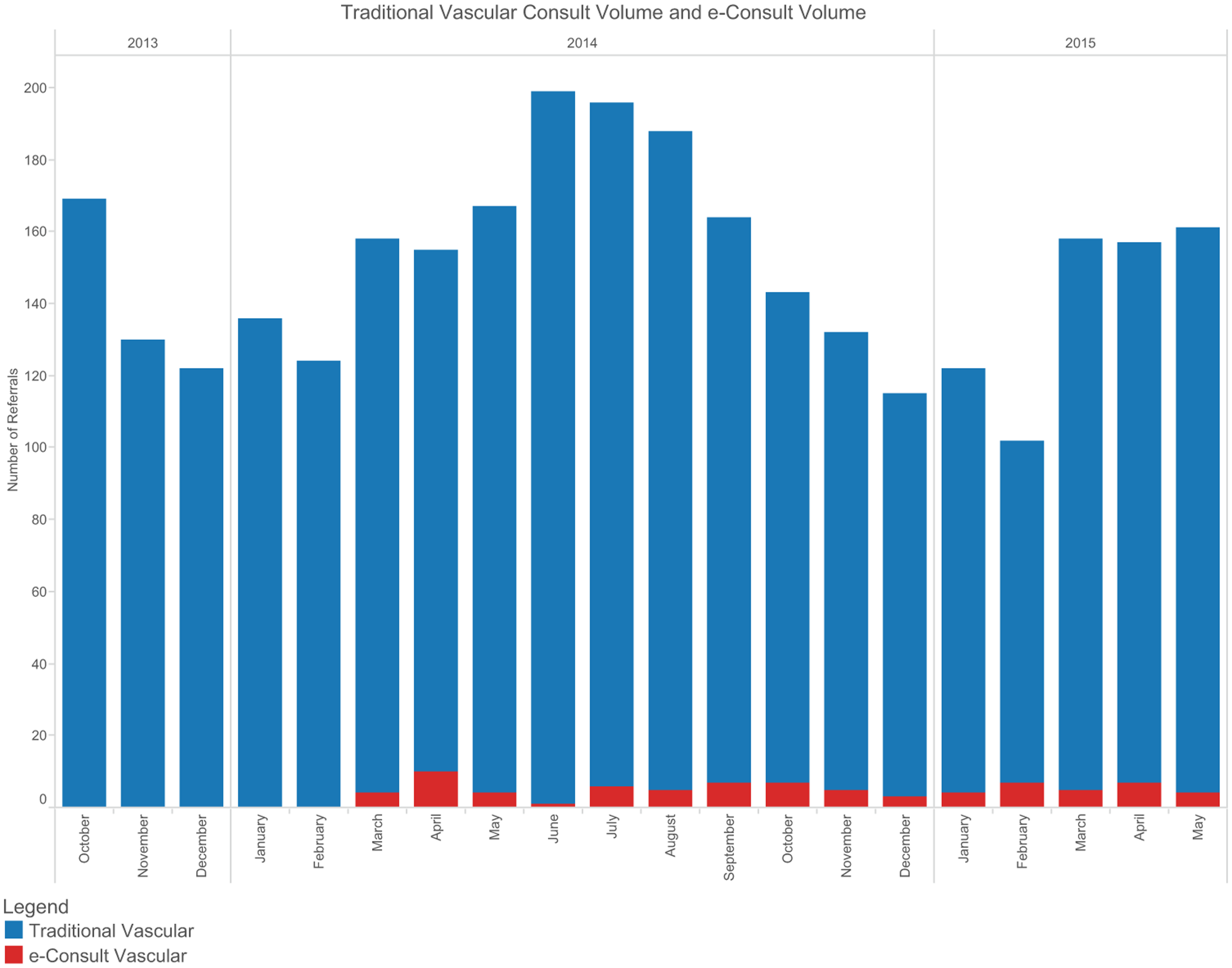
Traditional vascular consult volume versus e-consult volume.
Compliance with recommendations
Additional testing and recommendations were made in 49/54 (90.7%) e-consults including 23/49 (46.9%) lower-extremity venous duplex ultrasound exams with reflux testing; 6/49 (12.2%) duplex ultrasonography of the carotid artery, renal artery or abdominal aorta; 7/49 (14.3%) computed tomography (CT); 4/49 (8.2%) magnetic resonance imaging (MRI); 8/49 (16.3%) non-invasive physiologic arterial exams, which include ankle/brachial index (ABI) and pulse volume recordings (PVR) with the option of treadmill exercise testing; 4/49 (8.2%) laboratory tests; 24/49 (48.9%) medication additions or adjustments; 14/49 (28.6%) graduated compression stockings; and 2/49 (4.1%) sequential lymphedema compression therapy. Referring providers implemented all specialist recommendations in 40/49 (81.6%) of the e-consults.
Additional specialist visits
In 3/54 (5.5%) e-consults, a referral to a vascular specialist for further evaluation and discussion of surgical treatment options was recommended and the patient underwent a traditional face-to-face consult. Eight of 54 (14.8%) e-consult patients were formally seen by a vascular specialist for a non-urgent evaluation within 90 days of the e-consult. Five of these eight (62.5%) encounters were for persistent venous insufficiency unrelieved with conservative management for which the patient desired the opportunity to discuss more definitive treatment with a vascular specialist. Two of these eight (25%) encounters were at the request of the ordering primary care provider (PCP) who desired the patient to discuss the vascular issue with a specialist. One of the eight (12.5%) encounters was a patient’s previously scheduled routine annual visit with their cardiovascular specialist.
Safety
By chart review, none of the 54 e-consult patients had a death, emergency department encounter or hospitalization for a vascular issue within 90 days of the e-consult.
Referring provider and patient satisfaction
A sample of 17/54 (31.5%) patients were reached after one phone call attempt and all participants that were reached completed the telephone survey. To our knowledge there are no validated questionnaires for assessing patient satisfaction with e-consults, so we created a survey using a four-point Likert scale (Appendix 1). The response options ‘very satisfied, somewhat satisfied, somewhat dissatisfied and very dissatisfied’ were assigned a point value of 3, 2, 1 and 0, respectively. Each questionnaire score was summed and a final score assigned to each patient. A score of 15 represented the highest possible satisfaction level. The score was not normally distributed. Median patient satisfaction score was 13.7/15 (91.3%) (SD ± 6.4). Of these, 16 patients were ‘very satisfied or somewhat satisfied’ with the e-consult and one was ‘somewhat dissatisfied’, stating a preference for a traditional face-to-face visit with a vascular specialist. Of the 17 patients, 16 were either ‘very satisfied or somewhat satisfied’ with their understanding of the plan and recommendations and one was ‘somewhat dissatisfied’ as he/she noted being still unclear about the plan owing to still awaiting further testing and results (Table 1).
Of 54 referring PCPs, 15/54 (28%) completed a survey. There were 13/15 (87%) who found the vascular e-consult very helpful, 12/15 (80%) who felt that it avoided having to refer to a vascular specialist, and 14/15 (93%) who would use this service again (Appendix 2).
Discussion
The management of chronic conditions is complex and costly, requiring multiple interventions including preventative services, well-coordinated multidisciplinary clinical efforts and community-based programs.16–19 In response to these needs, ACOs have emerged with the aim of decreasing fragmentation, avoiding duplication and improving communication across the continuum of care. ACOs sign contracts with payers to provide care for a group of members at a specified contracted amount using either a shared savings (no risk) model or shared savings and losses model. When the ACO succeeds in meeting quality metrics and/or reducing a rise in health care costs, they share in the savings achieved. In the Medicare Shared Savings Program (MSSP), a model for Medicare beneficiaries, the ACO can share savings if it meets quality performance standards and reduces healthcare expenditures, which often pertain to cardiovascular disease.20–22 Unnecessary visits to specialists can therefore impair ACO performance by increasing unnecessary cost and restricting needed access. In this setting, facilitating generalist–specialist communication in efficient and patient-centered ways is essential to ACO performance.
New models for generalist-specialist information exchange have already shown promise in some fields. For example, at the University of California, San Francisco (UCSF) an Active Referral Management (ARM) system permitted specialist clarification of consultation questions, turning visit requests into electronic evaluations (eReferrals). These eReferrals provided a more productive, appropriate and effective first consult. The iterative pre-visit communication between specialist and PCP resulted in more complete work-ups by the PCP, prevented inappropriate referrals, decreased wait times and maintained high-quality care in community health clinics. 23 Furthermore, rheumatology eReferrals permitted pre-consultation exchange of information between generalist and specialist that enabled management and resolution of the clinical question without ever requiring a traditional visit. 24
Here, we have extended those results to vascular e-consults. Peripheral vascular disease represents a growing problem across the world, complicating outcomes of most chronic illnesses more than many other co-morbid conditions.25,26 We have validated the concept of delivering vascular care through e-consults in an ACO setting. In particular, we have demonstrated that vascular e-consults are associated with high rates of provider and patient satisfaction and low rates of subsequent traditional visits or emergency encounters.
This was performed at a single center, so it is difficult to extrapolate these findings to other care delivery systems. In addition, this was a pilot study. We have not tracked these patients beyond 90 days to determine their health status and if they eventually did see a vascular specialist in the traditional face-to-face environment after 3 months. While the satisfaction results were high in the population surveyed, limitations include a small sample size and low response rate from referring providers.
Concerns about miscommunication of information and legal risk may impair clinician and organization readiness to implement e-consults. We reviewed our e-consult process with risk management lawyers and we were able to reassure providers that this system would not place them at undue legal risk. While we restricted e-consults to referrals from internal hospital physicians only, this limitation was established in an effort to protect patient safety and reduce the potential for inadequate communication between providers by ensuring all providers had access to the same medical information in the EMR. Because of the lack of third party payer reimbursement, implementing and funding an e-consult program may depend on the health care system assuming shared risk. An ACO with a high proportion of patients with vascular disease in insurance risk contracts might find implementing a program a promising financial proposition. While we believe there is value in increasing access to vascular specialist care, further work is needed to evaluate long term value for patients. Continued monitoring of volume and long-term clinical outcomes is essential in order to further validate the effectiveness of this strategy for providing vascular care in an ACO setting. At this time we are unable to formally assess the quality of care delivered.
Conclusion
These findings suggest that vascular e-consults provide an effective mechanism for specialist generalist information exchange. This program was associated with high rates of provider and patient satisfaction.
Footnotes
Appendix
Acknowledgements
We greatly appreciate the contributions of Jennifer Bocklett, Sharon Fiumara and Tamika Jeune to our e-consult program and to this manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.