
Abstract
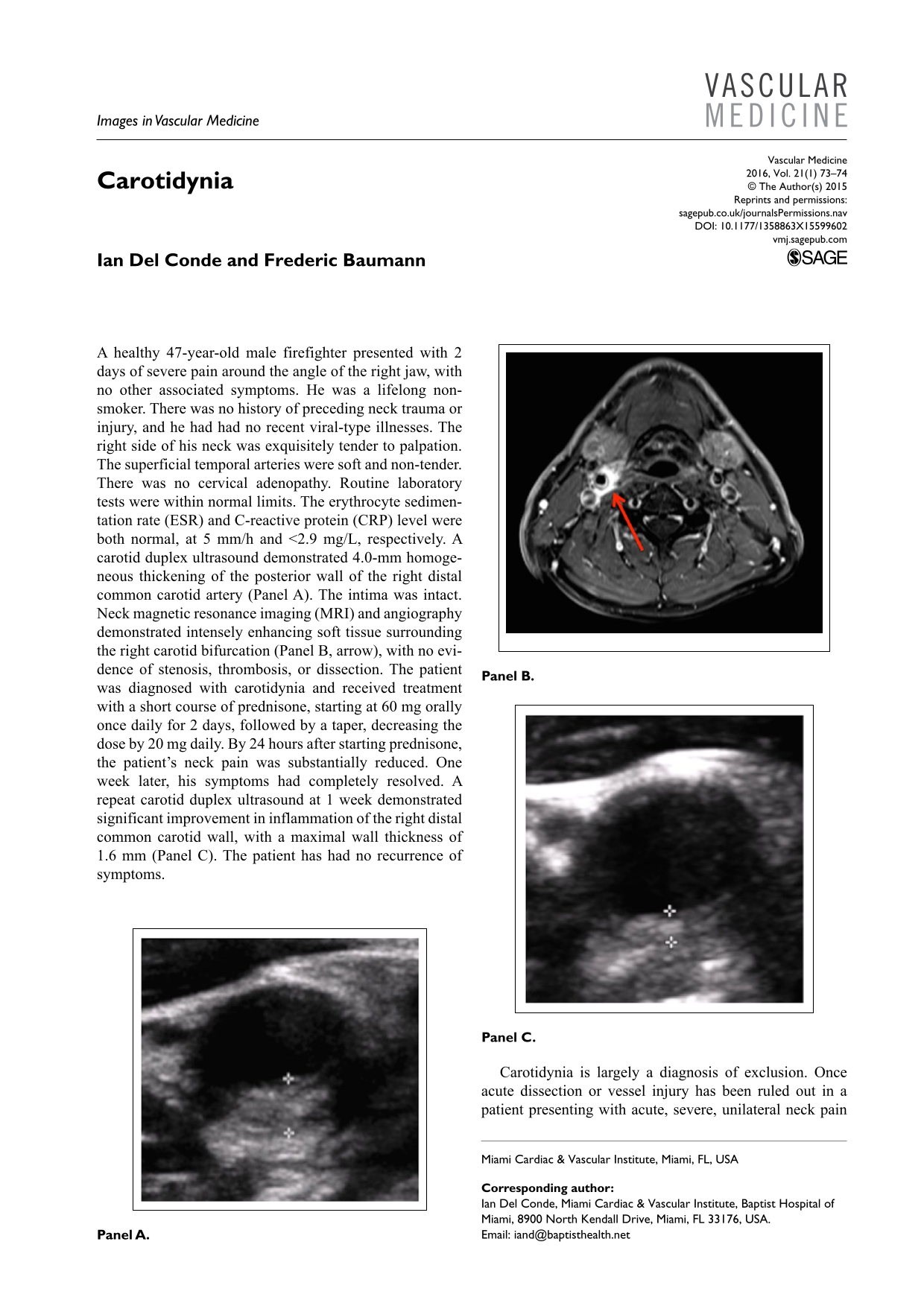
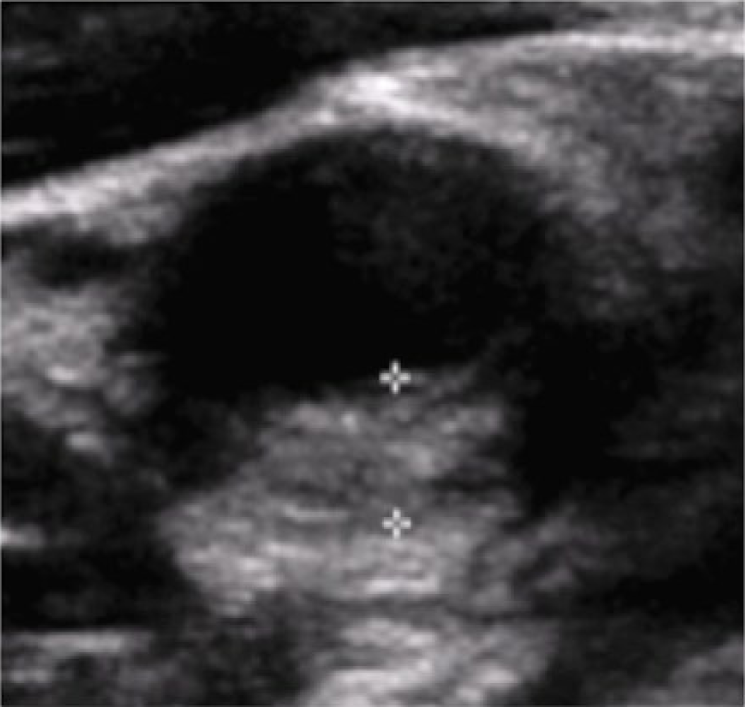
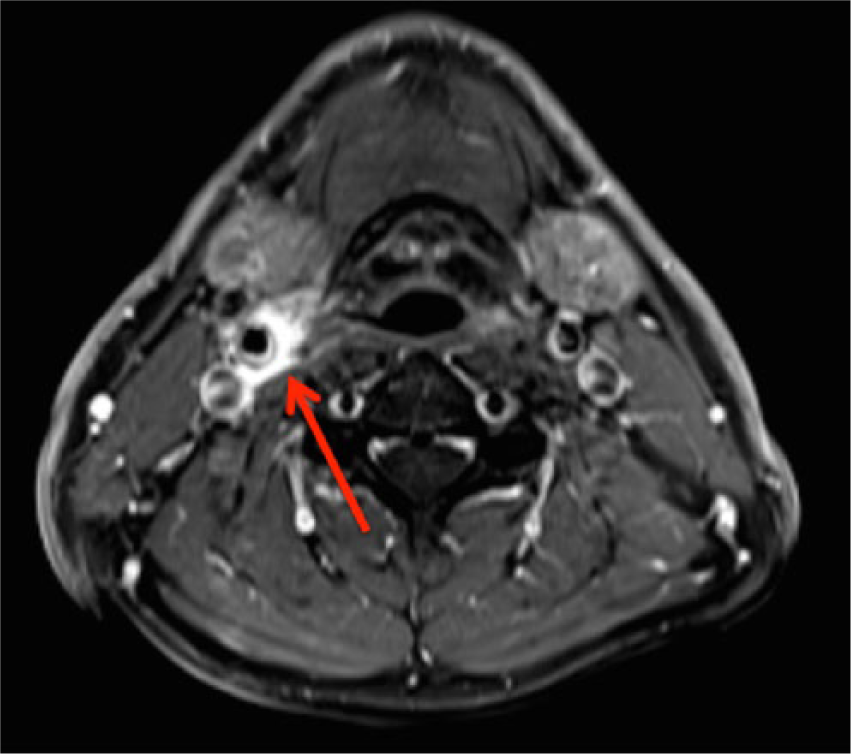
A healthy 47-year-old male firefighter presented with 2 days of severe pain around the angle of the right jaw, with no other associated symptoms. He was a lifelong non-smoker. There was no history of preceding neck trauma or injury, and he had had no recent viral-type illnesses. The right side of his neck was exquisitely tender to palpation. The superficial temporal arteries were soft and non-tender. There was no cervical adenopathy. Routine laboratory tests were within normal limits. The erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level were both normal, at 5 mm/h and <2.9 mg/L, respectively. A carotid duplex ultrasound demonstrated 4.0-mm homogeneous thickening of the posterior wall of the right distal common carotid artery (Panel A). The intima was intact. Neck magnetic resonance imaging (MRI) and angiography demonstrated intensely enhancing soft tissue surrounding the right carotid bifurcation (Panel B, arrow), with no evidence of stenosis, thrombosis, or dissection. The patient was diagnosed with carotidynia and received treatment with a short course of prednisone, starting at 60 mg orally once daily for 2 days, followed by a taper, decreasing the dose by 20 mg daily. By 24 hours after starting prednisone, the patient’s neck pain was substantially reduced. One week later, his symptoms had completely resolved. A repeat carotid duplex ultrasound at 1 week demonstrated significant improvement in inflammation of the right distal common carotid wall, with a maximal wall thickness of 1.6 mm (Panel C). The patient has had no recurrence of symptoms.
Carotidynia is largely a diagnosis of exclusion. Once acute dissection or vessel injury has been ruled out in a patient presenting with acute, severe, unilateral neck pain with evidence of carotid wall thickening, the diagnosis of carotidynia can be entertained. Although laboratory markers of inflammation are usually normal, 1 an inflammatory component is likely. With modern imaging modalities, carotid wall thickening and inflammation can be identified. 2 Histopathological studies could greatly improve our understanding of this disease.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.