
Abstract
The presence of bone tissue in calcified arteries may provide insights into the pathophysiology and potential reversibility of calcification, but the prevalence, distribution, and determinants of bone and osteoclasts in calcified arteries are unknown. Specimens of 386 arteries from lower limb amputations in 108 patients were examined retrospectively. Calcification was present in 282 arteries from 89 patients, which was medial in 64%, intimal in 9%, and both in 27%. Bone was present in 6% of arteries, essentially all of which were heavily calcified. Multiple sampling revealed that the true prevalence of bone in heavily calcified arteries was 25%. Bone was more common in medial rather than intimal calcifications (10% vs 3%, p=0.03) but did not vary with artery location (above vs below the knee). Heavily calcified arteries with bone were more likely to come from patients who were older (p=0.04), had diabetes (p=0.06), or were receiving warfarin (p=0.06), but there was no association with gender or renal failure. Bone was almost always adjacent to calcifications, along the periphery, but never within. Staining for the bone-specific proteins osteocalcin and osterix was noted in 20% and 45% of heavily calcified arteries without visible bone. Osteoclasts were present in 4.9% of arteries, all of which were heavily calcified and most of which contained bone. The frequent absence of bone in heavily calcified vessels and the histologic pattern strongly suggests a secondary rather than primary event. Recruitment of osteoclasts to vascular calcifications can occur but is rare, suggesting a limited capacity to reverse calcifications.
Introduction
Vascular calcification is a common lesion for which the pathophysiology and treatment remain uncertain. An intriguing finding is the presence of bone in some calcified arteries, which has important implications in terms of the pathophysiology and reversibility of the calcification as well as mechanisms for de novo bone formation. While the presence of bone has suggested that calcification is an osteogenic process, initiated through osteoblastic trans-differentiation of smooth muscle cells,1,2 bone is often not observed and osteogenic markers are not always present, 3 raising the possibility that osteogenesis is a secondary event. The conversion of calcifications to bone could render them more permanent as a self-perpetuating tissue, with reversal requiring changes in bone metabolism that would also affect the skeleton. Lastly, identification of factors responsible for bone formation in calcified arteries may provide insight into mechanisms for forming new bone.
Since the presence of bone in calcified arteries has not been extensively studied, its prevalence and epidemiology as well as its histology are unknown. This could provide clues to whether bone formation is a primary or secondary process, while identification of vessel-specific and patient-specific factors could help elucidate the underlying mechanisms and potentially lead to preventative measures. Although the focus has been on osteoblasts and osteoblastic transformation, osteoclasts are equally important bone-specific cells responsible for bone resorption. These cells would be necessary for removing bone from calcified arteries and may also be required to remove the other calcifications since they are also largely composed of highly insoluble apatite. 4 Yet, essentially, nothing is known about this process in calcified arteries.
Patients undergoing amputations provide an excellent opportunity to study these questions since this surgery is performed in a large number of patients with a variety of underlying conditions. A large proportion of these arteries are calcified, and specimens of all the major arteries are routinely prepared during pathologic examination. As part of a study on the histopathology of peripheral arterial disease, 5 arteries from amputation specimens were also examined for the presence of bone and osteoclasts.
Methods
Patients
Patients with peripheral arterial disease (PAD) and lower limb amputations were identified prospectively from searches of the surgical schedule and retrospectively from computerized searches of the electronic medical records. Cases were purposely selected so as to ensure adequate representation of patients with and without different risk factors. Amputations of the feet or toes and amputation performed for indications other than PAD (emboli, compartment syndromes, joint disease, neoplasms, trauma) were excluded. Individual medical records were reviewed to identify diabetes mellitus, end-stage renal disease (ESRD), smoking history, warfarin use, and baseline serum creatinine at the time of surgery. Diabetes mellitus was defined as a history of diabetes in the medical record or the use of insulin or oral hypoglycemic medications. ESRD was defined as outpatient dialysis. A smoking history included both present and past smoking. This protocol was approved by the Institutional Review Board of Emory University. Patient consent was not obtained since this was a retrospective study but patient information was anonymized and de-identified prior to analysis.
Histologic analysis
This was a retrospective study of prior surgical specimens, all processed in the Division of Anatomic Pathology according to standard procedures for paraffin embedment. In addition to the vascular margins, sections of specific arteries were also obtained, usually from heavily diseased segments as per standard protocol for surgical specimens. In the case of amputations below the knee, this usually resulted in two sections (proximal and distal) of each tibial artery. However, serial sections were not performed. For some specimens, the original tissue blocks were obtained and additional sections were prepared. Tissue sections stained with hematoxylin and eosin (H&E) were reviewed for this study. Calcification was delineated by the basophilic staining, usually present in large collections. In the medial layer this was graded semi-quantitatively from 1 to 4, where 1 indicates barely visible calcification, usually appearing as a dusting, and 2 through 4 indicate confluent areas of calcification comprising less than 10%, 10–50%, and >50% of the vessel circumference, respectively, as previously described. 5 Intimal calcification was graded on a similar scale except that grades 2–4 were assigned qualitatively. Bone was identified as dense, well-demarcated eosinophilic material that demonstrated linear birefringence with polarized light. Immature bone (also termed primary or woven) exhibited disarrayed linear birefringence while mature bone (also termed secondary or lamellar) exhibited parallel birefringence. Osteoclasts were identified as multinucleated giant cells with eosinophilic cytoplasm. Immunoperoxidase staining for SM22α, osteocalcin, and osterix was performed as previously described 3 using Clone 1A4 mouse monoclonal antibody (Sigma-Aldrich), OC4-30 mouse monoclonal antibody (Abcam), and rabbit polyclonal antibody, respectively (Abcam). Hematoxylin was used as a counterstain.
Statistics
Continuous variables are expressed as means ± standard errors and differences determined by two-tailed t-testing. Differences between categorical variables were determined by Fisher’s exact test for 2×2 comparisons and chi-squared testing for larger arrays.
Results
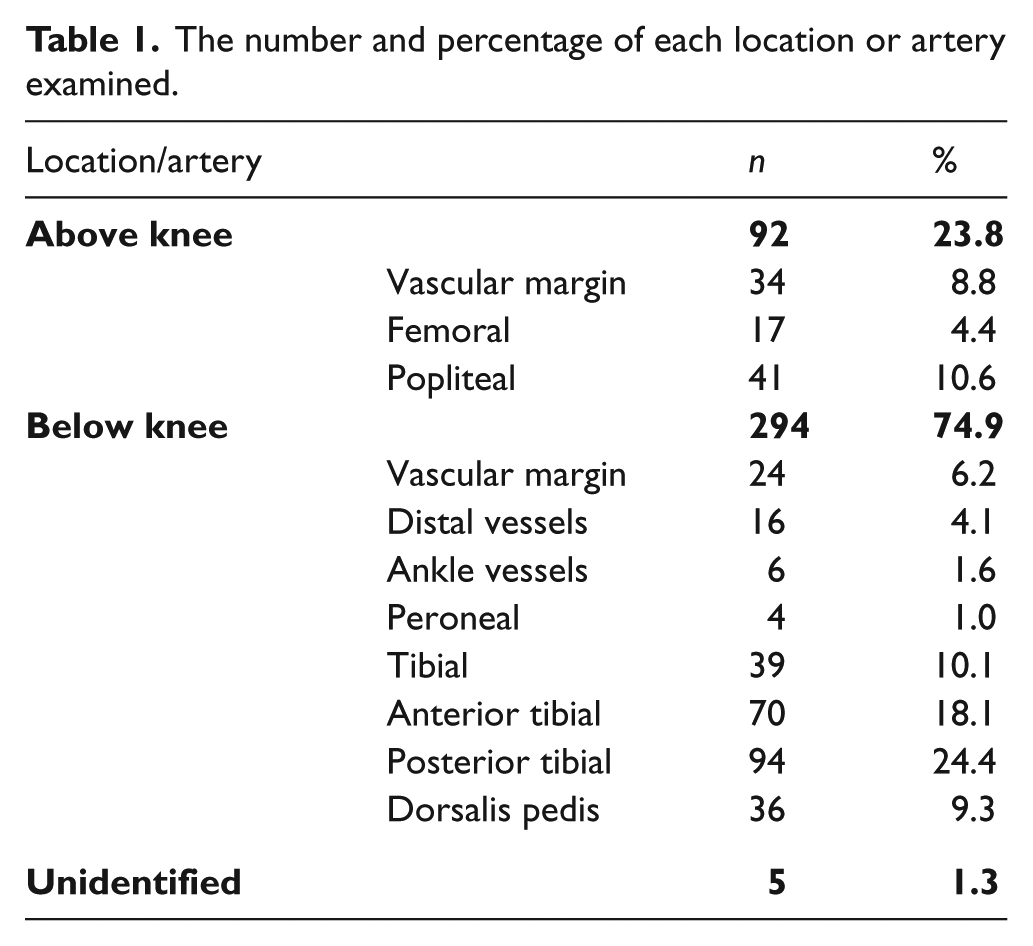
A total of 386 arteries from 122 amputations in 108 patients were examined, of which 49 amputations were above and 73 below the knee. The distribution of arteries is shown in Table 1. The mean number of arteries examined per patient was 3.6 and ranged from 1 to 11. Single arteries were available in 16 patients, two arteries in 23, three arteries in 23, four arteries in 18, five arteries in 10, and six or more arteries in 18 patients. Vascular calcifications were present in 282 arteries from 89 patients, as assessed by H&E staining, with medial calcification present in 64%, intimal calcification in 9%, and both in 27%. The characteristics of the patients with and without arterial calcification are shown in Table 2, and, as expected, age, diabetes, and ESRD were all associated with arterial calcification. Bone was identified in 23 arteries (6.0%) and, as shown in Figure 1, was present only in calcified vessels, all but one of which was heavily calcified (score of 3 or 4). The prevalence of bone was 9.9% in calcified arteries and 12.8% in heavily calcified arteries. To assess possible sampling errors, additional sections were prepared from the paraffin blocks of 43 specimens with severe calcification that did not contain bone on the original section. Bone was present in only five of these and in only one of 21 negative specimens sectioned for a third time. These additional five arteries with bone were included in the subsequent analyses. The results of multiple sectioning indicated that the true prevalence of bone in heavily calcified arteries is approximately 25%.
The number and percentage of each location or artery examined.
Characteristics of patients with amputations.
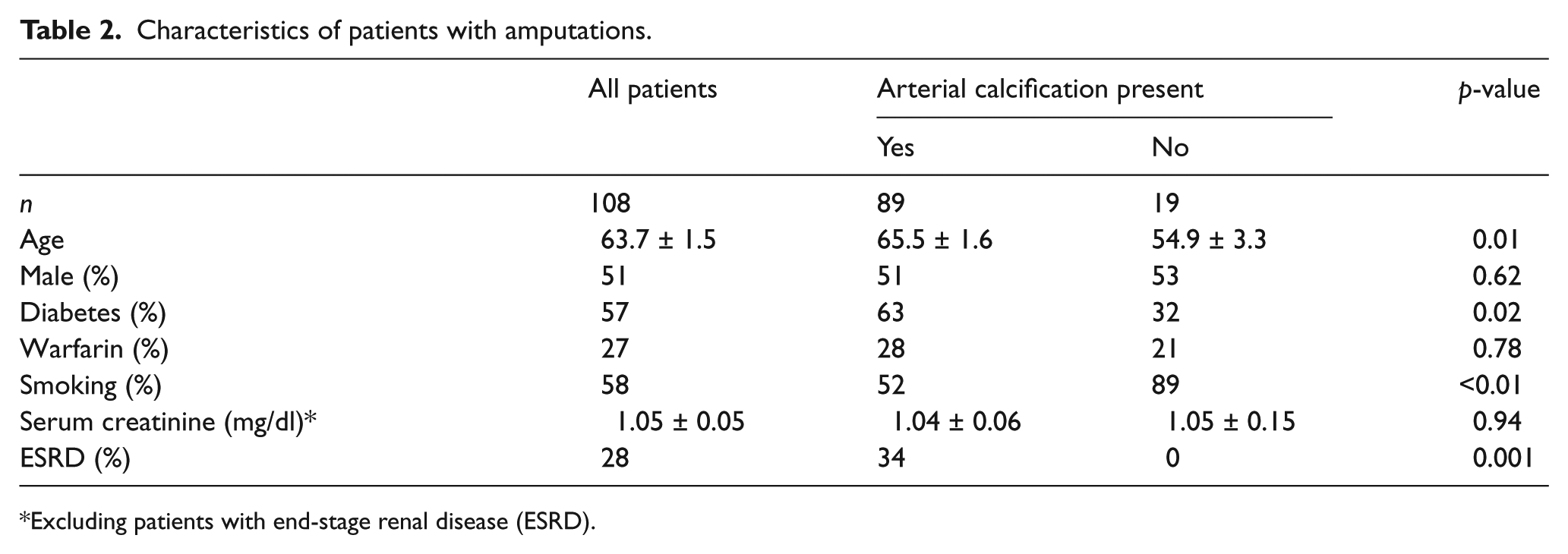
Excluding patients with end-stage renal disease (ESRD).
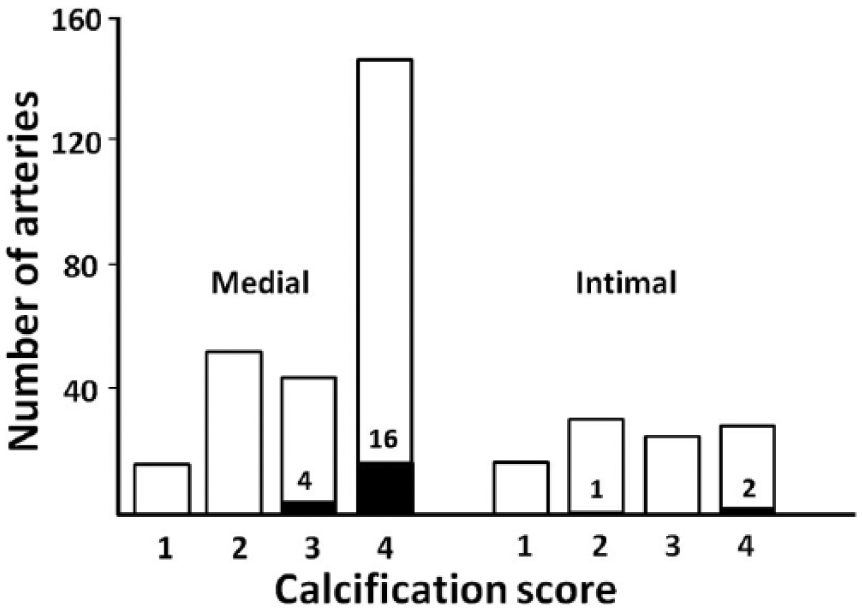
Effect of the severity of calcification on the prevalence of bone in calcified arteries. Left-hand bars: prevalence of bone within medial calcifications. Right-hand bars: prevalence of bone within intimal calcifications. A higher score indicates more severe calcification, as described in the ‘methods section’. Solid bars and numbers inside the open bars indicate the number of arteries with bone.
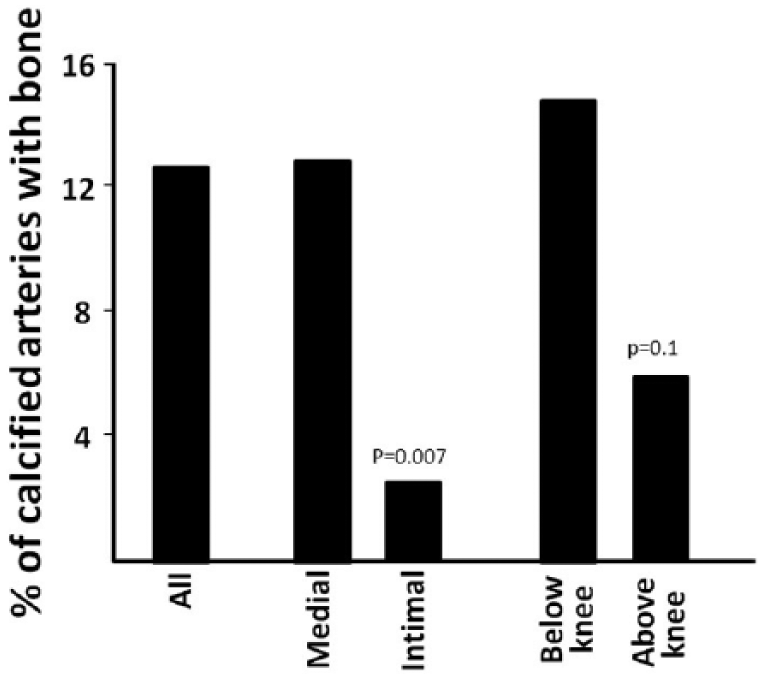
To identify factors associated with bone independent of the degree of calcification, subsequent analyses included only arteries with heavy calcification. As shown in Figure 2, bone was far more prevalent in regions of medial calcification than in regions of intimal calcification. While bone was more frequent in heavily calcified arteries located below the knee, this was not statistically different and is likely explained by the greater prevalence of medial versus intimal calcification in these arteries. 5 The relationship between patient characteristics and the presence or absence of bone in heavily calcified arteries is shown in Table 3. Heavily calcified arteries containing bone were more likely to come from older patients and from patients with diabetes or receiving warfarin, although the latter two associations were of borderline significance. There were 15 patients with arterial bone from whom more than one artery with heavy calcification was available. Of these 58 additional arteries (excluding the first calcified artery for each patient), the prevalence of bone was 21% compared to the 9% in all the other heavily calcified arteries (p<0.05), indicating a clustering of bone-containing arteries within patients.
Anatomical characteristics of bone in heavily calcified arteries.
Patient characteristics of heavily calcified arteries with and without bone.
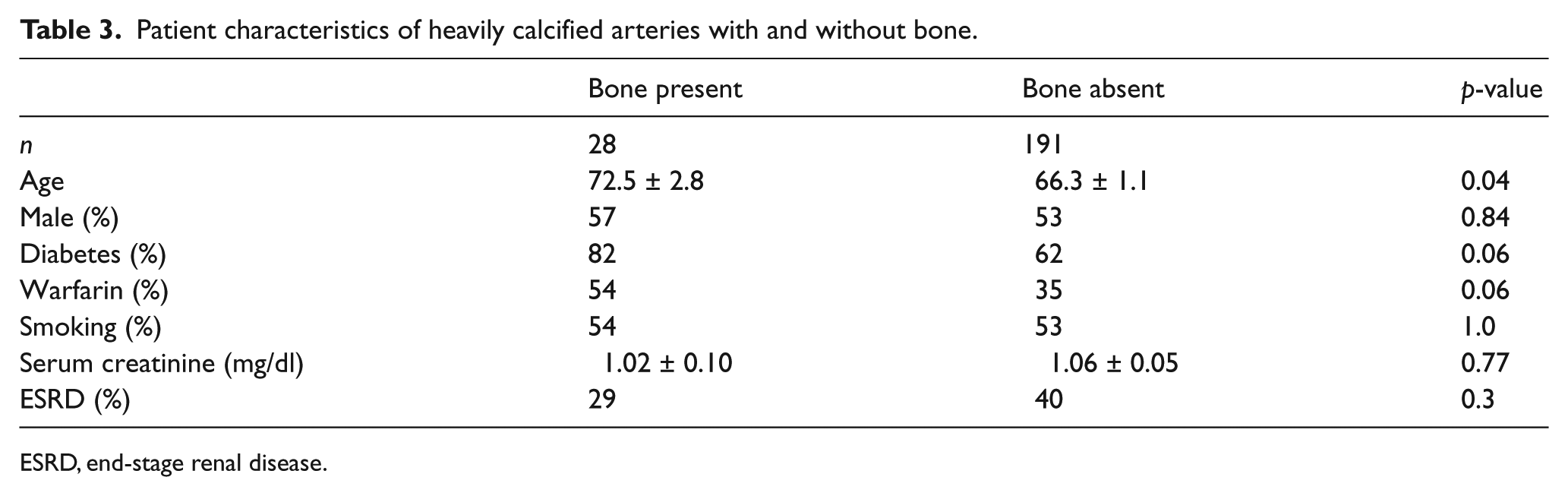
ESRD, end-stage renal disease.
In addition to patients with severe PAD, we identified 10 patients with amputations performed for other indications: six were performed for cancer, two for prosthesis malfunction, one for osteomyelitis, and one for acute embolus. Of the 15 arteries examined, five had no calcification and only two had severe calcification. Bone was not detected in any of the arteries.
The histology of bone within calcified arteries is shown in Figure 3. The majority of sections lacked any visible bone, despite very heavy calcification (Figure 3A). Bone was always along the periphery of the calcifications (Figures 3B and 3C) and in only a single section was bone present without adjacent calcifications (Figure 3D). Mature lamellar bone with marrow was rarely observed (Figure 3E), and in no cases was cartilage observed. It is clear from these images that even when present, bone was absent from much of the calcifications. Osteoclasts (Figure 3F) were observed in 4.9% of arteries, all of which were heavily calcified. The prevalence in heavily calcified arteries was 8.7%. The ability to identify osteoclasts was limited by the fact that almost all of these arteries underwent acid decalcification, which precluded staining for tartrate-resistant acid phosphatase. Of the arteries in which osteoclasts were found, 63% contained bone. With the exception of one specimen in which osteoclasts appeared to be resorbing calcifications (Figure 3F), osteoclasts were not immediately adjacent to the calcifications. No patient characteristics correlated with the presence of osteoclasts but the sample was small.
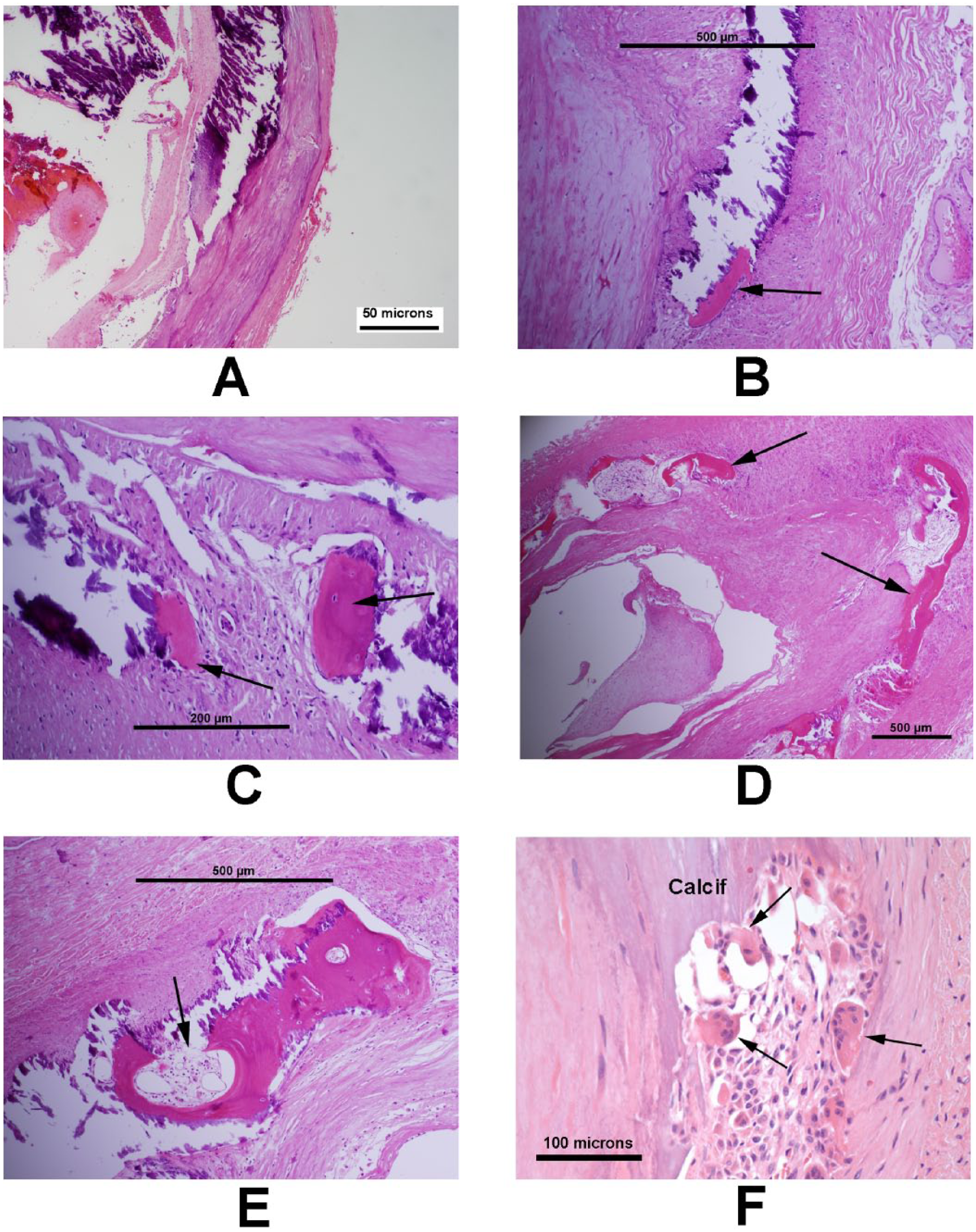
Bone in calcified arteries. (A) Heavily calcified artery without bone. (B and C) Bone (arrows) adjacent to calcifications. (D) Bone (arrows) surrounding a calcification. (E) Mature lamellar bone with marrow (arrow). (F) Osteoclasts (arrows). The two osteoclasts on the left appear to be resorbing the calcification (calcif). (Hematoxylin and eosin stains.)
Since very early stages of bone formation may not be recognized by H&E staining, additional sections of heavily calcified arteries without apparent bone were stained for the bone-specific protein osteocalcin and the bone-specific transcription factor osterix (Figure 4). There was frequent staining of the calcifications for osteocalcin, as previously observed, 3 that likely represents either binding of circulating osteocalcin or non-specific binding of the antibody to the calcifications. Cellular staining was observed in only two of 10 sections. Cellular staining for osterix was observed in five of 11 sections. Antibody specificity was confirmed in sections of human bone and neonatal mouse spine as previously described. 3 Since osteogenic transformation should be accompanied by loss of smooth muscle phenotype, arteries were also stained for the smooth muscle-specific protein SM22α. As shown in Figures 4E and 4F, there was robust staining of cells immediately adjacent to and within calcifications. While some calcifications showed little adjacent staining, this was due primarily to cell loss rather than loss of staining.
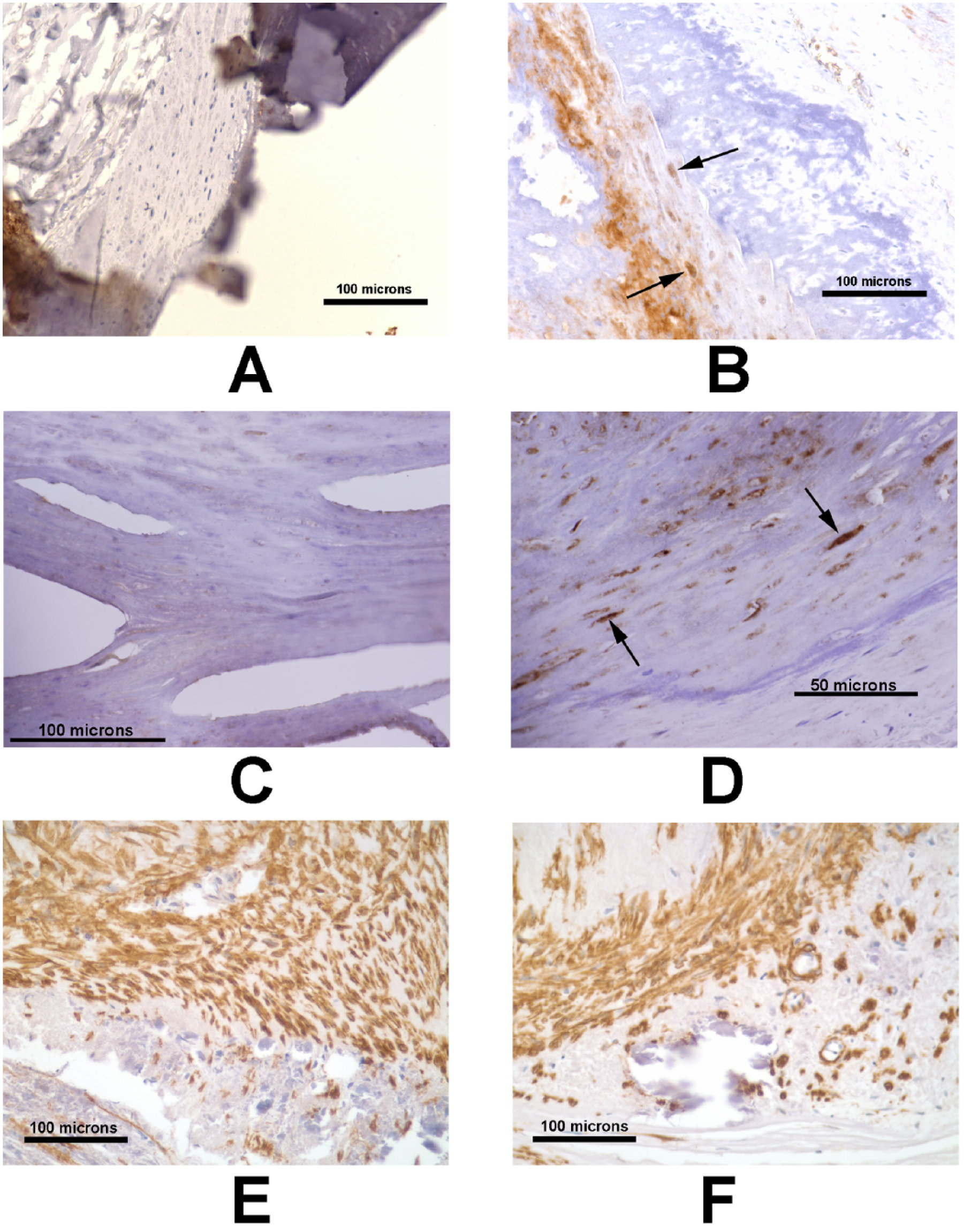
Immunohistochemistry of calcified arteries. Negative (A) and positive (B) cellular staining (arrows) for osteocalcin in heavily calcified arteries. Note the non-specific staining of calcifications. Negative (C) and positive (D) cellular staining (arrows) for osterix in heavily calcified arteries. There is also non-specific staining of calcifications. Staining for SM22α revealed staining of smooth muscle cells immediately adjacent to (E) and within (F) calcifications.
Discussion
In this large sample of lower extremity arteries from patients with PAD and critical limb ischemia, bone was present in only 6% on initial review and was limited almost entirely to severely calcified vessels, in which the prevalence was two-fold higher. Whether this rarity is due to sampling error or to the fact that most calcified vessels do not contain any bone was addressed by examining multiple sections of single arteries. While this increased the yield of bone, the increase was minimal by the third section, indicating that bone was absent in three-quarters of heavily calcified arteries. The prevalence of bone in calcified arteries has not previously been reported, but the paucity of bone was consistent with a previous study in calcified human heart valves, 6 of which only 13% contained bone.
The absence of bone in most of the heavily calcified arteries cannot be explained by an inability to detect early bone formation since osteocalcin was detected in only 20% of heavily calcified arteries devoid of bone. Osterix, a bone-specific osteogenic transcription factor, was detected more commonly, indicating either very early osteogenesis or that osterix expression does not necessarily lead to osteogenesis. Previous studies have implicated osteogenic differentiation of smooth muscle cells as an initial event in vascular calcification based on the expression of osteogenic genes and proteins in calcified arteries from humans7,8 and animal models. 2 However, many of these genes, such as osteopontin, alkaline phosphatase, and Runx2, are not specific for bone, and a previous study of early calcification in human breast arteries was unable to demonstrate expression of more specific osteogenic proteins. 3 Furthermore, a concomitant loss of smooth muscle phenotype, as indicated by staining for SM22α, was not observed in calcified peripheral arteries. The results are consistent with other mechanisms for vascular calcification such as loss of endogenous inhibitors or changes in extracellular matrix rather than osteogenic transformation of vascular smooth muscle.
When detected, bone was almost always immediately adjacent to the calcifications along the periphery and appeared to represent de novo formation, akin to intramembranous formation in the skeleton, since cartilage was not observed. Both immature (primary or woven) and mature (secondary or lamellar) bone were present, as indicated by disarrayed or parallel linear birefringence, respectively, of the collagen fibers. Although cartilaginous metaplasia has been described in a number of animal models of cardiovascular calcification,9–11 endochondral bone formation has rarely been reported in human arteries 12 and was observed in less than 2% of calcified heart valves. 6 This appears to be an important distinction between animal models and human disease that may be related to the differences in bone physiology between adult rodents and humans.
The paucity of bone in calcified arteries, its restriction to heavily calcified arteries, and its location on the periphery of calcifications and never within, strongly suggest that bone formation is a secondary event in vascular calcification. The fact that staining for osteogenic markers was absent in the majority of heavily calcified arteries also argues against a primary role for osteogenic transformation. The possibility that calcification can induce osteogenesis is supported by the finding that hydroxyapatite induces Runx2 expression in vascular smooth muscle cells in culture. 13 Alternatively, the calcifications could attract circulating osteoblastic precursor cells as evidenced by the presence of circulating osteogenic precursors expressing osteocalcin in calcified aortic valves. 14 The presence of bone in up to one-quarter of heavily calcified arteries has therapeutic implications. Once formed, arterial bone would be a self-perpetuating tissue whose metabolism would be similar to skeletal bone. Thus, formation could continue under normal conditions and could only be prevented by measures that prevent bone formation in general. Likewise, therapies to resorb arterial bone would have similar deleterious effects on the skeleton.
It was clear that the parameter most strongly associated with bone formation was the severity of calcification. After accounting for that by including only heavily calcified arteries in the analyses, there appeared to be some anatomic specificity. Bone was much more likely to be associated with medial rather than intimal calcification. The significance of this is unclear but could be related to the different pathophysiologies of these distinct lesions. However, since medial calcification was usually more extensive than intimal calcification and there was no reliable method to compare the severity of the two, the predilection for the media could be explained in part by the severity of the calcification.
Patient-specific factors also appeared to determine the presence of bone in heavily calcified arteries since arterial bone was more common when other arteries from the same patient contained bone. Arterial bone was more likely to occur in older patients and patients with diabetes or receiving warfarin, although the latter two associations were of borderline significance. Warfarin promotes vascular calcification by reducing the carboxylation and activity of matrix Gla protein, an endogenous inhibitor of calcification.15,16 This protein also binds and inactivates bone morphogenic protein 2, 17 which is expressed in calcified arteries, 18 possibly explaining the greater prevalence of arterial bone in patients receiving warfarin. However, age, diabetes, and warfarin are all risk factors for medial calcification and, despite attempts to control for this, could be influencing bone formation merely through more severe calcification that was not discernible in our qualitative assessment. The fact that these risk factors do not affect the severity of medial calcification in amputation specimens 5 would argue against this. Also, ESRD was not associated with arterial bone, although it is associated with greater medial calcification in amputation specimens. 5
Osteoclasts were notably rare in calcified arteries. Since arterial calcifications are composed of apatitic and other highly insoluble forms of calcium, 19 a biologic process akin to osteoclastic resorption in bone would be required for their removal. The occasional presence of osteoclasts demonstrates that they can be recruited to vascular calcifications but their rarity indicates that this process is impaired in most cases. There was no apparent pattern to this except that osteoclasts were only found in heavily calcified arteries and usually ones containing bone, consistent with recruitment through secretion of cytokines such as RANK ligand by osteocytes. The paucity of osteoclasts implies a limited capacity for reversal of vascular calcifications and that failure to recruit osteoclasts contributes to the severity of vascular calcification.
This study was limited to lower extremities and vascular calcification is known to vary between arterial beds. However, this variability relates primarily to the propensity to develop calcification and the type of calcification. While the calcification in lower extremity arteries is mostly medial, intimal (atherosclerotic) calcification was also present and presumably is representative of the intimal calcification that is common in the coronary and central arteries. Because of the predilection of bone for medial calcification, it is unlikely that bone would be more prevalent in these other arteries.
Clinical Significance
This study demonstrates for the first time the frequency and anatomic distribution of bone and osteoclasts within arterial calcifications, as well as associated patient characteristics. The data have implications for the pathogenesis of vascular calcification in that bone formation appears to be a secondary and not primary event, and implications for therapy in that bone formation and the paucity of osteoclasts would render calcification difficult to reverse.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.