
Abstract
Vascular endothelial-cadherin is the most important transmembrane component of endothelial adherens junctions, exclusively expressed by endothelial cells in all types of vessels. Targeting either the extracellular domain or the cytoplasmic tail deleteriously affects the junctional strength and leads to vascular permeability. Recently, cytokine-induced phosphorylation of the vascular endothelial-cadherin cytoplasmic domain was reported to trigger cleavage of its extracellular domain, producing the soluble form of the protein – soluble vascular endothelial-cadherin. Hence, the presence of soluble vascular endothelial-cadherin or auto-antibodies to human vascular endothelial-cadherin in human serum could signalize the presence of vascular abnormalities. This systematic review covers many human studies reporting increased levels of soluble vascular endothelial-cadherin, as well as auto-antibodies to human vascular endothelial-cadherin, which could be promising biomarkers of endothelial dysfunction in a large panel of diseases.
Introduction
Cohesion between endothelial cells is maintained by specialized structures known as intercellular junctions, which control the flow of solutes between the bloodstream and adjacent tissues, allowing white blood cells access to tissues at infection and inflammation events. In the quiescent state the intercellular adhesion depends on various transmembrane proteins called adherens or tight junctions, which are located in junctional structures and distributed throughout the zone of contact. Vascular endothelial-cadherin (VEC) is the most important amid the transmembrane component of these endothelial adherens junctions, being expressed exclusively in endothelial cells of arterial, venous and lymphatic vessels.
VEC is believed to play a major role in maintaining the integrity of endothelial cell contacts and the stability of endothelial junctions. More recently, it has been shown that the extracellular domain of VEC can be cleaved upon cytokine-induced phosphorylation of its cytoplasmic domain 1 and released into the blood stream as soluble VEC (sVE). sVE has been detected both in human serum and ex vivo in conditioned media used for endothelial cell cultivation. 2 Even if its role remains unclear, serum sVE levels could be increased in patients suffering from vascular abnormalities, with several published clinical studies describing how sVE can be used to diagnose vascular disorders.
In this review, we carefully look at various clinical studies to explore the possibility of sVE being used as a new biomarker of endothelial dysfunction. Additionally, a recent study has reported a method to identify auto-antibodies to human VEC (AAVEs) in human serum from patients suffering from several autoimmune diseases. AAVEs directed against the extracellular domain of VEC seem to increase vascular permeability and could also be used as a new biomarker of endothelial dysfunction.
Vascular permeability and VEC forms found in animal studies and human disease conditions
The major role played by VEC in maintaining the integrity of endothelial adherens junctions was shown in animal studies using VEC-deficient mice, which did not develop beyond mid-gestation due to severe vascular abnormalities. Endothelial cells were not fully organized into large vessels and angiogenesis was impaired in the embryos.3,4 A similar phenotype was observed in mice expressing partially truncated VEC, which lacks the cytosolic domain but retains the extracellular part, with the authors arguing that intracellular beta-catenin signaling is critical for VEC’s function during vascular morphogenesis. 4
Mutations in the VEC gene have not yet been reported in humans but abnormal vascular structures have been observed in several human diseases such as cerebral cavernous malformation (CCM). Analysis of endothelial junctions in CCM showed significant disorganization of venous vessels in the central nervous system associated with decreased VEC expression and markedly upregulated expression of N-cadherin and mesenchymal markers.5–8 These alterations lead to increased levels of perilesional erythrocytes and fluid oozing.
Almost all diseases involving inflammation – particularly tumors inducing an angiogenic process – could be associated with cell–cell adhesion defects. Cellular adhesion molecules play a key role in maintaining barrier functions such as regulating permeability and controlling leukocyte transendothelial migration, a crucial step during inflammation. The increased permeability observed during inflammation is mainly a consequence of reorganization of junctional proteins like VEC, leading to a transient loosening process of endothelial junctions. Actually, changes in the endothelial cell cytoskeleton and disruption of junctional adhesion molecules observed in human diseases have been linked to intracellular redistribution of VEC.
Some therapeutic approaches were already tested in animal models by exploring the stabilization of adherens junctions, thus reducing vascular permeability. 9 In hypoxic conditions, found within tumors for example, endothelial cell permeability is induced by vascular endothelial growth factor (VEGF), a factor thought to trigger enhanced VEC endocytosis. Vascular abnormalities are often observed in the tortuous capillary network of vessels feeding tumors (more permeable to macromolecules), which have significantly larger diameters than ‘normal’ vessels. 7 Still in the tumor context, it has been reported that certain epitopes of the VEC molecule can be exposed to the local environment prior to the formation of trans-adhesion dimers at endothelial cell–cell contacts. These temporarily exposed epitopes are accessible to monoclonal antibodies (mAbs), which can prevent cell–cell adhesion from occurring and consequently impair angiogenesis. Other epitopes remain accessible regardless of whether or not adhesions have formed, and are thus always prone to disruption.10,11 Among the VEC modifications affecting its adhesive functions, a few reports have pointed out that endocytosis or intracellular degradation12,13 induced by challenge with VEGF plays a relevant role. Moreover, it has been also suggested that tyrosine phosphorylation of components of the cadherin–catenin complexes – beta-catenin, plakoglobin, VEC and other cadherins (E- and N-cadherins) – correlate well with the dissociation of endothelial cell layers (i.e. through dissociation of the cadherin–catenin complex).14,15 The cytoplasmic domain of VEC bears nine putative tyrosine phosphorylation sites, including Y658, Y685 and Y731, which have been individually implicated in controlling barrier integrity. Although several kinases are thought to contribute to VEC phosphorylation, the exact mechanism explaining how tyrosine phosphorylation leads to vascular leakage still remains elusive. More recently, evidence was produced showing that VEC tyrosine phosphorylation precedes cleavage of its extracellular domain to produce sVE (Figure 1); 1 and that proteolytic cleavage of cell surface proteins appears to be mediated by members of the metzincin superfamily of zinc-dependent proteases, including the matrix metalloproteinases (MMPs) and ADAMs (a disintegrin and metalloproteinase). 16 The MMPs and adamalysins were considered to be major mediators of cartilage destruction in rheumatoid arthritis (RA). Also, interestingly, MMP-2, MMP-7 and MMP-9 are the foremost documented ones, involved in the induction of VEC cleavage in several physiological events, namely apoptosis, diabetic retinopathy and dengue virus infection. Adamalysins such as ADAM-9 and ADAM-10 have been shown to mediate VEC cleavage during retinal neovascularization and in human umbilical vein endothelial cells (HUVECs) upon thrombin stimulation, respectively.16,17
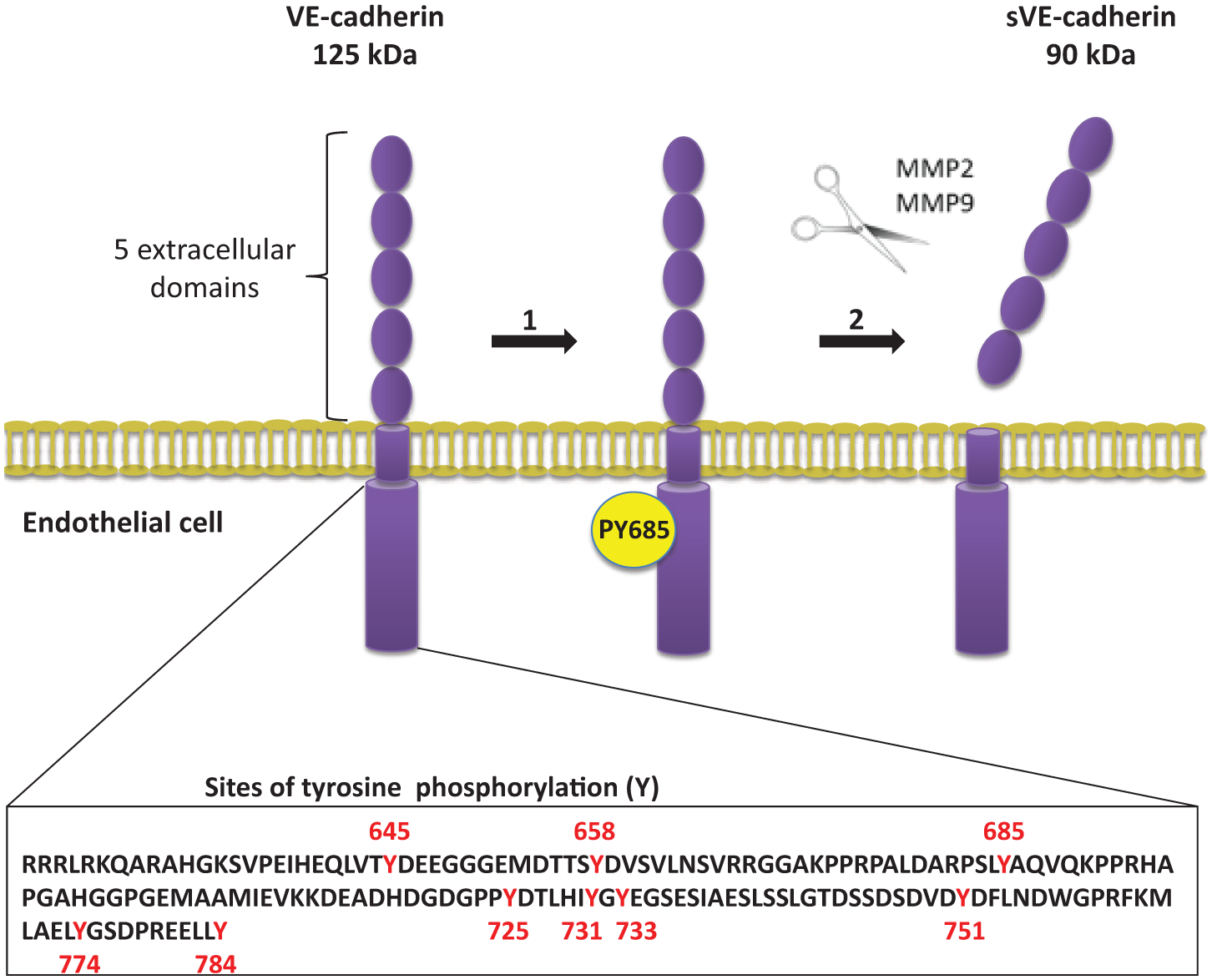
Schematic figure of vascular endothelial-cadherin (VEC) structural modifications resulting in cleavage: VEC can undergo phosphorylation at site Y685, which is located in a consensus domain for Src family kinases. This phosphorylation precedes VEC cleavage of the extracellular domain, known as sVE.
sVE is the focus of this systematic review aiming at exploring how its levels correlate with human diseases, their prognosis and responsiveness to treatment, based on published literature available by September 2014.
Review of clinical studies
A search was performed using the MEDLINE database in September 2014 to retrieve clinical studies by entering the keywords: ‘sVE-cadherin’ (eight papers), ‘soluble VE-cadherin’ (42 papers), ‘VE-cadherin cleavage’ (17 papers) and ‘VE-cadherin shedding’ (13 papers). Only clinical studies where sVE has been quantified in human populations were considered for further analysis, irrespective of the quantitation method used. A total of 15 studies were found in which sVE levels were determined in human serum withdrawn from patients expressing microvascular endothelial dysfunction. Diseases included systemic vasculitis, inflammatory skin diseases or tumors (Figure 2, Table 1). Most of the studies were open, with only a few comparing the results from patients to a healthy group of individuals (controls).
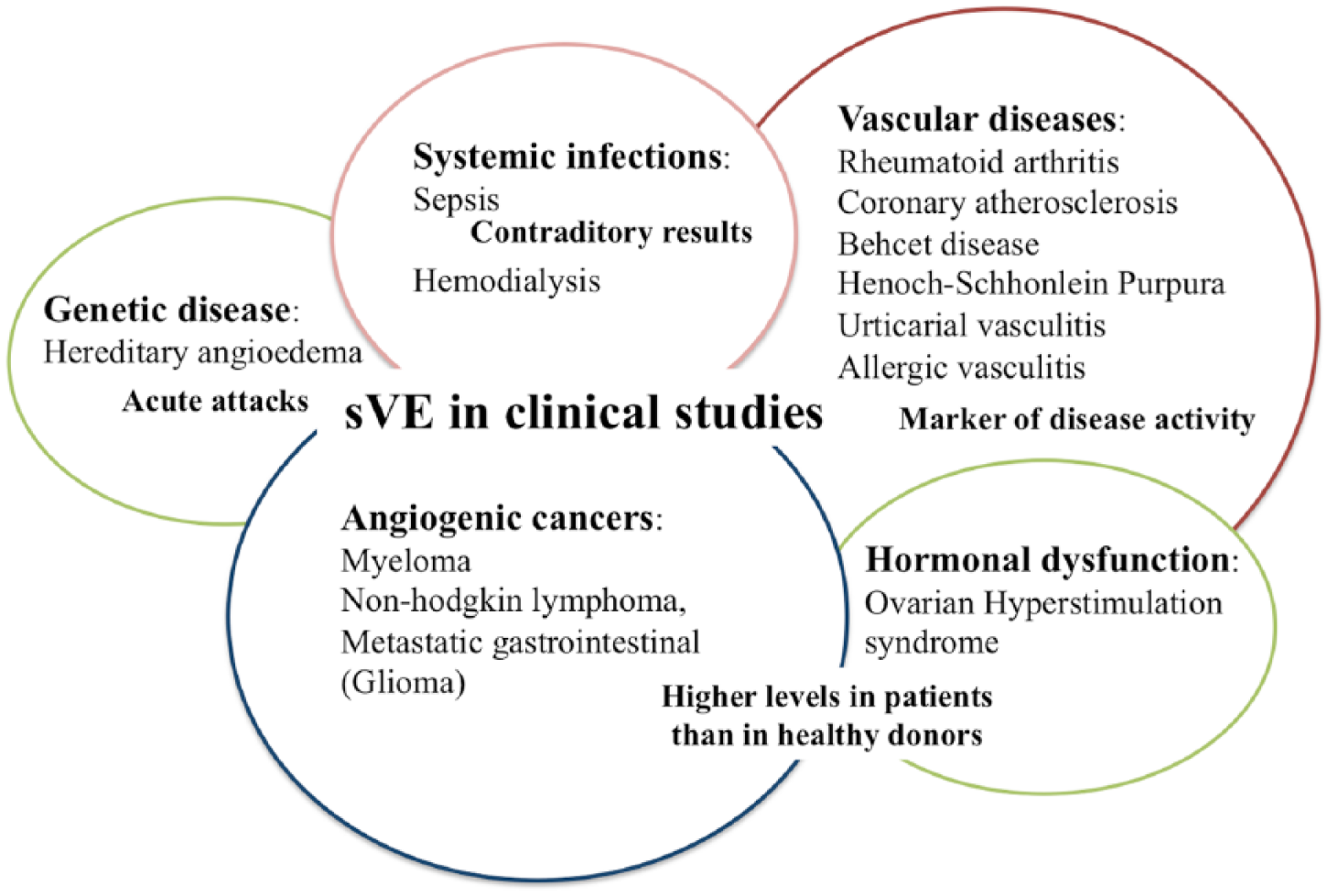
Schematic diagram of clinical studies that analyzed soluble vascular endothelial-cadherin (sVE) in serum from patients with several diseases exhibiting microvascular endothelial dysfunctions. (Source: Medline until September 2014.)
Overview of clinical studies where soluble vascular endothelial-cadherin (sVE) was measured in human serum.
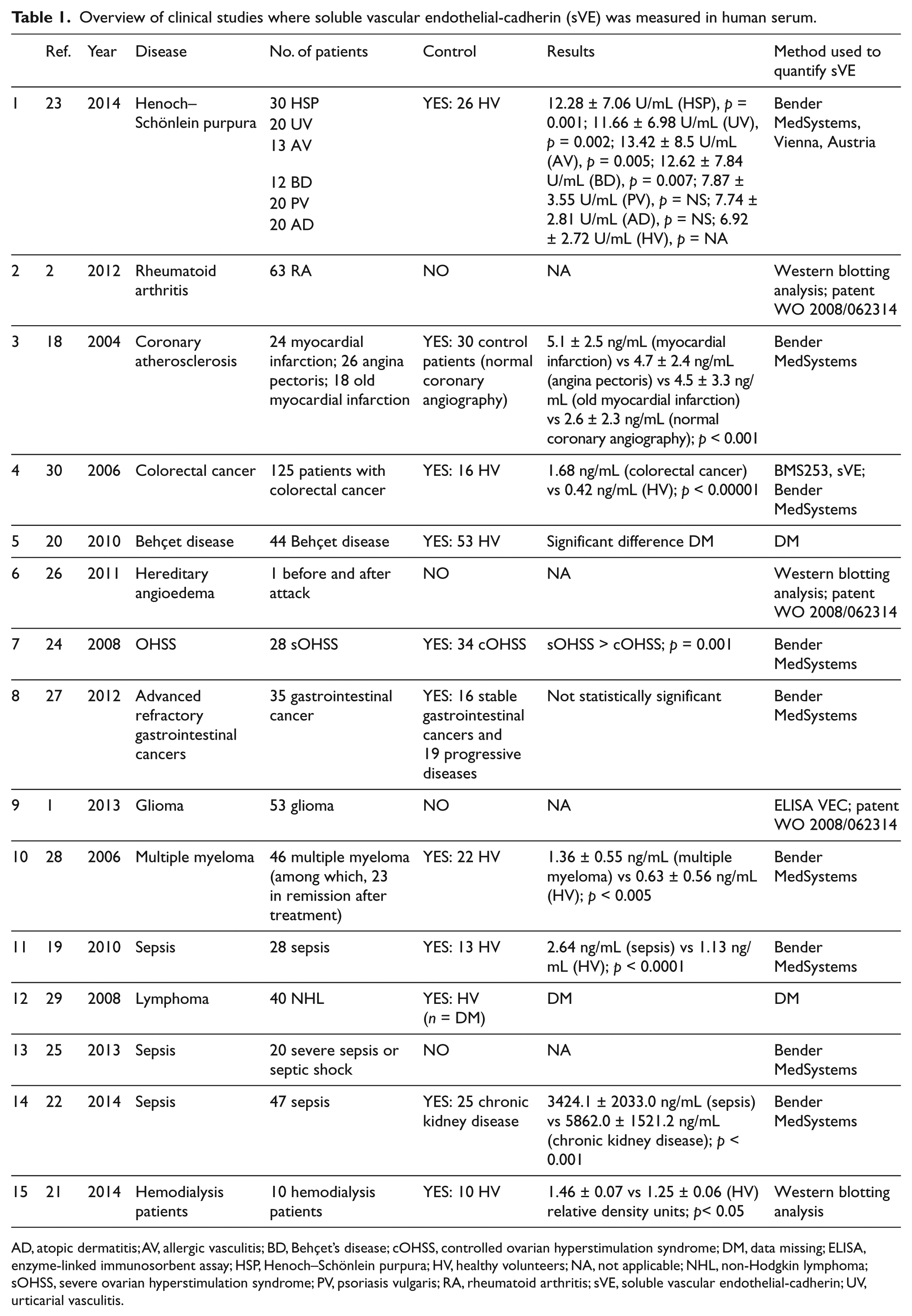
AD, atopic dermatitis; AV, allergic vasculitis; BD, Behçet’s disease; cOHSS, controlled ovarian hyperstimulation syndrome; DM, data missing; ELISA, enzyme-linked immunosorbent assay; HSP, Henoch–Schönlein purpura; HV, healthy volunteers; NA, not applicable; NHL, non-Hodgkin lymphoma; sOHSS, severe ovarian hyperstimulation syndrome; PV, psoriasis vulgaris; RA, rheumatoid arthritis; sVE, soluble vascular endothelial-cadherin; UV, urticarial vasculitis.
sVE, a marker of atherosclerosis?
The first clinical study assessing sVE levels was published in 2004 and covered patients with coronary atherosclerosis. 18 Three groups of patients were studied: a group with acute myocardial infarction (n=24), a group with angina pectoris (n=26), and a group with old myocardial infarction (n=18). Results of these three groups of patients were compared to those of a control group showing no signs of coronary artery stenosis on angiography (n=30). This study, led by a cardiology team, provided several vascular risk factors associated with the disease for each group, including gender, age, history of smoking, hypertension, diabetes mellitus, HDL-cholesterol and triglyceride levels. These parameters were similar for all groups, with no significant statistical difference found between them. The results demonstrated an increased level of sVE in the three groups of patients compared to the control group, yet no differences in sVE levels between the three groups of patients were found. The authors concluded that a high concentration of sVE was associated with coronary atherosclerosis, and that sVE was therefore a useful indicator of this disease rather than a result of its activity. Despite this interesting outcome, no further studies have been conducted to confirm these first observations. Studies investigating other diseases2,19,20 did not draw enough attention to the different vascular risk factors in the populations being studied (Figure 2).
sVE, a marker of inflammation?
Inflammation is generally associated with increased vascular permeability and a major characteristic of several diseases such as RA. sVE has been assayed in patients with various forms of systemic vasculitis like RA, Behçet’s disease (BD), Henoch–Schönlein purpura (HSP), as well as urticarial and allergic vasculitis. The studies retained here1,2,19,22 explored the hypothesis of sVE being a marker of disease activity. In HSP, for instance, serum sVE levels were significantly increased at the acute stage and correlated with disease severity (Figure 2). 23 Yet, in patients with inflammatory skin diseases like psoriasis vulgaris (PV) and atopic dermatitis (AD), 23 sVE levels were not increased when compared to healthy donor ones (n=26). Altogether, it might be hypothesized that in inflammatory disease, sVE might be a useful marker of endothelial dysfunction. However, it should also be mentioned here that higher levels of sVE were found in other clinical conditions, such as severe ovarian hyperstimulation syndrome (OHSS), 24 making it difficult to conclude on sVE specificity as a disease follow-up marker.
sVE, a marker of sepsis?
A conclusion on sepsis is difficult to draw as the three studies retrieved reported contradictory results.19,22,25 In the most recent one, sVE levels in 47 patients with sepsis were significantly lower than those measured in control subjects (25 patients with chronic kidney disease without sepsis). 22 The authors of another study also reported reduced sVE levels in 20 patients with sepsis, but the results were not statistically significant. 25 Contrariwise, Zhang and colleagues found higher sVE levels in a population of patients with severe sepsis. 19 Such contradictory outcomes from the studies might well reflect an analytical problem with the employed quatitation assays, the range of sVE concentrations measure or the overall analytical robustness of the method, and/or the stability of sVE itself in serum. Owing to the small cohorts studied, and until other studies come to light to confirm these results, the value of these data remains limited by several factors: (1) the selected populations might be heterogenous, with the inclusion of only symptomatic patients and the exclusion of patients with milder forms of the disease in some studies; (2) several studies omitted results covering a control group;1,2,26 and (3) even in studies including a control group, that group was not necessarily composed of only ‘healthy patients’ (i.e. the possibility of unintentional inclusion of asymptomatic donors with a vascular risk factor cannot be ruled out).
More recently, a study by Cohen-Mazor et al. described a population with 10 hemodialysis patients (HD) and 10 control individuals pointing out higher sVE levels in the HD patients’ group. VEC cleavage, which might lead to endothelium dysfunction in HD patients, was correlated with the presence of active elastase and cathepsin G, released from primed peripheral polymorphonuclear leukocytes. 21
sVE, a marker of malignant disease?
In vitro experiments have shown that VEGF-induced tyrosine phosphorylation of VEC on Y685 preceded cleavage of its extracellular adhesive domain. Since VEGF is the major mediator in several cancers, sVE could be detected in the serum of patients suffering from these diseases. Only a few papers have explored sVE in several types of human cancer, including myeloma, lymphoma, colorectal cancer, refractory gastrointestinal cancers and glioma1,27–30 (Figure 2). These recent studies take into account the fact that angiogenesis is often stimulated to promote the hypervascularity of tumors. Notably, tumor angiogenesis produces highly unusual blood vessels with structural abnormalities like heterogeneous distribution, tortuosity, dilation and inadequate perivascular cell (PVC) investment.
In patients diagnosed with multiple myeloma (MM), the role of angiogenesis in the pathogenesis and disease progression is well established. 28 Because elevated VEC RNA levels were found in patients with lymphoproliferative disorders, the authors hypothesized that sVE could be a reliable marker of angiogenic activity. In MM patients not receiving treatment, the sVE levels were found to be significantly higher than in healthy controls or even in MM patients who were in partial remission. 28 The sVE serum levels were not statistically different between MM patients in partial remission, after chemotherapy, and healthy subjects used as a control group. Albeit based on a relatively small group of patients, the results suggest that sVE might be helpful to assess the intensity of angiogenesis in MM, and therefore a useful noninvasive determination for prognosis and patients’ responsiveness to treatment. In non-Hodgkin lymphoma (NHL), serum sVE levels were assayed to determine their prognostic significance. 28 The results revealed that sVE levels significantly increased (p<0.05) in NHL patients (diffuse large cell lymphoma) compared to controls. 29 Higher levels of sVE were found in patients with stage II and III disease compared to stage IV, though the difference was not statistically significant. Low levels of sVE in stage IV disease could contribute to the invasiveness of the disease and metastasis formation, but no correlation with the overall survival rates was found.
To determine its role in colorectal cancer, sVE levels were measured in control subjects (healthy donors, n=16) and in sera from patients, collected preoperatively (n=125). 30 sVE levels were fourfold higher in patients’ sera than in the controls. In patients with advanced metastatic gastrointestinal cancers, mainly metastatic colorectal carcinoma, for whom standard therapies had failed, a series of pharmacodynamic and pharmacokinetic analyses were performed to determine the potential of sVE to act as a possible pharmacokinetic/pharmacodynamic marker of response to a new therapy. 27 After starting the metronomic schedule, sVE levels tend to be higher in patients with progressive disease (n=19) when compared to the levels found in patients with stable disease (n=16). While the difference was not statistically significant, it suggests a possible relationship between sVE levels and treatment efficacy. In these four clinical studies, increased sVE levels were found in cancer patients compared to healthy donors, possibly indicating tumor-related angiogenesis. Our group also reported a study where sVE was dosed in oncologic patients suffering of brain tumors. 1 Interestingly, sVE was found in serum from 53 glioma patients, however, and, in contrast to other cancer studies, the analysis indicated that a low preoperative sVE level was associated with shorter progression-free survival. 1 Two hypotheses can be advanced to explain this singularity. First, in brain tumors, the presence or absence of significant perilesional edema is associated with aggressiveness of the tumor. Indeed, it has been shown that patients with small peritumoral edema had shorter survival times, with their tumors being characterized by more brain-invasive growth. 31 The highest serum levels of sVE were measured in patients with significant perilesional edema, which could cause extensive diffusion of sVE into the blood. Second, another hypothesis is the reported decreased expression of VEGF-receptor in the tumor capillary network of the most aggressive tumors, which do not respond to therapy. 32
Altogether, there is a major omission from these studies in cancer: the lack of prospective randomized trials to address the question of whether or not sVE quantification is of any benefit in terms of progression-free and overall survival of patients.
Can acute and chronic diseases regulate sVE expression differently?
Based on the published studies, the utility of sVE as a biomarker might well depend on the disease stage; it can be a marker of endothelial damage or a marker of inflammatory response, and it can also be useful to differentiate between acute and chronic phases. Acute, and generally reversible, disorganization of junctional VEC has been documented but chronic dissociation of VEC in endothelial junctions is not a reversible process. This has been observed as a consequence of several conditions: the constitutive presence of angiogenic and inflammatory stimuli; and mutations in the regulators of endothelial junction stability; down-regulation of VEC transcription and expression. In the Soeki et al. study, 18 the authors examined sVE in coronary artery disease because VEC had been shown to be expressed in endothelial cells from atherosclerotic lesions, and was associated with neovascularization. 18 In patients with acute myocardial infarction, plasma sVE concentrations were unchanged in the acute and chronic phases. The authors thus suggested that sVE could be used as a marker of atherosclerosis in atherosclerotic disease rather than an inflammatory marker. 18 Serum sVE levels were significantly increased in HSP patients at the acute stage. This might be an indicator of the overall severity of the disease or the result of an immuno-inflammatory response to factors that damage vessels’ endothelium. 23 A recent study reported quantitation of sVE in hereditary angioedema (HAE) patients, a heritable autosomal-dominant disease caused by C1 inhibitor deficiency as a result of mutations in the SERPING1 gene. 26 This C1 inhibitor deficiency in HAE patients leads to the activation of plasma proteolytic cascades with consequent generation of plasma kallikrein (KK) and kinins, with bradykinin (BK) being the predominant mediator of enhanced vascular permeability in HAE. The authors showed that BK and KK induced VEC phosphorylation and cleavage when applied on an endothelial monolayer. What is more, sVE analysis in HAE patients showed a specific profile during the acute phase suggesting that sVE might represent a biomarker of HAE attacks. 26
Even if some available data provided some hints, the exact correlation between acute and chronic VEC regulation and the clinical features of human vascular diseases remains unknown. 15 The phosphorylation of VEC on tyrosine residues is believed to weaken junctions, making them permeable, but this alone might not be sufficient to draft a conclusion as other molecular signals can also contribute to the weakening of the endothelial barrier, such as beta-catenin phosphorylation.16,33 One possible explanation could be tyrosine phosphorylation of VEC – as observed in several human vascular disorders – which might occur on different specific tyrosine residues, depending on the particular type of disease. This variable phosphorylation might or might not lead to the cleavage of the VEC extracellular domain. 1 In chronic inflammatory diseases, the sVE levels and their correlation to disease outcome might be difficult to interpret because the criteria to assess disease activity are not always clear cut. Also, an acute attack in a chronic disease or the chronic phase of it cannot be ruled out altogether, which makes interpretation of results rather stumbling.
Auto-antibodies to human VEC (AAVEs) are associated with autoimmune diseases and vascular disorders
Destabilization of endothelial cell–cell junctions can be induced in vitro by targeting VEC using specific antibodies directed against its extracellular domain. 34 Thus, exposure of an endothelial cell monolayer to these antibodies in vitro decreases the adhesive function of VEC resulting in the monolayer dissociation and enhanced vascular permeability. 35 And, in vivo, the effect of these antibodies appeared to be much stronger than the effect of other antibodies against several other adhesion molecules located at the endothelial cell interfaces. 4 Antibodies directed against the extracellular domain of VEC were shown to increase vascular permeability, while decreasing tumor growth and metastasis were observed.36,37 In embryonic day 7.5 (E7.5) mouse embryos, intracardial injection of VEC antibodies, but not control antibodies, causes abnormal remodeling of the vasculature, confirming that VEC is essential for vascular integrity and expansion/angiogenesis. 4 A recent study reported a method to identify AAVEs in human serum from patients with several autoimmune diseases 35 such as RA (n=23), systemic lupus erythematosus (SLE, n=31), systemic sclerosis (n=30), and BD (n=16). Levels of these antibodies in patients’ sera were compared to levels measured in the ones withdrawn from a group of healthy donors (n=75), obtained from the French Blood Service, showing a significantly higher level in RA (p<0.0001), SLE (p<0.05) and BD (p<0.05) populations. Further characterization of the epitopes recognized by AAVEs showed that BD patients had specific antibodies against the EC3 and EC4 domains, whereas SLE patients’ antibodies preferentially recognized the EC1 fragment. The authors suggested that distinct epitopes of human VEC might explain the differences between distinct autoimmune diseases. In cancer, and because tumors are now widely accepted to be immunogenic, it will be interesting to analyse the AAVEs and epitope recognition profile. The pathogenesis of these AAVEs might be of clinical interest, with further prospective clinical studies needed to confirm this hypothesis and to provide evidence of a specific AAVE signature associated with vascular disorders in autoimmune diseases. Determining the physiological role played by AAVEs is still a scientific challenge but their presence is already considered to be a useful indicator of disease, at least in the case of RA. Further studies are needed to understand the pathological meaning of the presence of AAVEs in autoimmune diseases. These antibodies can be any one or a combination of: (a) disease-specific; (b) a response to a vascular disorder; (c) consistent with a general inflammatory condition; or (d) a potential biomarker for assessing responsiveness to treatment.
Quantification methods of sVE and AAVEs
Three quantitation methods for sVE and AAVEs were found in the published literature screened for this review. There were two reported enzyme-linked immunosorbent assays (ELISA) for sVE – the first being the kit provided by Bender MedSystems, Vienna, Austria (now eBioscience, Inc., San Diego, USA). All the authors claimed to have performed the ELISA according to the manufacturer’s instructions. The coefficients of variation were around 4.1% (intra-assay) and 7.2% (inter-assay). 18 The second ELISA has been previously described by the patent WO 2008/062314 and additionally summarized in detail by the authors. 1 The coefficients of variation were around 4.5% (intra-assay) and 13.7% (inter-assay) (data not published). The third quantitation method is based on western blotting. Several analytical differences and performance robustness between the employed quantitation methods could be discussed. The affinity and sensitivity of the captured anti-VEC antibody used in the two ELISA methods were not necessarily the same. And in the second ELISA method, the addition of detergent seems to improve the detection by boosting the interaction between the antibody anti-VEC and VEC protein. Consequently, the testing with the second ELISA made use of a 1:100 dilution of blood serum whereas the first ELISA kit used 100 µl of undiluted blood sera, as per the manufacturer’s instructions.
In both ELISA tests, a standard VEC was used to establish a range and normalize the reported results. This standard, however, was not necessarily the same in both tests; an extracellular domain called VE-cad 1-4 was used in both whereas the glycosylated form was only present in the second test.
From all the exposed and perhaps other unforeseen bias arising from incomplete descriptions of the reagents used in the manufacturer’s test, the obtained results are quite difficult to compare amid the different series of studies. The sVE level measured with the manufacturer’s ELISA test seems to be less than 1 ng/mL, 18 while the other ELISA expected a quantitation level between 500 and 700 ng/mL, taking into account the difference in the dilution of the blood samples. 2 To the best of our knowledge, the two methods do not seem to evaluate the same portion of sVE, and the glycosylated portion of sVE should be included by adding a detergent, owing to a sVE-cadherin–lipids interaction in circulating human blood (manuscript in preparation). This could explain the possible bias with some treatments alongside the testing conditions to determine the dose. Nowhere were we able to find the precise conditions used for patients’ sampling (‘fasting or not’ with the possibility of some interference with the lipid or the requirement to use a detergent). The best option should be a confirmation method using a second method such as western blotting, as in the publication where an ELISA was developed to capture auto-antibodies, using a recombinant human VEC fragment covering the extracellular domains as the target antigen. 35 The specificity of the AAVEs for the target antigen was then confirmed by western blotting, and basal AAVE levels could be determined for healthy donors (n=75). The coefficients of variation were less than 6% intra-assay and less than 15% inter-assay.
Soluble VEC and other methods to evaluate the vascular endothelial dysfunction
Despite today’s good level of understanding of the molecular mechanisms regulating VEC function in the endothelial barrier, questions remain open on how these functions are modulated and how they are involved in human physiology and pathology. For the diseases mentioned in this review, we are unable to conclude whether it is the cleavage of VEC, and the subsequent junction destabilization that is pathophysiological relevant, or if sVE has a particular function on its own. In several diseases linked to altered endothelial permeability and vascular organization, structural alterations in endothelial junction organization are described, but for most of them – systemic scleroderma, hemangiomas, or ischemic stroke – sVE and AAVEs have yet to be explored. Hence, it will be important to investigate how sVE levels change in several physiological situations (such as aging, stress, food intake, sport, cardiovascular risk) to further determine whether or not sVE represents a potential marker for atherosclerosis or chronic inflammation.
Methodologies for assessing the central role of the endothelium throughout several diseases led to the development of several methods to test different aspects of its function, which include measures of endothelial injury but also repairing. These studies provided not only novel insights into pathophysiology but also a clinical opportunity to gauge early disease status, quantify risk, judge response to interventions designed to prevent progression of early disease, and reduce later adverse events in patients. Endothelial function testing, such as arterial stiffness, shows great potential for development; the currently available tests are still too expensive and somehow difficult to interpret, making them unfit for routine clinical use. Flow-mediated dilation (FMD) of the brachial artery by ultrasounds is the most widely used noninvasive vascular test to assess endothelium-dependent vasodilation. It is probably the most reproducible test when an appropriate methodology is applied.38,39 FMD and reactive hyperemia peripheral arterial tonometry (RH-PAT), another non-invasive tool, are independent predictors of cardiovascular events and all-cause mortality according to a systematic review of 32 human studies. 40 Even if these tests are non-invasive, and allowing for repeated measurements, the optimal methodology to investigate different aspects of endothelial dysfunction is still under debate. FMD is a more sensitive method than RH-PAT in evaluating the effect of classical atherosclerotic risk factors on vascular endothelial function, 41 but technical difficulties, such as inter-laboratory calibration, are limiting its widespread clinical use.
The ability to measure endothelial function noninvasively might transform today’s understanding of the evolution of associated vascular diseases, but future large-scale clinical trials are required to demonstrate the real clinical interest of these biomarkers and ensure reproducibility of results between laboratories. So far, no correlative data exist between sVE and AAVE and other endothelium markers such as Von Willebrand factor, endothelial progenitor cells (EPC) or endothelial microparticles (EMP). 42
Conclusion
In conclusion, sVE and AAVEs are promising new biomarkers of vascular stress and endothelial dysfunction for a large range of diseases and disease stages. New clinical studies are necessary to determine the clinical and biological parameters required for further validation of these biomarkers in a clinical setting.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the patient association, ASF (‘Association des Sclérodermiques de France’) with the grant ‘bourse ASF jeune chercheur’ given to Sophie Blaise, and by the association GFRS (‘Groupe Francophone de Recherche sur la Sclérodermie’). Helena Polena received grants from the ARC Foundation (French Association against Cancer).