
Abstract

Keywords
1. Introduction
1.1. Document development process
1.1.1. Writing committee organization
The writing committee was selected to represent the American College of Cardiology (ACC), Society for Vascular Medicine (SVM), American Board of Internal Medicine (ABIM), and American Board of Vascular Medicine (ABVM), and included a cardiovascular training program director, a vascular medicine program training director, early-career vascular medicine experts, and highly experienced specialists representing both the academic and community-based practice settings. The committee also included physicians experienced in defining and applying training standards according to the 6 general competency domains promulgated by the Accreditation Council for Graduate Medical Education (ACGME) and American Board of Medical Specialties (ABMS) and endorsed by the ABIM. The ACC determined that relationships with industry or other entities were not relevant to the creation of this general cardiovascular training statement. Employment and affiliation details for authors and peer reviewers are provided in Appendixes 1 and 2, respectively, along with disclosure reporting categories. Comprehensive disclosure information for all authors, including relationships with industry and other entities, is available as an online supplement to this document.
1.1.2. Document development and approval
The writing committee developed the document, approved it for review by individuals selected by the ACC and SVM, and then addressed the peer reviewers’ comments. The document was revised and posted for public comment from December 20, 2014, to January 6, 2015. Authors addressed the additional comments from the public to complete the document. The final document was approved by the Task Force, COCATS Steering Committee, and ACC Competency Management Committee; ratified by the ACC Board of Trustees in March, 2015; and endorsed by the SVM. This document is considered current until the ACC Competency Management Committee revises or withdraws it.
1.2. Background and scope
Cardiovascular physicians frequently encounter patients with peripheral vascular diseases. Atherothrombosis, in particular, is a systemic disorder with clinical manifestations in the peripheral circulation. These and other vascular diseases account for substantial cardiovascular morbidity and mortality. Moreover, technological advances in imaging techniques and endovascular therapies have brought the management of vascular diseases firmly into the sphere of the cardiovascular medicine specialist. As part of a broader effort to standardize training criteria for all aspects of cardiovascular medicine, this Task Force was charged with updating previouslypublished adult vascular medicine training guidelines1,2 on the basis of changes in the field since 2008. One modification presented by this update is the transfer of the training recommendations on catheter-based peripheral vascular interventions to the COCATS 4 Task Force 10 report, thus integrating the recommendations with other cardiovascular interventional training components. The Task Force also updated previously published standards to address the evolving framework of competency-based medical education described by the ACGME Outcomes Project and by the 6 general competencies endorsed by the ACGME and ABMS. The background and overarching principles governing fellowship training are provided in the COCATS 4 Introduction, and readers should become familiar with this foundation before considering the details of training in a subdiscipline like vascular medicine. The Steering Committee and Task Force recognize that implementation of these changes in training requirements will occur incrementally.
For most areas of cardiovascular medicine, 3 levels of training are delineated:
The knowledge and competencies recommended at each level of training are based on published guidelines, competency statements, and the experience and opinions of the writing group. It is assumed that training is directed by appropriately trained mentors and that satisfactory completion of training is documented by the program director. The milestones required for each level of training are summarized in Section 4.
2. General standards
The ACC and the SVM have addressed training requirements and guidelines for vascular medicine training.1,2 The recommendations are congruent and address faculty, facility requirements, emerging technologies, and clinical practice. We strongly recommend that candidates for the ABIM examination for certification in cardiovascular diseases, as well as those seeking certification from the ABVM, review the specific examination requirements. 3 Cardiovascular fellowship programs should satisfy the requirements regarding faculty and facilities for training in vascular medicine.1,2 The intensity of training and required resources vary according to the level of training provided.
2.1. Faculty and facilities
2.1.1. Faculty
Trainees should be exposed to individuals with special training in vascular medicine. In some institutions, leadership of the vascular medicine component of training will come from vascular medicine specialists. In other programs, training in vascular medicine will be guided by faculty in other disciplines such as general cardiology, hematology, neurology, vascular surgery, and vascular or interventional radiology. All faculty members responsible for training fellows in vascular medicine should be board certified or board eligible in their subspecialties.
Ideally, faculty will include individuals certified in vascular medicine by the ABVM. Recognizing that this may not be possible at all institutions, cardiovascular fellows may spend time in other departments or divisions to gain the expertise necessary to interpret noninvasive vascular studies and to evaluate and manage patients with vascular disease. Faculty with expertise in disciplines relevant to vascular medicine, such as vascular surgery, vascular radiology, hematology, neurology, dermatology, and rheumatology, play important roles in training cardiovascular fellows. Faculty should provide didactic and practical education to fellows and deliver appropriate feedback about the performance of trainees.
2.2. Facilities
The training institution should provide comprehensive facilities for the care of patients with vascular disease and include offices for outpatient evaluation and treatment, inpatient vascular consultative services, a noninvasive vascular laboratory accredited by the Intersocietal Accreditation Commission (Intersocietal Accreditation Commission Vascular Testing Division, formerly Intersocietal Commission for the Accreditation of Vascular Laboratories), 4 facilities for computed tomographic angiography and magnetic resonance angiography, a peripheral vascular catheterization laboratory, and comprehensive vascular surgery and wound care programs.
2.3. Equipment
Noninvasive vascular laboratories require dedicated equipment to perform diagnostic studies, including duplex ultrasound units capable of high-resolution B-mode (grayscale) imaging as well as color and spectral Doppler analysis, equipment for physiological testing with appropriately sized cuffs to measure blood pressure at multiple sites in the limbs, Doppler and plethysmographic devices (e.g. pulse volume recordings, photoplethysmographic sensors), and equipment for digital image recording and archiving. Equipment required for cardiovascular computed tomography, cardiovascular magnetic resonance, and catheter-based angiography is discussed in the COCATS 4 Task Force 7, 8, and 10 reports, respectively.
2.4. Ancillary support
Ancillary support should be available to facilitate appointment scheduling and follow-up; manage clinical and financial records; retrieve laboratory and other clinical reports; enable telephone communications between patients and providers (e-mailing optional); provide clean, prepared examination and consultation rooms; and properly contain, control, and remove medical waste.
3. Training components
3.1. Didactic program
3.1.1. Lectures and conferences
Conferences for Level I training in vascular medicine for cardiovascular fellows should include case presentations and formal lectures that review diagnostic and therapeutic approaches to vascular diseases. Case presentations should illustrate the use of clinical tools, including noninvasive laboratory testing, magnetic resonance, computed tomographic and catheter-based angiography, and therapeutic approaches for patients with vascular diseases. Lectures should provide information regarding vascular anatomy, pathobiology, and pathophysiology; epidemiology and the natural history of peripheral vascular disorders; diagnostic evaluation; perioperative evaluation and management; and therapeutic options, including the risks and benefits of medical, endovascular, and surgical approaches to vascular disease to complement teaching in the clinic and at the bedside.
In addition to the lectures and case presentations described in the previous text for Level I trainees, didactic activities for Level II and III trainees should include a comprehensive longitudinal conference series on vascular topics, including peripheral artery disease; renal artery stenosis; mesenteric vascular disease and extracranial cerebrovascular disease; aneurysmal disease of the aorta and peripheral arteries; vasculitis; vasospastic and temperature-related diseases; venous thromboembolism; chronic venous insufficiency and varicose veins; lymphedema; less-common disorders such as fibromuscular dysplasia and arteriopathies associated with inherited diseases of connective tissue; congenital vascular malformations and arterial entrapment syndromes; leg ulcers; and the preoperative evaluation and perioperative management of patients undergoing vascular surgery. Conferences should also cover the noninvasive vascular laboratory, including principles of vascular physiology, vascular ultrasound imaging and Doppler flow velocity measurements, ultrasound physics, blood pressure measurement and pulse volume recordings, transducer technology, imaging artifacts, and reviews of the noninvasive evaluation of specific vascular diseases. Lectures and case presentations should cover other vascular imaging modalities such as magnetic resonance, computed tomographic, and catheter-based angiography. The lecture series should include regularly scheduled patient safety or quality improvement conferences, journal clubs, or other fora for interactive discussion of the established literature and emerging scientific advances. Interaction with vascular specialists from other disciplines at these conferences is recommended.
3.2. Clinical experience
Level I trainees should gain experience in vascular disease management in both the inpatient and outpatient settings, assisting in patient care in a manner that provides patientcentered education. It is important that Level I trainees evaluate and manage patients with arterial, venous, and lymphatic disorders. Training in vascular medicine may occur either in dedicated rotations or throughout the cardiovascular clinical training period. During the course of patient-based rotations, Level I trainees should encounter and receive instruction in the bedside evaluation of patients with peripheral (limb) artery disease, renal and mesenteric artery disease, extracranial carotid artery disease, thoracic and abdominal aortic aneurysms, acute aortic syndromes, deep vein thrombosis, pulmonary embolism, and chronic venous insufficiency. Program activity should include appropriate use of vascular diagnostic modalities (physiological testing; duplex ultrasound imaging; and magnetic resonance, computed tomographic, and catheter-based angiography); indications for and use of pharmacotherapy to prevent and treat atherosclerosis, venous thromboembolism, and their risk factors; the role of endovascular and surgical revascularization; assessment of cardiovascular risk; and periprocedural/perioperative management of patients undergoing endovascular procedures and vascular surgery.
Level II training for a cardiovascular specialist concentrating in vascular medicine should include the evaluation and management of patients with vascular disease in both the outpatient clinic and the hospital, extending the skills acquired during Level I training. Level II training must include performance and interpretation of noninvasive vascular tests. Trainees should understand physiological and ultrasound vascular testing and should perform and interpret segmental pressure measurements, pulse volume recordings, and duplex ultrasonography for venous thrombosis, venous insufficiency, peripheral artery disease, abdominal aortic aneurysm, renal and mesenteric artery disease, and carotid artery disease.
Level III training in vascular medicine should provide the knowledge and skills to function as a vascular specialist, including the ability to interpret patients’ clinical presentation, plan diagnostic testing, apply clinical and laboratory information, and develop appropriate management plans for patients across the entire range of vascular diseases, including but not limited to peripheral artery disease, renal artery disease, mesenteric vascular disease, extracranial cerebrovascular disease, aneurysmal disease of the aorta and peripheral arteries, vasculitis, venous thromboembolism, chronic venous insufficiency, varicose veins, lymphedema, leg ulcers, and Raynaud’s phenomenon and other vasospastic and temperature-related disorders. Trainees should also acquire skills to evaluate patients before and after interventional peripheral vascular procedures.
3.3. Hands-on experience
Trainees should perform physical examinations and noninvasive vascular testing appropriate to their level of training. Level I trainees should be able perform a complete vascular examination and measure the ankle-brachial index using a hand-held Doppler device and should become familiar with the interpretation of vascular laboratory reports as they apply to the noninvasive assessment of obstructive arterial and venous thromboembolic diseases affecting the vessels of the lower extremities.
Level II and III trainees should independently perform and interpret arterial physiological studies of the limbs and vascular ultrasound examinations of the veins and arteries of the limbs, abdominal vessels, and extracranial carotid arteries. Additional experience in the vascular laboratory during Level III training may include transcranial Doppler examinations, treatment of femoral artery pseudoaneurysms with ultrasound-guided compression or thrombin injection, and ultrasound-guided treatment of varicose veins. Level III training may include training in wound care techniques, including debridement and application of appropriate dressings.
4. Summary of training requirements
4.1. Development and evaluation of core competencies
Training and requirements in vascular medicine address the 6 general competencies promulgated by the ACGME/ ABMS and endorsed by the ABIM. These competency domains are: medical knowledge, patient care and procedural skills, practice-based learning and improvement, systems-based practice, interpersonal and communication skills, and professionalism. The ACC has used this structure to define and depict the components of the core clinical competencies for cardiovascular medicine. The curricular milestones for each competency and domain also provide a developmental roadmap for fellows as they progress through various levels of training and serve as an underpinning for the ACGME/ABIM reporting milestones. The ACC has adopted this format for its competency and training statements, career milestones, lifelong learning, and educational programs. Additionally, it has developed tools to assist physicians in assessing, enhancing, and documenting these competencies.
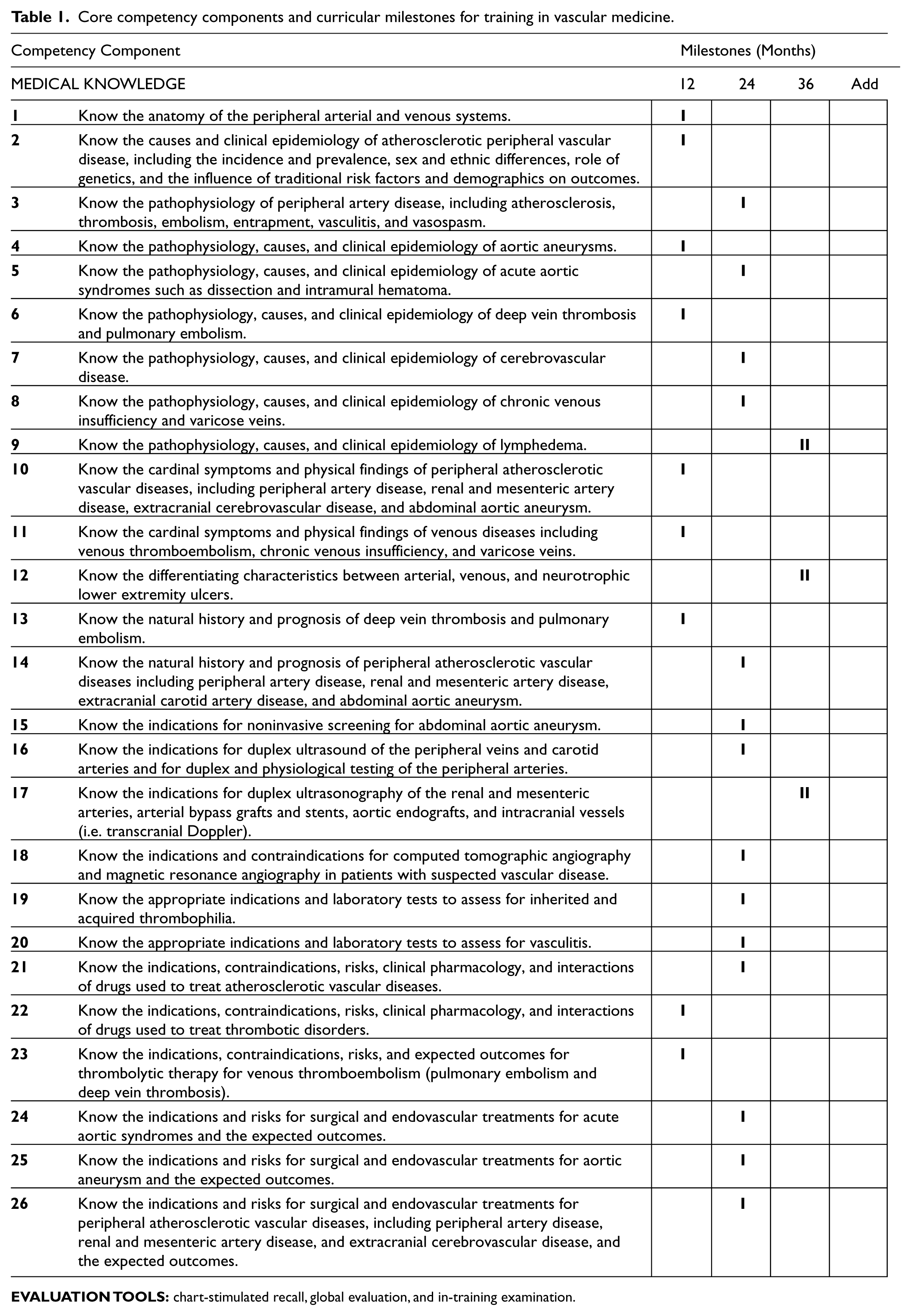
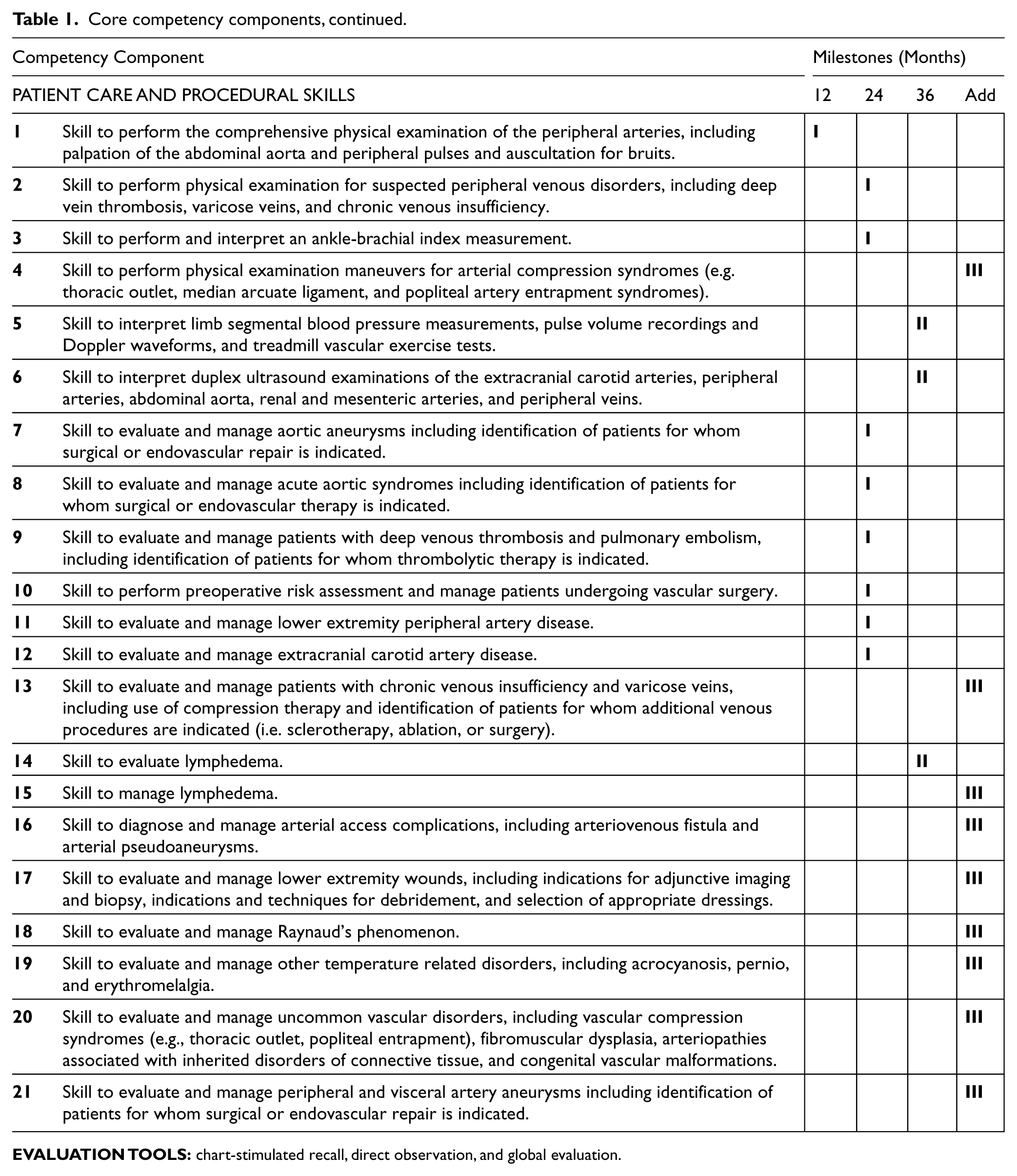
Table 1 delineates each of the 6 competency domains as well as their associated curricular milestones for training in vascular medicine. The milestones are categorized into Level I, II, and III training (as previously defined in this document) and indicate the stage of fellowship training (12, 24, or 36 months, and additional time points) by which the typical cardiovascular trainee should achieve the designated level. Given that programs may vary with respect to the sequence of clinical experiences provided to trainees, the milestones at which various competencies are reached may also vary. Level I competencies may be achieved at earlier or later time points. Acquisition of Level II skills requires additional training that may be completed during the standard 3-year cardiovascular fellowship. Level III skills require additional training in a dedicated advanced vascular medicine program after completion of the general cardiovascular fellowship. The table also describes examples of evaluation tools suitable for assessing competence in each domain.
Core competency components and curricular milestones for training in vascular medicine.
Core competency components, continued.
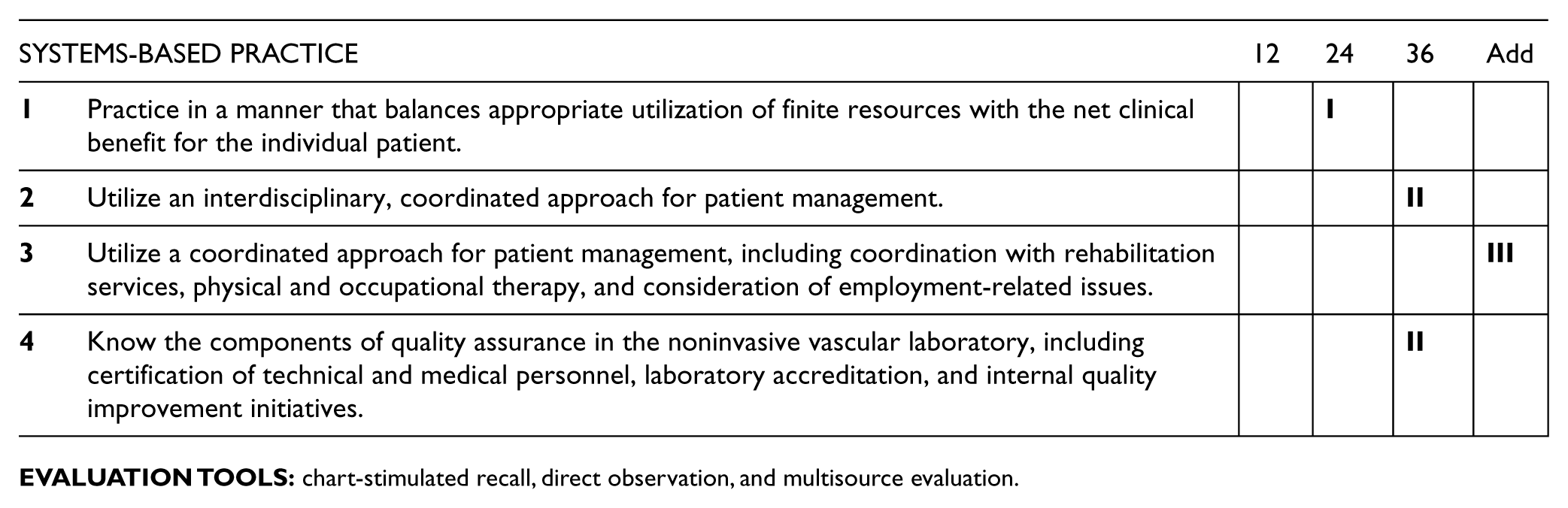
Core competency components, continued.
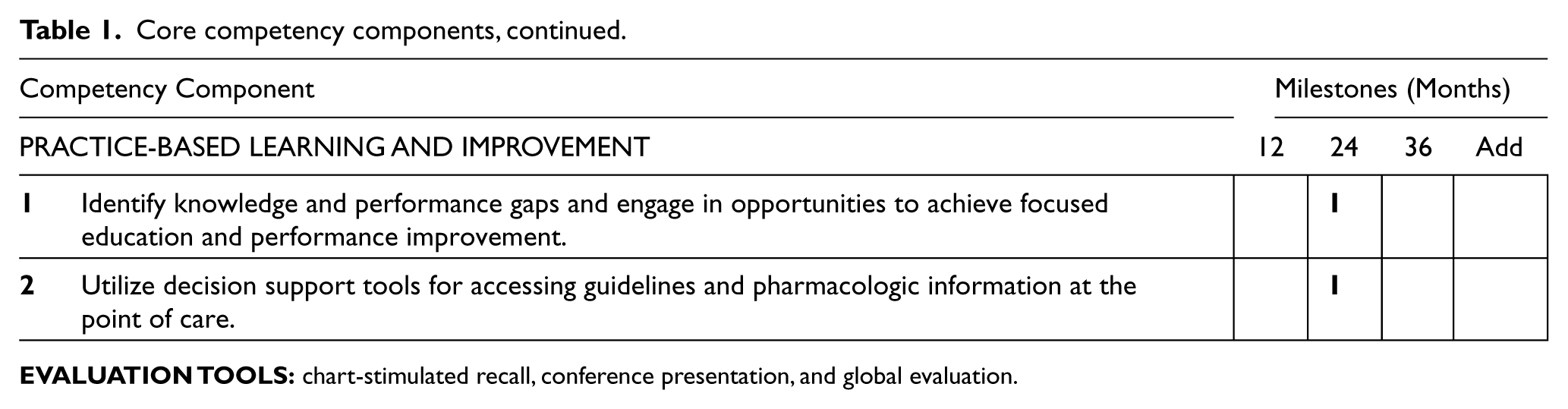
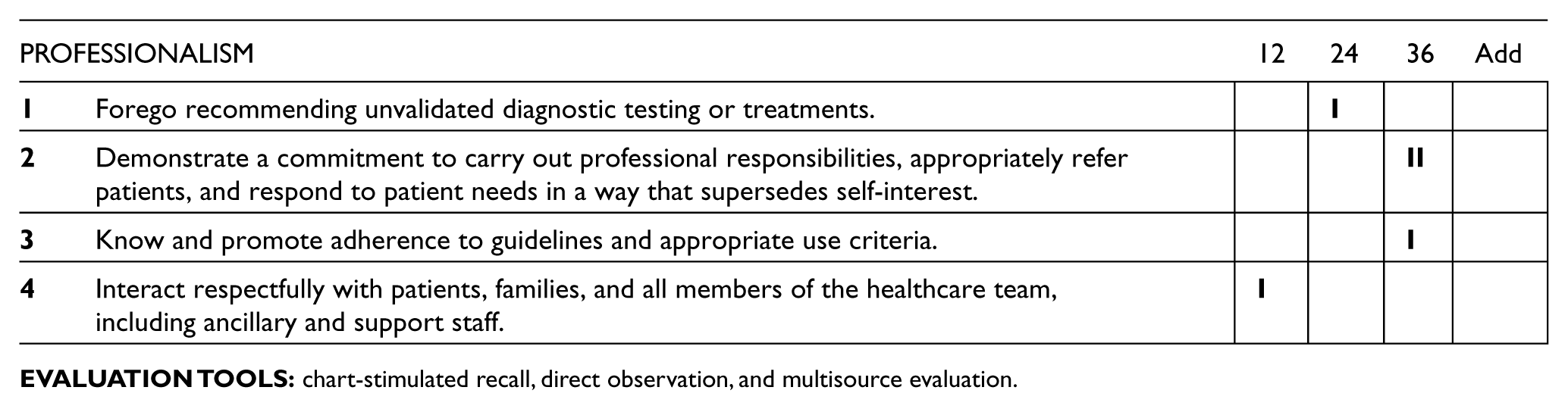
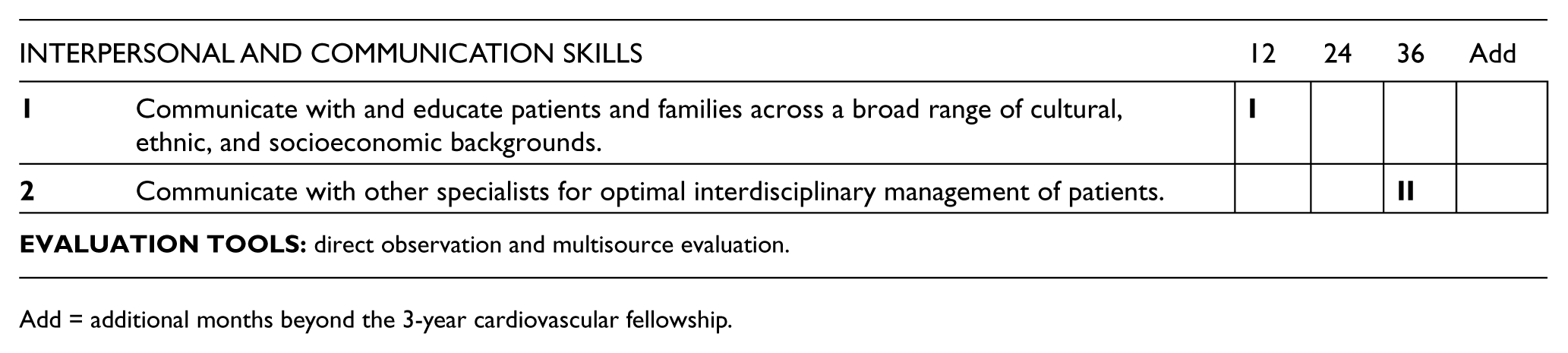
Add = additional months beyond the 3-year cardiovascular fellowship.
4.2. Duration and structure of training
Level I competencies must be obtained by all fellows during the 3-year cardiovascular disease fellowship training program. Level II competencies may be obtained by selected fellows during the cardiovascular disease fellowship depending on their career focus and elective experiences. Level III competencies are noted as additional requirements for advanced training beyond the standard 3-year fellowship. The duration and structure of training required for the typical fellow to gain competencies in Levels I, II, and III training in vascular medicine are summarized in the following text. In all cases, achievement of the competencies must be assessed.
4.2.1. Level I training requirements
Level I training typically requires 2 months of exposure to vascular medicine services, either as dedicated rotations or in aggregate, to provide the knowledge, skills, and attitudes required for diagnosis and management of patients with vascular diseases (Table 1). Training should focus on the value of the clinical history and examination for diagnosis, and exposure to bedside testing, vascular physiologic testing, duplex ultrasound imaging, and other noninvasive angiographic imaging modalities (computed tomographic and magnetic resonance angiography). The curriculum should include testing methods, indications, diagnostic criteria, and technical limitations. Level I trainees should understand the advantages and disadvantages of the various vascular testing modalities for specific clinical conditions. Sufficient exposure to catheter-based angiography and endovascular procedures should be provided to allow understanding of the roles of these modalities in diagnosis and management. The Level I trainee should understand basic concepts of surgical and endovascular treatments, including indications, contraindications, and potential complications. Level I trainees should also be instructed in the comprehensive evaluation of patients undergoing vascular surgery, including indications and risks of preoperative testing and management of perioperative cardiovascular problems and complications. They should learn to recognize and manage disorders associated with vascular diseases, including hypertension, hypercholesterolemia, and diabetes mellitus, throughout the cardiovascular fellowship and should know when it is appropriate to refer patients to a vascular specialist for further evaluation and intervention.
4.2.2. Level II training requirements
Level I training in vascular medicine is a prerequisite for Level II training. In addition to the 24 months of clinical training required for board eligibility in cardiovascular medicine, further training, typically during the third year, should enable the fellow to become more knowledgeable and skilled in vascular medicine and noninvasive vascular laboratory procedures.1,2 At completion of Level II training, the trainee should be able to perform and interpret noninvasive vascular diagnostic examinations. In addition to interpretation, hands-on experience and familiarity with scanning protocols are required. Completion of the vascular laboratory curriculum during Level II or III training should make the trainee eligible for the Physicians’ Vascular Interpretation Examination 5 and meet the requirements to serve as medical staff or medical director of an accredited vascular laboratory. Trainees seeking additional competency in vascular medicine during cardiovascular fellowship should participate in additional inpatient and outpatient vascular medicine consultations and noninvasive vascular laboratory activities, and should observe magnetic resonance, tomographic, and catheter-based angiography and interventions.
4.2.3. Level II and III noninvasive vascular laboratory training
Expertise in the noninvasive vascular laboratory is important for vascular medicine specialists and required for Level II and III trainees. The curriculum should include diagnostic testing procedures and equipment, indications, diagnostic criteria, and technical limitations. In addition to the curricular components, Level II and III trainees should have extensive mentored experience in interpreting vascular studies. The Physicians’ Vascular Interpretation Examination should be successfully completed after either Level II or III training. Interpretation under faculty supervision of at least 500 studies distributed across the vascular testing areas is a prerequisite for the Physicians’ Vascular Interpretation Examination. 5 These areas include duplex ultrasonography of limb veins, limb arteries (including bypass grafts and stents), carotid arteries, renal and mesenteric arteries, and the abdominal aorta; physiological testing for peripheral artery disease; and transcranial Doppler examination. The vascular laboratory curriculum for the Level III trainee should include laboratory quality and accreditation processes, a review of correlation studies, and participation in quality improvement activities, such as peer review and cross-modality correlation studies.
4.2.4. Level III training requirements
Level III training should provide trainees with the knowledge and skills to interpret the clinical presentation, plan diagnostic testing, apply clinical and laboratory information, and develop appropriate management plans for patients with a variety of vascular disorders as a vascular medicine specialist. This extends the knowledge and skills acquired during Level I training to the entire range of vascular diseases, as described in Sections 3.2 and 3.3 and outlined in Table 1, and includes performance and interpretation of noninvasive vascular diagnostic examinations, as described in Section 4.2.3.
Fellows planning careers as vascular medicine specialists require advanced training beyond the 24 months of clinical training required for board eligibility in cardiovascular medicine, typically during a 4th year dedicated to this field.1,2 Level I training in vascular medicine is a prerequisite for Level III training, and Level II training can be applied to Level III training, decreasing the time required to gain Level III competence. Level III training cannot be obtained during the standard 3-year cardiovascular fellowship and requires additional exposure in a program meeting requirements that will be addressed in a subsequent, separately published Advanced Training Statement (formerly Clinical Competence Statement).1,2 The Level III trainee is expected to pass the certification examination offered by the ABVM. 3 Fellows seeking training in peripheral vascular interventions should consult the COCATS 4 Task Force 10 report, which integrates peripheral endovascular intervention with other cardiovascular interventional training components.
5. Evaluation of competency
A key characteristic of the competency- and curricular milestone–based system is integration with outcomes-based evaluations. For training programs, evaluation tools include a variety of modalities, such as direct observation by instructors, in-training examinations, procedure logbooks, conference and case presentations, multisource evaluations, trainee portfolios, and simulation. Case management, judgment, and interpretive and technical skills must be evaluated in every trainee. An optimum training environment includes bidirectional evaluations in which faculty evaluate and provide positive or negative feedback to trainees, and trainees evaluate faculty after each rotation. The program director should review these evaluations with the trainee and faculty individually. Mechanisms should be incorporated so that the fellow who performs suboptimally can be counseled and further action can be taken if necessary.
Within a given clinical area, achievement of competence is expected for each of the specific Level I curricular milestones. It is not expected, however, that the training program formally evaluate each component (curricular milestone) individually. Rather, evaluation tools may focus on representative components in a given area. The program director should record each trainee’s experiences and performance of various patient care skills to document satisfactory achievement at each level of training. Trainees should maintain records of participation and advancement in the form of a Health Insurance Portability and Accountability Act (HIPAA)–compliant electronic database or logbook that meets ACGME reporting standards and summarizes pertinent clinical information (e.g. number of cases, diagnoses, disease severity, outcomes, and disposition). The program director is responsible for confirming the experience and competence of trainees. Under the aegis of the program director, the faculty should record each trainee’s experiences and assess performance to document satisfactory achievement. The fund of knowledge regarding vascular disease must be evaluated in every trainee. Quality of clinical skills; reliability; judgment; actions that result in complications; and interactions with other physicians, patients, and laboratory support staff are key components of the evaluation. Initiative and the ability to make independent and appropriate decisions should also be assessed. The program director and Clinical Competency Committee should specifically review the overall progress of individual trainees and achievement of selected training milestones and identify areas in which additional focused training is required.
Along with other professional organizations, including the SVM, the ACC has formulated a clinical competence statement on vascular medicine and catheter-based vascular interventions. 2 The SVM has defined the essential components of a specialized program for training in vascular medicine. 1 Self-assessment programs are available through the ACC. Training directors and trainees are encouraged to incorporate these resources in the course of training.
Evidence of competence can be ascertained by several certification examinations. The American Registry for Diagnostic Medical Sonography (ARDMS) offers a certifying examination for physicians performing and interpreting noninvasive vascular examinations (the Physicians’ Vascular Interpretation Examination) for individuals completing the noninvasive vascular laboratory prerequisites during Level II or III training. Information concerning the eligibility and prerequisites for this examination can be obtained from the American Registry for Diagnostic Medical Sonography. 5 The ABVM offers an examination for certification in vascular medicine for individuals completing Level III training. Information concerning eligibility requirements can be obtained from the ABVM. 3 Additional information regarding peripheral intervention is discussed in the COCATS 4 Task Force 10 report.
Footnotes
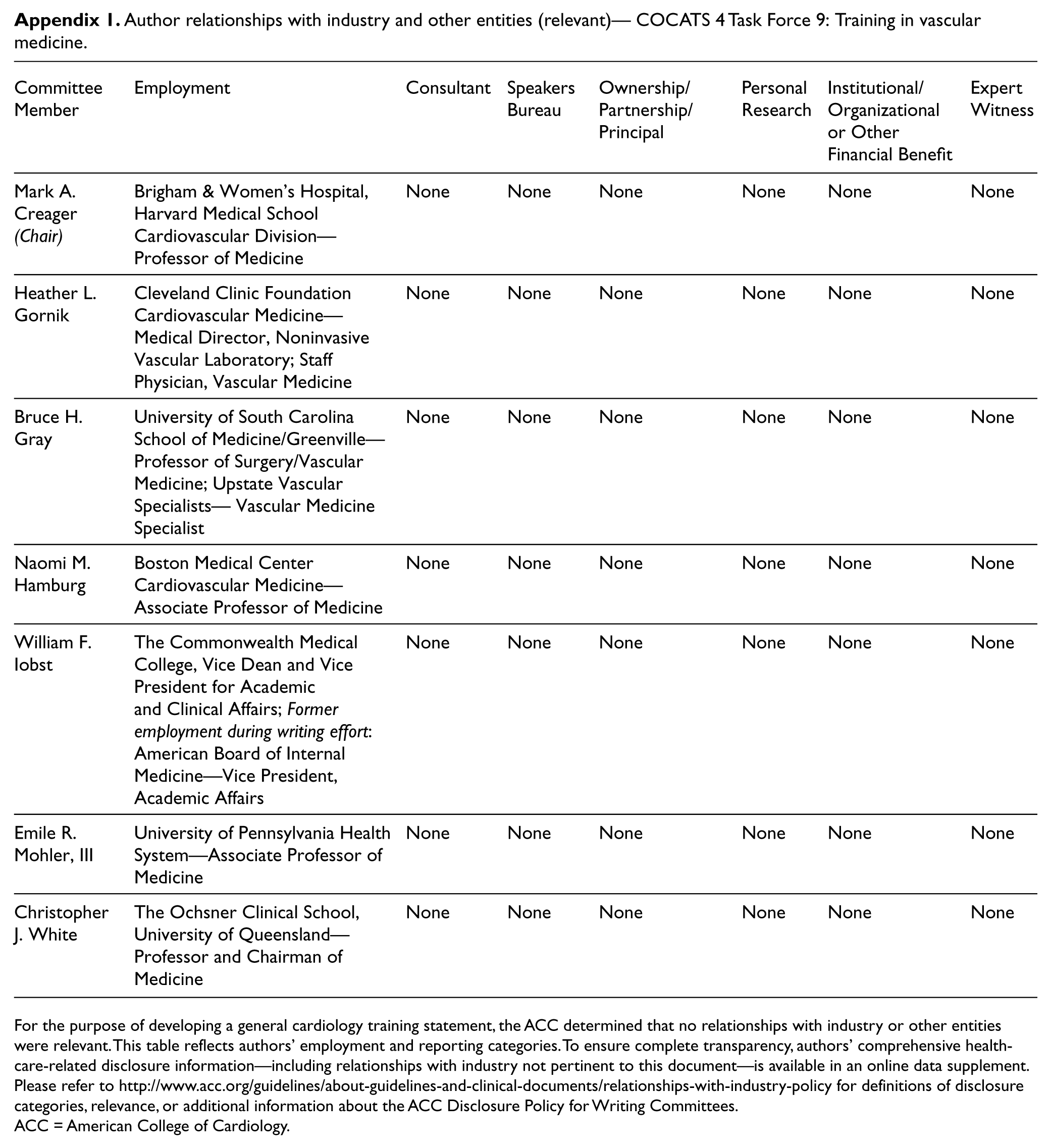
Appendix 1. Author relationships with industry and other entities (relevant)— COCATS 4 Task Force 9: Training in vascular medicine
| Committee Member | Employment | Consultant | Speakers Bureau | Ownership/ Partnership/ Principal | Personal Research | Institutional/ Organizational or Other Financial Benefit | Expert Witness |
|---|---|---|---|---|---|---|---|
| Mark A. Creager (Chair) | Brigham & Women’s Hospital, Harvard Medical School Cardiovascular Division—Professor of Medicine | None | None | None | None | None | None |
| Heather L. Gornik | Cleveland Clinic Foundation Cardiovascular Medicine—Medical Director, Noninvasive Vascular Laboratory; Staff Physician, Vascular Medicine | None | None | None | None | None | None |
| Bruce H. Gray | University of South Carolina School of Medicine/Greenville— Professor of Surgery/Vascular Medicine; Upstate Vascular Specialists— Vascular Medicine Specialist | None | None | None | None | None | None |
| Naomi M. Hamburg | Boston Medical Center Cardiovascular Medicine—Associate Professor of Medicine | None | None | None | None | None | None |
| William F. Iobst | The Commonwealth Medical College, Vice Dean and Vice President for Academic and Clinical Affairs; Former employment during writing effort: American Board of Internal Medicine—Vice President, Academic Affairs | None | None | None | None | None | None |
| Emile R. Mohler, III | University of Pennsylvania Health System—Associate Professor of Medicine | None | None | None | None | None | None |
| Christopher J. White | The Ochsner Clinical School, University of Queensland—Professor and Chairman of Medicine | None | None | None | None | None | None |
For the purpose of developing a general cardiology training statement, the ACC determined that no relationships with industry or other entities were relevant. This table reflects authors’ employment and reporting categories. To ensure complete transparency, authors’ comprehensive healthcare-related disclosure information—including relationships with industry not pertinent to this document—is available in an online data supplement. Please refer to http://www.acc.org/guidelines/about-guidelines-and-clinical-documents/relationships-with-industry-policy for definitions of disclosure categories, relevance, or additional information about the ACC Disclosure Policy for Writing Committees.
ACC = American College of Cardiology.
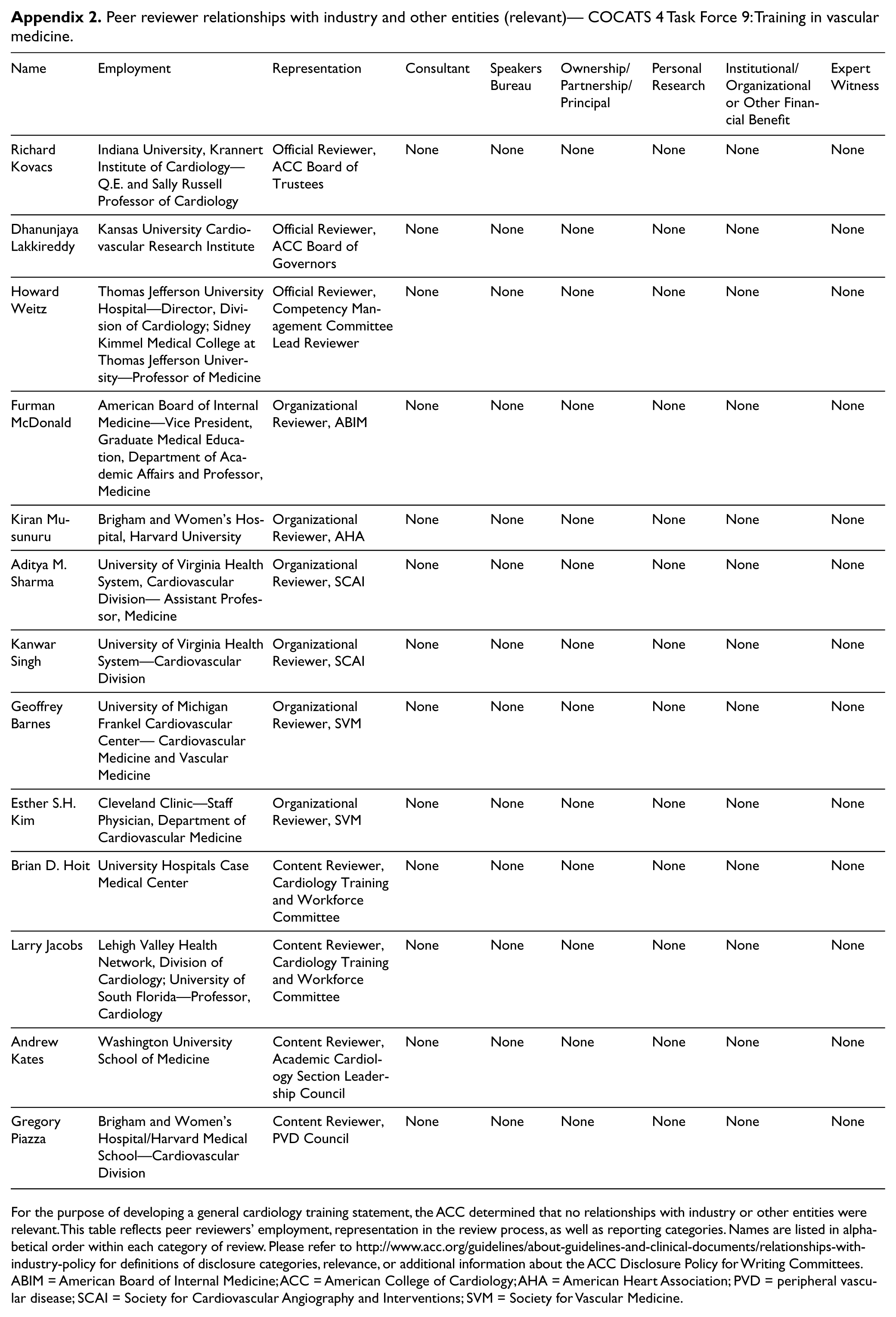
Appendix 2. Peer reviewer relationships with industry and other entities (relevant)— COCATS 4 Task Force 9: Training in vascular medicine
| Name | Employment | Representation | Consultant | Speakers Bureau | Ownership/ Partnership/ Principal | Personal Research | Institutional/ Organizational or Other Financial Benefit | Expert Witness |
|---|---|---|---|---|---|---|---|---|
| Richard Kovacs | Indiana University, Krannert Institute of Cardiology—Q.E. and Sally Russell Professor of Cardiology | Official Reviewer, ACC Board of Trustees | None | None | None | None | None | None |
| Dhanunjaya Lakkireddy | Kansas University Cardiovascular Research Institute | Official Reviewer, ACC Board of Governors | None | None | None | None | None | None |
| Howard Weitz | Thomas Jefferson University Hospital—Director, Division of Cardiology; Sidney Kimmel Medical College at Thomas Jefferson University—Professor of Medicine | Official Reviewer, Competency Management Committee Lead Reviewer | None | None | None | None | None | None |
| Furman McDonald | American Board of Internal Medicine—Vice President, Graduate Medical Education, Department of Academic Affairs and Professor, Medicine | Organizational Reviewer, ABIM | None | None | None | None | None | None |
| Kiran Musunuru | Brigham and Women’s Hospital, Harvard University | Organizational Reviewer, AHA | None | None | None | None | None | None |
| Aditya M. Sharma | University of Virginia Health System, Cardiovascular Division— Assistant Professor, Medicine | Organizational Reviewer, SCAI | None | None | None | None | None | None |
| Kanwar Singh | University of Virginia Health System—Cardiovascular Division | Organizational Reviewer, SCAI | None | None | None | None | None | None |
| Geoffrey Barnes | University of Michigan Frankel Cardiovascular Center— Cardiovascular Medicine and Vascular Medicine | Organizational Reviewer, SVM | None | None | None | None | None | None |
| Esther S.H. Kim | Cleveland Clinic—Staff Physician, Department of Cardiovascular Medicine | Organizational Reviewer, SVM | None | None | None | None | None | None |
| Brian D. Hoit | University Hospitals Case Medical Center | Content Reviewer, Cardiology Training and Workforce Committee | None | None | None | None | None | None |
| Larry Jacobs | Lehigh Valley Health Network, Division of Cardiology; University of South Florida—Professor, Cardiology | Content Reviewer, Cardiology Training and Workforce Committee | None | None | None | None | None | None |
| Andrew Kates | Washington University School of Medicine | Content Reviewer, Academic Cardiology Section Leadership Council | None | None | None | None | None | None |
| Gregory Piazza | Brigham and Women’s Hospital/Harvard Medical School—Cardiovascular Division | Content Reviewer, PVD Council | None | None | None | None | None | None |
For the purpose of developing a general cardiology training statement, the ACC determined that no relationships with industry or other entities were relevant. This table reflects peer reviewers’ employment, representation in the review process, as well as reporting categories. Names are listed in alphabetical order within each category of review. Please refer to http://www.acc.org/guidelines/about-guidelines-and-clinical-documents/relationships-with-industry-policy for definitions of disclosure categories, relevance, or additional information about the ACC Disclosure Policy for Writing Committees.
ABIM = American Board of Internal Medicine; ACC = American College of Cardiology; AHA = American Heart Association; PVD = peripheral vascular disease; SCAI = Society for Cardiovascular Angiography and Interventions; SVM = Society for Vascular Medicine.
Appendix 3. Abbreviation list
ABIM = American Board of Internal Medicine
ABMS = American Board of Medical Specialties
ABVM = American Board of Vascular Medicine
ACC = American College of Cardiology
ACGME = Accreditation Council for Graduate Medical Education
ARDMS = American Registry for Diagnostic Medical Sonography
COCATS = Core Cardiovascular Training Statement
HIPAA = Health Insurance Portability and Accountability Act
PVI = Physicians’ Vascular Interpretation
SVM = Society for Vascular Medicine