
Abstract

It is thought that lymphovenous communications may allow lymph to enter blood before the thoracic duct (TD). Whether this occurs physiologically 1 or in response to lymphatic dysfunction2,3 is unclear. These images of a 54-year-old man who initially presented with right-sided, painless, intermittent, pitting lower limb swelling support the existence of such communications. He was initially investigated with lymphoscintigraphy. Five years later, the swelling became bilateral and he underwent further lymphoscintigraphy. On both occasions, 20 MBq of Tc-99m-nanocolloid (General Electric, UK) was injected subcutaneously into the first web spaces of both feet, followed by gamma camera imaging immediately after injection (0 min) and at 45 and 150 minutes post injection. He undertook no strenuous exercise before completion of imaging. Anterior projections (Panels B and D) illustrate very heavy hepatic and splenic activity at 150 minutes in the first and second studies. There was no activity in the liver at 0 or 45 minutes in either study (anterior projections; Panels A and C), excluding intravascular injection as the origin of the hepatic activity. Accumulation of the activity in the right lymphatic system was delayed and reduced compared with the left, most apparent at 45 minutes. The left is also abnormal as shown by popliteal node visualisation (Panel D; arrow), indicating diversion of lymph into the deep lymphatic system. The 150-minute hepatic activity was quantified in relation to ilio-inguinal nodal activity on the anterior projections as the ratio of counts per pixel in a region of interest (ROI) over the right lobe of the liver to the total counts in ROIs encompassing both ilio-inguinal nodal groups. 3 The rationale underpinning this ratio is that if all tracer from the lower extremities ultimately entering the TD first passes through ilio-inguinal nodes, then the ratio would be approximately constant from patient to patient. However, the ratio in this patient’s second scan was 100 pixels-1x10-6; ~40-fold higher than in subjects with normal lymphatic function. 3 The ratio could not be quantified in the first scan because the only data available were saved in a format that could not be numerically analysed. However, from the imaging (Panel B), it can be seen that the value would have been broadly similar. From this study, the patient received a diagnosis of primary bilateral lower extremity lymphedema. When interpreting lymphoscintigraphy, finding excessive hepatic activity in delayed images, not present in the immediate image, should be regarded as suspicious for abnormal lymphatic function.
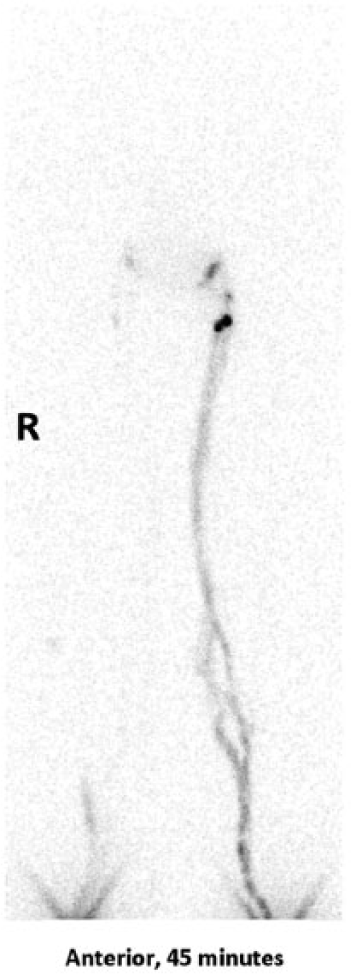
Anterior half-body lymphoscintigraphy acquired 45 minutes after injection of 20 MBq Tc-99m-nanocolloid into the first web spaces of both feet – first study. Note absence of hepatic activity.
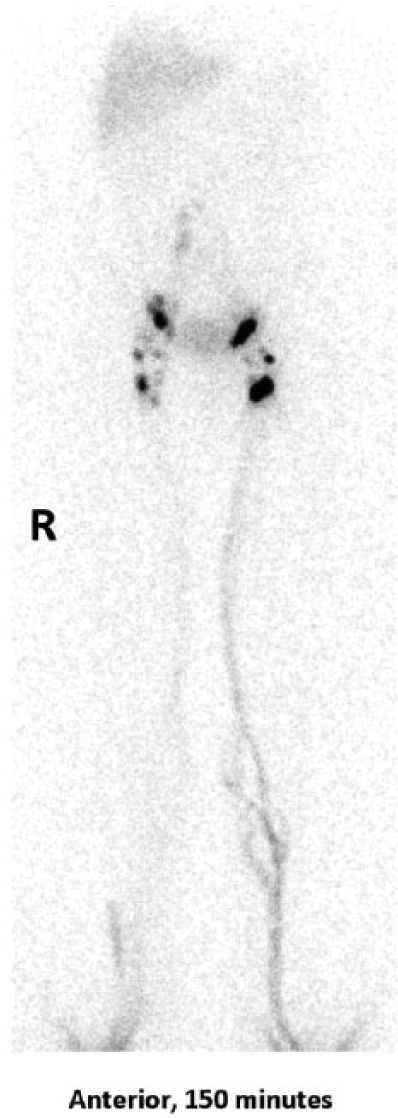
Anterior half-body lymphoscintigraphy acquired 150 minutes after injection of 20 MBq Tc-99m-nanocolloid into the first web spaces of both feet – first study.
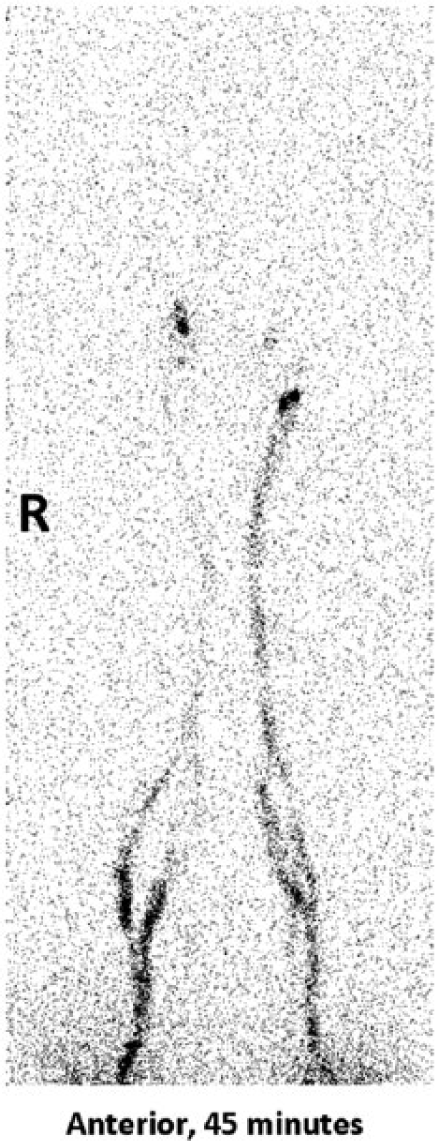
Anterior half-body lymphoscintigraphy acquired 45 minutes after injection of 20 MBq Tc-99m-nanocolloid into the first web spaces of both feet – follow-up study. Note absence of hepatic activity.
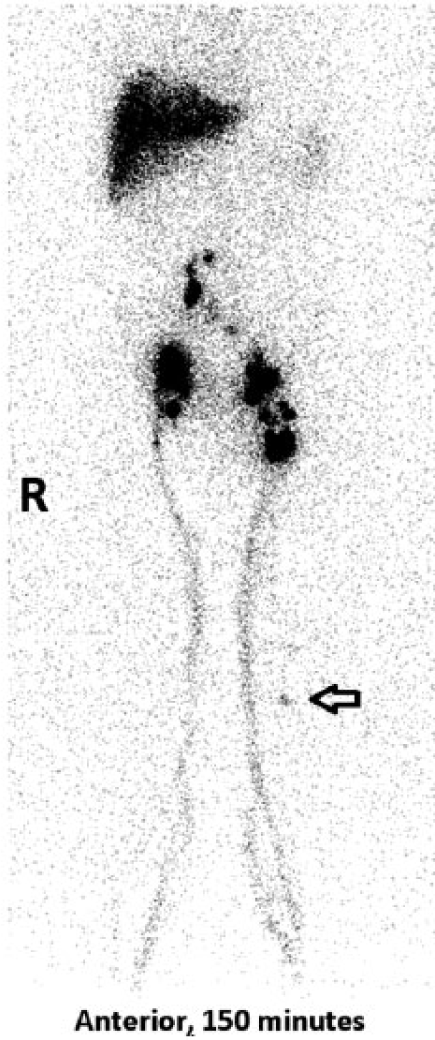
Anterior half-body lymphoscintigraphy acquired 150 minutes after injection of 20 MBq Tc-99m-nanocolloid into the first web spaces of both feet – follow-up study. Arrow indicates popliteal node.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather L Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.