
Abstract
Case history
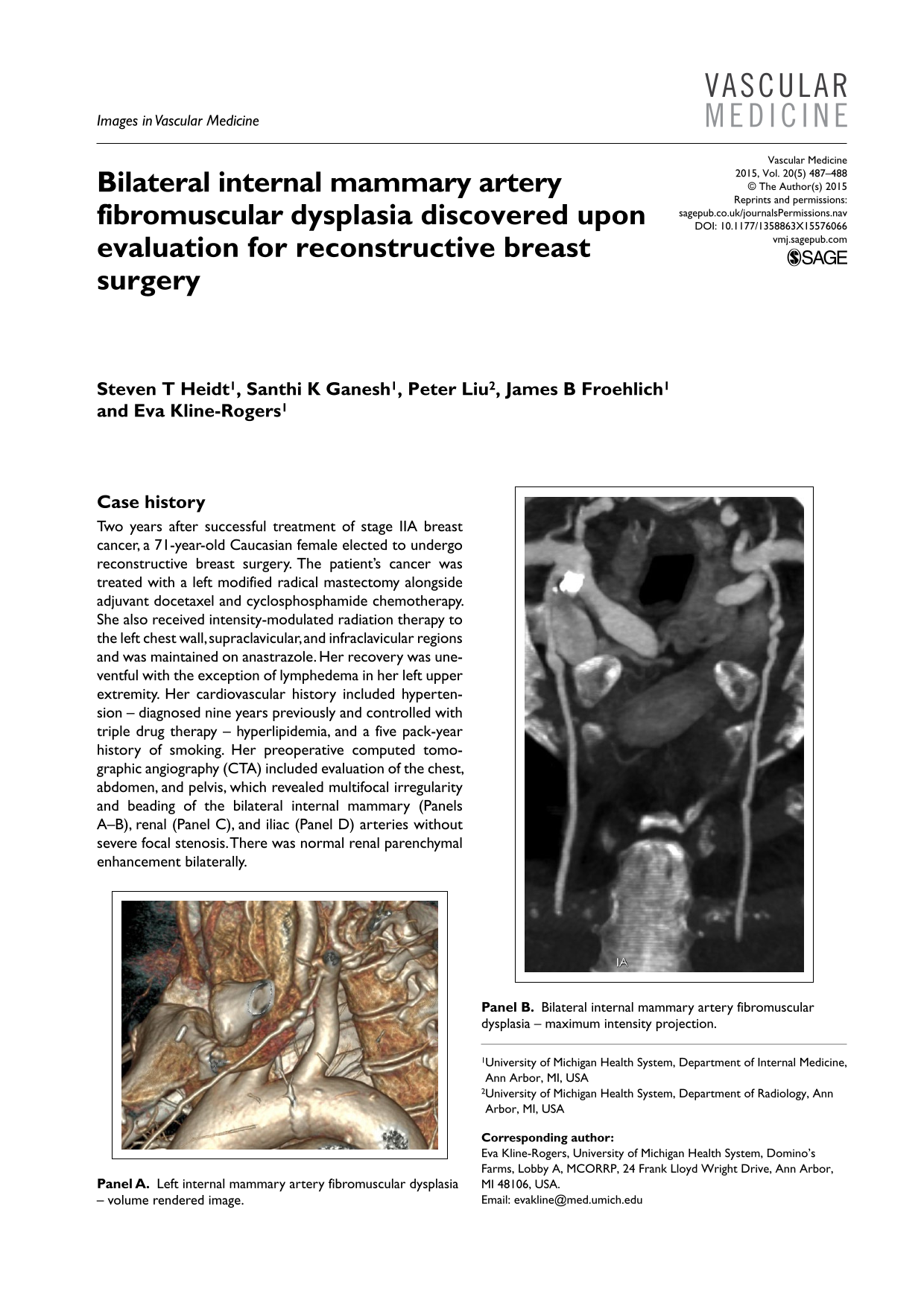
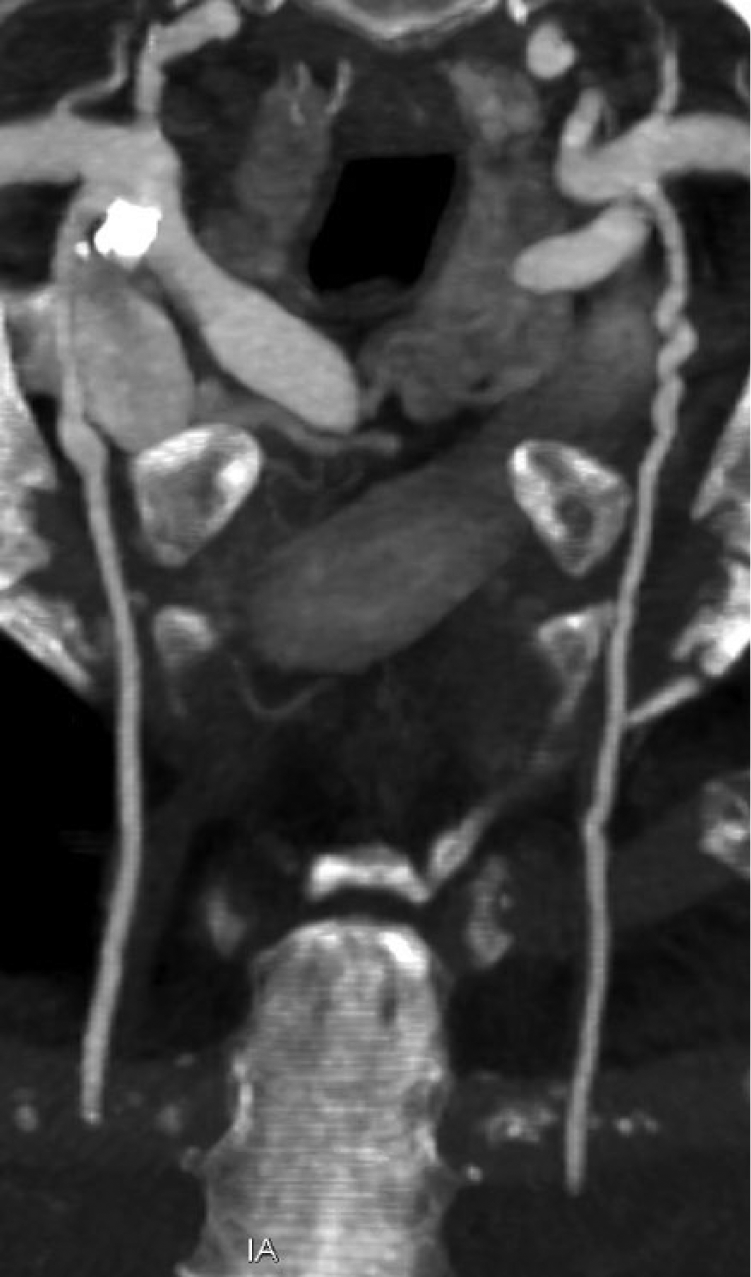
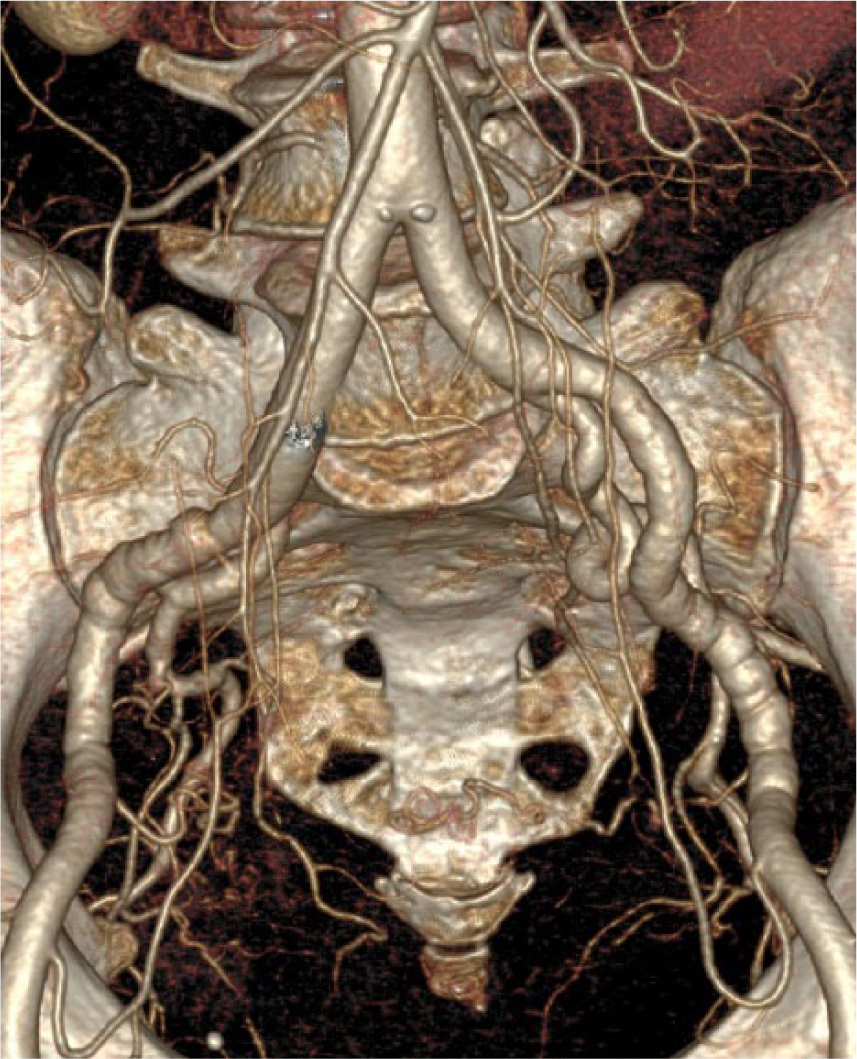
Two years after successful treatment of stage IIA breast cancer, a 71-year-old Caucasian female elected to undergo reconstructive breast surgery. The patient’s cancer was treated with a left modified radical mastectomy alongside adjuvant docetaxel and cyclosphosphamide chemotherapy. She also received intensity-modulated radiation therapy to the left chest wall, supraclavicular, and infraclavicular regions and was maintained on anastrazole. Her recovery was uneventful with the exception of lymphedema in her left upper extremity. Her cardiovascular history included hypertension – diagnosed nine years previously and controlled with triple drug therapy – hyperlipidemia, and a five pack-year history of smoking. Her preoperative computed tomographic angiography (CTA) included evaluation of the chest, abdomen, and pelvis, which revealed multifocal irregularity and beading of the bilateral internal mammary (Panels A–B), renal (Panel C), and iliac (Panel D) arteries without severe focal stenosis. There was normal renal parenchymal enhancement bilaterally.

Left internal mammary artery fibromuscular dysplasia – volume rendered image.
Bilateral internal mammary artery fibromuscular dysplasia – maximum intensity projection.

Bilateral renal artery fibromuscular dysplasia – maximum intensity projection.
Bilateral iliac artery fibromuscular dysplasia – volume rendered image.
Though the disease may only be confirmed histopathologically, 1 physicians believed the patient to have fibromuscular dysplasia (FMD) based on the multifocal beaded appearance of her affected arteries and her longstanding history of hypertension. It should be noted that she was not assessed for an increased C-reactive protein level or erythrocyte sedimentation rate to rule out radiation-induced vasculitis after completing her cancer therapy. However, she had no clinical findings of autoimmune or inflammatory disease and her history of hypertension and the presence of beaded bilateral renal and iliac arteries suggested FMD over vasculitis.
The patient was referred to the vascular surgery and hypertension departments for evaluation of her symptomatic renal FMD. In accordance with current therapeutic guidelines, both departments suggested medical management with low dose aspirin and continuation of her antihypertensive regimen. In order to evaluate possible disease progression, she was scheduled for follow-up renal duplex ultrasound studies to assess for elevated arterial velocities.
FMD within the internal mammary arteries raises specific concerns not associated with other vascular territories. Should this patient require coronary artery bypass grafts in the future, her internal mammary artery FMD must be considered when selecting an arterial conduit, including vessels not imaged, such as radial arteries. A recent study showed that among 50 patients with spontaneous coronary artery dissections, 43 (86%) had FMD in a non-coronary bed. 2 In light of these findings, surgeons may wish to use lower extremity veins as bypass conduits in order to avoid future complications.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather L Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interest
Steven T Heidt has no relevant financial relationships to disclose.
Santhi K Ganesh has no relevant financial relationships to disclose. She is an unpaid medical advisor for the non-profit Fibromuscular Dysplasia Society of America.
Peter Liu has no relevant financial relationships to disclose.
James B Froehlich is a consultant for Pfizer, Sanofi-Aventis, Ortho-McNeil, Boehringer-Ingelheim, and Merck. He receives grant support from Sanofi-Aventis, Blue Cross/Blue Shield of Michigan, Mardigian Foundation, and the Fibromuscular Dysplasia Society of America.
Eva Kline-Rogers is a member of the Advisory Board for the American College of Physicians, and is a member of the Anticoagulation Forum’s Board of Directors.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The patient referenced in this article consented to take part in the United States Registry for Fibromuscular Dysplasia, which is funded by the Fibromuscular Dysplasia Society of America.